
Abstract
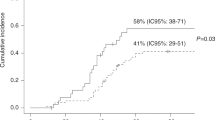
Non-myeloablative (NMA) allogeneic donor SCT for patients with relapsed lymphoma is associated with lower treatment-related mortality (TRM). However, the impact of conditioning intensity on post transplant infections remains unclear. We evaluated infections in 141 consecutive patients with lymphoma who were allografted using NMA (n=76) or myeloablative (MA; n=65) conditioning regimens. Using infection incidence density per 1000 patient days, we accounted for all infectious episodes during the first post transplant year. Before neutrophil engraftment, the NMA cohort had a 53% lower rate of bacterial infection (relative risk=0.47; P=0.06), whereas after engraftment the density of bacterial infections was similar in the two groups. In the first month, both invasive fungal infections and viral infections were twofold less frequent (P=0.22; P=0.06) in NMA patients. Late viral and fungal infections as well as CMV reactivation were infrequent after either conditioning intensity. The 1-year infection-related mortality was significantly lower after NMA conditioning (NMA 9% (3–16%) vs MA 22% (11–40%); P=0.03). NMA allogeneic transplantation for lymphoma patients results in substantially fewer early infections and lower infection-related deaths, although the similar frequency of later infections suggests that immune reconstitution is delayed with either conditioning intensity.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
van Besien K, Loberiza Jr FR, Bajorunaite R, Armitage JO, Bashey A, Burns LJ et al. Comparison of autologous and allogeneic hematopoietic stem cell transplantation for follicular lymphoma. Blood 2003; 102: 3521–3529.
Levine JE, Harris RE, Loberiza Jr FR, Armitage JO, Vose JM, Van Besien K et al. Lymphoma Study Writing Committee, International Bone Marrow Transplant Registry and Autologous Blood and Marrow Transplant Registry. A comparison of allogeneic and autologous bone marrow transplantation for lymphoblastic lymphoma. Blood 2003; 101: 2476–2482.
Peniket AJ, Ruiz de Elvira MC, Taghipour G, Cordonnier C, Gluckman E, de Witte T et al. An EBMT registry matched study of allogeneic stem cell transplants for lymphoma: allogeneic transplantation is associated with a lower relapse rate but a higher procedure-related mortality rate than autologous transplantation. Bone Marrow Transplant 2003; 31: 667–678.
Phillips GL, Reece DE, Barnett MJ, Connors JM, Fay JW, Herzig GP et al. Allogeneic marrow transplantation for refractory Hodgkin's disease. J Clin Oncol 1989; 7: 1039–1045.
Tomblyn MR, Brunstein C, Burns LJ, Miller JS, MacMillan M, DeFor TE et al. Similar and promising outcomes in lymphoma patients treated with myeloablative or non-myeloablative conditioning and allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2008; 14: 538–545.
Sorror ML, Storer BE, Maloney DG, Sandmaier BM, Martin PJ, Storb R . Outcomes after allogeneic hematopoietic cell transplantation with nonmyeloablative or myeloablative conditioning regimens for treatment of lymphoma and chronic lymphocytic leukemia. Blood 2008; 111: 446–452.
Meijer E, Dekker AW, Lokhorst HM, Petersen EJ, Nieuwenhuis HK, Verdonck LF . Low incidence of infectious complications after nonmyeloablative compared with myeloablative allogeneic stem cell transplantation. Transpl Infect Dis 2004; 6: 171–178.
Junghanss C, Marr KA, Carter RA, Sandmaier BM, Maris MB, Maloney DG et al. Incidence and outcome of bacterial and fungal infections following nonmyeloablative compared with myeloablative allogeneic hematopoietic stem cell transplantation: a matched control study. Biol Blood Marrow Transplant 2002; 8: 512–520.
Junghanss C, Boeckh M, Carter RA, Sandmaier BM, Maris MB, Maloney DG et al. Incidence and outcome of cytomegalovirus infections following nonmyeloablative compared with myeloablative allogeneic stem cell transplantation, a matched control study. Blood 2002; 99: 1978–1985.
Khouri IF, Saliba RM, Giralt SA, Lee MS, Okoroji GJ, Hagemeister FB et al. Nonablative allogeneic hematopoietic transplantation as adoptive immunotherapy for indolent lymphoma: low incidence of toxicity, acute graft-versus-host disease, and treatment-related mortality. Blood 2001; 13: 3595–3599.
Bainton RD, Byrne JL, Davy BJ, Russell NH . CMV infection following nonmyeloablative allogeneic stem cell transplantation using Campath. Blood 2002; 100: 3843–3844.
Martino R, Caballero MD, Canals C, San Miguel J, Sierra J, Rovira M et al. Reduced-intensity conditioning reduces the risk of severe infections after allogeneic peripheral blood stem cell transplantation. Bone Marrow Transplant 2001; 28: 341.
Diaconescu R, Flowers CR, Storer B, Sorror ML, Maris MB, Maloney DG et al. Morbidity and mortality with nonmyeloablative compared with myeloablative conditioning before hematopoietic cell transplantation from HLA-matched related donors. Blood 2004; 104: 1550–1558.
Rodriguez R, Nademanee A, Ruel N, Smith E, Krishnan A, Popplewell L et al. Comparison of reduced-intensity and conventional myeloablative regimens for allogeneic transplantation in non-Hodgkin's lymphoma. Biol Blood Marrow Transplant 2006; 12: 1326–1334.
Escalon MP, Champlin RE, Saliba RM, Acholonu SA, Hosing C, Fayad L et al. Nonmyeloablative allogeneic hematopoietic transplantation: a promising salvage therapy for patients with non-Hodgkin's lymphoma whose disease has failed a prior autologous transplantation. J Clin Oncol 2004; 22: 2419–2423.
Van Burik JA, Carter SL, Freifeld AG, High KP, Godder KT, Papanicolaou GA et al. Higher risk of cytomegalovirus and aspergillus infections in recipients of T cell-depleted unrelated bone marrow: analysis of infectious complications in patients treated with T cell depletion versus immunosuppressive therapy to prevent graft-versus-host disease. Biol Blood Marrow Transplant 2007; 13: 1487–1498.
Keung YK, Watkins K, Chen SC, Groshen S, Levine AM, Douer D . Increased incidence of central venous catheter-related infections in bone marrow transplant patients. Am J Clin Oncol 1995; 18: 469–474.
Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J, Crokaert F et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis 2002; 34: 7–14.
Lin DY . Non-parametric inference for cumulative incidence functions in competing risks studies. Stat Med 1997; 16: 901–910.
Peto R, Peto J . Asymptotially efficient rank invariant test procedures. J Royal Soc A 1972; 135: 185–207.
Cox DR . Regression models and life tables. J Royal Soc B 1972; 34: 187–220.
Lin D, Wei L, Yang I, Ying Z . Semiparametric regression for the mean and rate functions of recurrent events. J Royal Soc B 2000; 62: 711–730.
Mohty M, Faucher C, Vey N, Stoppa AM, Viret F, Chabbert I et al. High rate of secondary viral and bacterial infections in patients undergoing allogeneic bone marrow mini-transplantation. Bone Marrow Transplant 2000; 26: 251–255.
Busca A, Lovisone E, Aliberti S, Locatelli F, Serra A, Scaravaglio P et al. Immune reconstitution and early infectious complications following nonmyeloablative hematopoietic stem cell transplantation. Hematology 2003; 8: 303–311.
Chakrabarti S, Mackinnon S, Chopra R, Kottaridis PD, Peggs K, O’Gorman P et al. High incidence of cytomegalovirus infection after nonmyeloablative stem cell transplantation: potential role of Campath-1H in delaying immune reconstitution. Blood 2002; 99: 4357–4363.
Walker CM, van Burik JA, De For TE, Weisdorf DJ . Cytomegalovirus infection after allogeneic transplantation: comparison of cord blood with peripheral blood and marrow graft sources. Biol Blood Marrow Transplant 2007; 13: 1106–1115.
Fukuda T, Boeckh M, Carter RA, Sandmaier BM, Boeckh M, Maris MB et al. Risks and outcomes of invasive fungal infections in recipients of allogeneic hematopoietic stem cell transplants after nonmyeloablative conditioning. Blood 2003; 102: 827–833.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bachanova, V., Brunstein, C., Burns, L. et al. Fewer infections and lower infection-related mortality following non-myeloablative versus myeloablative conditioning for allotransplantation of patients with lymphoma. Bone Marrow Transplant 43, 237–244 (2009). https://doi.org/10.1038/bmt.2008.313
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2008.313
Keywords
This article is cited by
-
Pre-existing invasive fungal infection is not a contraindication for allogeneic HSCT for patients with hematologic malignancies: a CIBMTR study
Bone Marrow Transplantation (2017)
-
Initial fluconazole prophylaxis may not be required in adults with acute leukemia or myelodysplastic/myeloproliferative disorders after reduced intensity conditioning peripheral blood stem cell allogeneic transplantation
Annals of Hematology (2015)
-
Promising Role of Reduced-Toxicity Hematopoietic Stem Cell Transplantation (PART-I)
Stem Cell Reviews and Reports (2012)
-
PCR diagnostics and monitoring of adenoviral infections in hematopoietic stem cell transplantation recipients
Archives of Virology (2010)
-
References
Bone Marrow Transplantation (2009)
