
Summary:
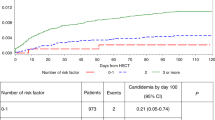
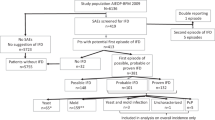
Invasive fungal infections (IFI) are common in allogeneic SCT recipients. We have reviewed our experience of IFI with special reference to candidaemia in 685 adult patients transplanted in 1983–2002. The donor was a matched sibling in 505 patients and an unrelated donor in 180 patients. A BM graft was used in 561 patients and a PB graft in 124 patients. Fluconazole prophylaxis was not used during the study period. Definite or probable IFI was observed in 60 patients (8.7%) with a dominance of Aspergillus infections (46 patients, incidence 6.7%). Candidaemia was found only in nine patients (1.3%). The causative agents were Candida albicans (n=8), C. krusei (n=2), and C. glabrata (n=1); in two patients, two causative agents were found. The median time to the diagnosis of candidaemia was 53 days (range 6–249 days) post transplant. Seven patients were neutropaenic at diagnosis, and four patients had experienced acute GVHD. All patients received antifungal therapy, but only one patient was cured. According to this study, candidaemia was a rare event in allogeneic SCT recipients. Thus, systematic prophylaxis against Candida infections might not be indicated. The prognosis of established infections is still poor due to comorbid conditions, notably GVHD.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Jantunen E, Ruutu P, Niskanen L et al. Incidence and risk factors for invasive fungal infections in allogeneic BMT recipients. Bone Marrow Transplant 1997; 19: 801–808.
Martino R, Subina M, Rovira M et al. Invasive fungal infections after allogeneic peripheral blood stem cell transplantation: incidence and risk factors in 395 patients. Br J Haematol 2002; 116: 475–482.
Morrison VA, Haake RJ, Weisdorf DJ . Non-Candida fungal infections after bone marrow transplantation: risk factors and outcome. Am J Med 1994; 96: 497–503.
Marr KA, Carter RA, Boekh M et al. Invasive aspergillosis in allogeneic stem cell transplant recipients: changes in epidemiology and risk factors. Blood 2002; 100: 4358–4366.
Verfaillie C, Weisdorf D, Haake R et al. Candida infections in bone marrow transplant recipients. Bone Marrow Transplant 1991; 8: 177–184.
Goodrich JM, Reed EC, Mori M et al. Clinical features and analysis of risk factors for invasive candidal infection after marrow transplantation. J Infect Dis 1991; 164: 731–740.
Safdar A, van Rhee F, Henslee-Downey JP et al. Candida glabrata and Candida krusei fungemia after high-risk allogeneic marrow transplantation: no adverse effect of low-dose fluconazole prophylaxis on incidence and outcome. Bone Marrow Transplant 2001; 28: 873–878.
Goodman JL, Winston DJ, Greenfield RA et al. A controlled trial of fluconazole to prevent fungal infections in patients undergoing bone marrow transplantation. N Engl J Med 1992; 326: 845–851.
Slavin MA, Osborne B, Adams R et al. Efficacy and safety of fluconazole prophylaxis for fungal infections after marrow transplantation – a prospective, randomized, double-blind study. J Infect Dis 1995; 171: 1545–1552.
Marr K, Seidel K, Slavin MA et al. Prolonged fluconazole prophylaxis is associated with persistent protection against candiasis-related death in allogeneic marrow transplant recipients: long-term follow-up of a randomized, placebo-controlled trial. Blood 2000; 96: 2055–2061.
Ringden O, Remberger M, Ruutu T, et al, for the Nordic Bone Marrow Transplantation Group. Increased risk of chronic graft-versus-host disease, obstructive bronchiolitis, and alopecia with busulfan versus total body irradiation: long-term results of a randomized trial in allogeneic marrow recipients with leukemia. Blood 1999; 93: 2196–2201.
Ruutu T, Volin L, Parkkali T et al. Cyclosporine, methotrexate, and methylprednisolone compared with cyclosporine and methotrexate for the prevention of graft-versus-host disease in bone marrow transplantation from HLA identical sibling donor: a prospective randomized study. Blood 2000; 96: 2391–2398.
Marr KA, Seidel K, White TC, Bowden RA . Candidemia in allogeneic blood and marrow transplant recipients: evolution of risk factors after the adoption of prophylactic fluconazole. J Infect Dis 2000; 181: 309–316.
Jantunen E, Salonen J, Juvonen E et al. Invasive fungal infections in autologous stem cell transplant recipients: a nation-wide study of 1188 transplanted patients. Eur J Haematol 2004; 73: 174–178.
Edmond MB, Wallace SE, McClish DK et al. Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis 1999; 29: 239–244.
Poikonen E, Lyytikäinen O, Anttila V-J, Ruutu P . Candidemia in Finland, 1995–1999. Emerg Infect Dis 2003; 9: 985–990.
Wingard JR . Fungal infections after bone marrow transplant. Biol Blood Marrow Transplant 1999; 5: 55–68.
de la Rosa GR, Champlin RE, Kontoyiannis DP . Risk factors for the development of invasive fungal infection in allogeneic blood and marrow transplant recipients. Transplant Infect Dis 2002; 4: 3–9.
Marr KA, Crippa F, Leisenring W et al. Itraconazole versus fluconazole for prevention of fungal infections in allogeneic stem cell transplant patients. Blood 2004; 103: 1527–1533.
Herbrecht R, Denning DW, Patterson TF et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002; 347: 408–415.
Bacci A, Montagnoli C, Perruccio K et al. Dendritic cells pulsed with fungal RNA induce protective immunity to Candida albicans in hematopoietic transplantation. J Immunol 2002; 168: 2904–2913.
Acknowledgements
This study was supported by Blood Disease Research Foundation in Finland.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jantunen, E., Nihtinen, A., Volin, L. et al. Candidaemia in allogeneic stem cell transplant recipients: low risk without fluconazole prophylaxis. Bone Marrow Transplant 34, 891–895 (2004). https://doi.org/10.1038/sj.bmt.1704662
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1704662
Keywords
This article is cited by
-
Initial fluconazole prophylaxis may not be required in adults with acute leukemia or myelodysplastic/myeloproliferative disorders after reduced intensity conditioning peripheral blood stem cell allogeneic transplantation
Annals of Hematology (2015)
-
A novel scoring system to predict the incidence of invasive fungal disease in salvage chemotherapies for malignant lymphoma
Annals of Hematology (2014)
-
Epidemiological Characteristics of Fatal Candida krusei Fungemia in Immunocompromised Febrile Neutropenic Children
Infection (2008)
-
The utility of intensified environmental surveillance for pathogenic moulds in a stem cell transplantation ward during construction work to monitor the efficacy of HEPA filtration
Bone Marrow Transplantation (2007)
