
Summary:
Established treatment of severe combined immunodeficiencies (SCID) and other primary immunodeficiencies (PID) is bone marrow transplantation (BMT). Normal lymphocyte numbers and protein antigen responses are present within 2 years of BMT, polysaccharide antibody responses appear last. Streptococcus pneumoniae infection causes significant morbidity and mortality post-BMT. Previous studies have shown good protein antigen responses post-BMT for SCID and PID, but had not examined the polysaccharide responses. We retrospectively analysed pneumococcal polysaccharide (PPS) responses in our patient series.
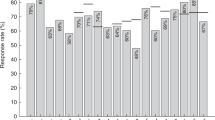
In total, 22 SCID and 12 non-SCID PID were evaluated, all >2 years post BMT: 17 SCID, 12 PID received chemotherapy conditioning; 17 SCID, three PID had T-cell depleted (TCD) BMT, others had nonconditioned whole marrow BMT. All had normal Haemophilus influenza B and tetanus antibody responses. Of 22 SCID, 13 vs 11/12 PID responded to PPS vaccine (P=0.05). There was no association with donor age, GvHD, B-cell chimerism, or IgG2 level. Fewer TCD marrow recipients responded to PPS (P=0.04). Analysis of the SCID group showed no association of PPS response with type of marrow received. This is the first study to specifically examine PPS antibody responses following SCID and PID BMT. Pneumococcal conjugate vaccine antibody responses should be examined in these children.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


References
Ryser O, Morell A, Hitzig WH . Primary immunodeficiencies in Switzerland: first report of the national registry in adults and children. J Clin Immunol 1988; 8: 479–488.
Antoine C, Miller S, Cant AJ et al. Long term survival and hematopoietic stem-cell transplantation for immunodeficiencies: a survey of the European experience (1968–1999). Lancet 2003; 361: 553–560.
Haddad E, Landais P, Friedrich W et al. Long-term immune reconstitution and outcome after HLA-nonidentical T-cell-depleted bone marrow transplantation for severe combined immunodeficiency: a European retrospective study of 116 patients. Blood 1998; 91: 3646–3653.
Fischer A, Landais P, Friedrich W et al. Bone marrow transplantation (BMT) in Europe for primary immunodeficiencies other than severe combined immunodeficiency: a report from the European group for BMT and the European group for immunodeficiency. Blood 1994; 83: 1149–1154.
Gennery AR, Dickinson AM, Brigham K et al. CAMPATH-1 MT cell depleted bone marrow transplantation for severe combined immunodeficiency: long term follow up of 19 children treated in the period 1987–1998 in a single centre. Cytotherapy 2001; 3: 221–232.
Velardi A, Cucciaioni S, Terenzi A et al. Acquisition of Ig isotype diversity after bone marrow transplantation in adults. J Immunol 1988; 141: 815–820.
Avanzini MA, Carra AM, Maccario R et al. Antibody response to pneumococcal vaccine in children receiving bone marrow transplantation. J Clin Immunol 1995; 15: 137–144.
Engelhard D, Cordonnier C, Shaw PJ et al. On behalf of the Infectious Disease Working Party of the European Bone Marrow Transplantation (IDWP-EBMT). Early and late invasive pneumococcal infection following stem cell transplantation: a European Bone Marrow Transplantation survey. Br J Haematol 2002; 117: 444–450.
Haddad E, Le Deist F, Aucouturier P et al. Longterm chimerism and B cell function after bone marrow transplantation in patients with severe combined immunodeficiency with B cells: a single centre study of 22 patients. Blood 1999; 94: 2923–2930.
Peltola H, Kayhty H, Virtanen M, Makela PH . The protective level of serum antibodies to the capsular polysaccharide of Haemophilus influenzae type B. J Infect Dis 1983; 147: 1100.
Griffiths H, Lea J, Bunch C et al. Predictors of infection in chronic lymphocytic leukaemia (CLL). Clin Exp Immunol 1992; 89: 374–377.
Winston JD, Schiffman G, Wang DC et al. Pneumococcal infections after human bone marrow transplantation. Ann Inter Med 1979; 91: 835–841.
Sheridan JF, Tutschka PJ, Sedmak DD, Copelan EA . Immunoglobulin G subclass deficiency and Pneumococcal infection after allogeneic bone marrow transplantation. Blood 1990; 75: 1583–1586.
Giebink GS, Warkentin PI, Ramsay NKC, Kersey JH . Titers of antibody to pneumococci in allogeneic bone marrow transplant recipients before and after vaccination with pneumococcal vaccine. J Infect Dis 1986; 154: 590–596.
Hammarstrom V, Pauksen K, Azinge J et al. Pneumococcal immunity and response to immunization with pneumococcal vaccine in bone marrow transplant patients: the influence of graft versus host reaction. Support Care Cancer 1993; 1: 195–199.
Witherspoon RP, Storb R, Ochs HD et al. Recovery of antibody production in human allogeneic marrow graft recipients: Influence of time posttransplantation, the presence or absence of chronic graft-versus-host disease, and antithymocyte globulin treatment. Blood 1991; 58: 360–368.
Rijkers GT, Sanders LAM, Zegers BJM . Anti-capsular polysaccharide antibody deficiency states. Immunodeficiency 1993; 5: 1–21.
White H, Thrasher A, Veys P et al. Intrinsic defects of B cell function in X-linked severe combined immunodeficiency. Eur J Immunol 2000; 30: 732–737.
Min D, Taylor PA, Panoskaltsis-Mortari A et al. Protection from thymic epithelial cell injury by keratinocyte growth factor: a new approach to improve thymic and peripheral T-cell reconstitution after bone marrow transplantation. Blood 2002; 99: 4592–4600.
Griffioen AW, Toebes EAH, Rijkers GT et al. The amplifier role of T cells in the human in vitro B cell response to type 4 pneumococcal polysaccharide. Immunol Lett 1992; 32: 265–272.
Hale G, Waldmann H . CAMPATH-1 monoclonal antibodies in bone marrow transplantation. J Hematother 1994; 3: 15–31.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Slatter, M., Bhattacharya, A., Flood, T. et al. Polysaccharide antibody responses are impaired post bone marrow transplantation for severe combined immunodeficiency, but not other primary immunodeficiencies. Bone Marrow Transplant 32, 225–229 (2003). https://doi.org/10.1038/sj.bmt.1704109
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1704109
Keywords
This article is cited by
-
Thyroid dysfunction after bone marrow transplantation for primary immunodeficiency without the use of total body irradiation in conditioning
Bone Marrow Transplantation (2004)
