
Summary:
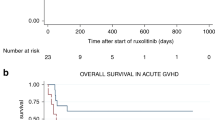
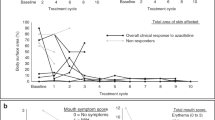
Thalidomide was used to treat acute (n=21) or chronic (n=59) graft-vs-host disease (GVHD) in 80 haematopoietic stem cell allograft recipients after failure to respond to the combination of cyclosporine and corticosteroids with or without other agents. The median time to onset of acute GVHD was 11 days, and thalidomide was started at a median of 48 days post transplant. In addition to corticosteroids and cyclosporine, 13 patients had also received other agents before thalidomide. None of the patients responded and all died of acute GVHD. For chronic GVHD (limited in 13, extensive in 46), thalidomide was started at a median of 385 days post transplant. In addition to corticosteroids and cyclosporine, 34 patients received azathioprine concomitantly. In all patients, thalidomide was added to the ongoing immunosuppressive regimen. The median duration of therapy with thalidomide was 60 days (range, 11–1210; <2 weeks in 11). In total, 13 patients (22%) had complete response, eight (14%) partial response and 38 (64%) no response. Response rates were comparable for limited (39%) and extensive (33%) chronic GVHD. At a median of 53 months, 19 patients are alive, 13 without evidence of chronic GVHD. Survival was significantly better in patients who responded to thalidomide. The principal causes of death were progressive chronic GVHD (n=29) and relapsed leukaemia (n=7). In conclusion, thalidomide has no activity in acute GVHD, but has some activity in chronic GVHD in combination with other agents.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Powles RL, Clink HM, Spence D et al. Cyclosporine A to prevent graft-versus-host disease in man after allogeneic bone-marrow transplantation. Lancet 1980; 1: 327–329.
Sullivan KM, Shulman HM, Storb R et al. Chronic graft-versus-host disease in 52 patients: adverse natural course and successful treatment with combination immunosuppression. Blood 1981; 57: 267–276.
Powles RL, Morgenstern GR, Kay HE et al. Mismatched family donors for bone-marrow transplantation as treatment for acute leukaemia. Lancet 1983; 1: 612–615.
Storb R, Deeg HJ, Whitehead J et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft vs host disease after marrow transplantation for leukaemia. N Engl J Med 1986; 314: 729–735.
Powles R, Mehta J, Kulkarni S et al. Allogeneic blood and bone-marrow stem-cell transplantation in haematological malignant diseases: a randomised trial. Lancet 2000; 355: 1231–1237.
Singhal S, Powles R, Treleaven J et al. Long-term outcome of adult acute leukaemia patients who are alive and well two years after allogeneic bone marrow transplantation from an HLA-identical sibling. Leuk Lymphoma 1999; 34: 287–294.
Kulkarni S, Powles R, Treleaven J et al. Chronic GVHD is associated with long term risk of pneumococcal infections in bone marrow transplant patients. Blood 2000; 95: 3683–3686.
Kulkarni S, Powles R, Treleaven J et al. Melphalan/TBI is not more carcinogenic than cyclophosphamide/TBI for transplant conditioning: follow-up of 725 patients from a single centre over a period of 26 years. Bone Marrow Transplant 2000; 25: 365–370.
Sullivan KM, Witherspoon RP, Storb R et al. Alternating-day cyclosporine and prednisone for treatment of high-risk chronic graft-v-host disease. Blood 1988; 72: 555–561.
Sullivan KM, Witherspoon RP, Storb R et al. Prednisone and azathioprine compared with prednisone and placebo for treatment of chronic graft-v-host disease: prognostic influence of prolonged thrombocytopenia after allogeneic marrow transplantation. Blood 1988; 72: 546–554.
Vogelsang GB . How I treat chronic graft-versus-host disease. Blood 2001; 97: 1196–1201.
Singhal S, Mehta J . Thalidomide in cancer: potential uses and limitations. BioDrugs 2001; 15: 163–172.
Vogelsang GB, Hess AD, Gordon G, Santos GW . Treatment and prevention of acute graft-versus-host disease with thalidomide in a rat model. Transplantation 1986; 41: 644–647.
Lim SH, McWhannell A, Vora AJ et al. Successful treatment with thalidomide of acute graft-versus-host disease after bone-marrow transplantation. Lancet 1988; 1: 117.
Vogelsang GB, Hess AD, Santos GW . Thalidomide for treatment of graft-versus-host disease. Bone Marrow Transplant 1988; 3: 393–398.
McCarthy DM, Kanfer EJ, Barrett AJ . Thalidomide for the therapy of graft-versus-host disease following allogeneic bone marrow transplantation. Biomed Pharmacother 1989; 43: 693–697.
Vogelsang GB, Farmer ER, Hess AD et al. Thalidomide for the treatment of chronic graft-versus-host disease. N Engl J Med 1992; 326: 1055–1058.
Koc S, Leisenring W, Flowers ME et al. Thalidomide for treatment of patients with chronic graft-versus-host disease. Blood 2000; 96: 3995–3996.
Cole CH, Rogers PC, Pritchard S et al. Thalidomide in the management of chronic graft-versus-host disease in children following bone marrow transplantation. Bone Marrow Transplant 1994; 14: 937–942.
Parker PM, Chao N, Nademanee A et al. Thalidomide as salvage therapy for chronic graft-versus-host disease. Blood 1995; 86: 3604–3609.
Rovelli A, Arrigo C, Nesi F et al. The role of thalidomide in the treatment of refractory chronic graft-versus-host disease following bone marrow transplantation in children. Bone Marrow Transplant 1998; 21: 577–581.
Mehta P, Kedar A, Graham-Pole J et al. Thalidomide in children undergoing bone marrow transplantation: series at a single institution and review of the literature. Pediatrics 1999; 103: e44.
Browne PV, Weisdorf DJ, DeFor T et al. Response to thalidomide therapy in refractory chronic graft-versus-host disease. Bone Marrow Transplant 2000; 26: 865–869.
Kulkarni S, Powles R, Mehta J et al. Thalidomide in GVHD–is anti-GVHD effect separable from the antiangiogenesis? Blood 1998; 92 (Suppl. 1): 344b.
Singhal S, Mehta J, Desikan R et al. Antitumor activity of thalidomide in refractory multiple myeloma. N Engl J Med 1999; 341: 1565–1571.
Powles R, Milan S, Horton C et al. The Royal Marsden Hospital leukaemia–myeloma database: an ‘operations research’ resource for assessing clinical outcomes and planning new drug trials. Blood 2001; 98 (Suppl. 1): 426a.
Glucksberg H, Storb R, Fefer A et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974; 18: 295–304.
Sullivan KM, Shulman HM, Storb R et al. Chronic graft-versus-host disease in 52 patients: adverse natural course and successful treatment with combination immunosuppression. Blood 1981; 57: 267–276.
Akpek G, Zahurak M, Piantadosi S et al. Development of a prognostic model for grading chronic graft-versus-host disease. Blood 2001; 97: 1219–1226.
Martin PJ, Schoch G, Fisher L et al. A retrospective analysis of therapy for acute graft-versus-host disease: initial treatment. Blood 1990; 76: 1464–1472.
Mehta J, Powles R, Treleaven J et al. Induction of graft-versus-host disease as immunotherapy of leukaemia relapsing after allogeneic transplantation: single-center experience of 32 adult patients. Bone Marrow Transplant 1997; 20: 129–135.
Singhal S, Powles R, Kulkarni S et al. Long-term follow-up of relapsed acute leukaemia treated with immunotherapy after allogeneic transplantation: the inseparability of graft-versus-host disease and graft-versus-leukaemia, and the problem of extramedullary relapse. Leuk Lymphoma 1999; 32: 505–512.
Corral LG, Kaplan G . Immunomodulation by thalidomide and thalidomide analogues. Ann Rheum Dis 1999; 58 (Suppl. 1): I107–I113.
Chao NJ, Parker PM, Niland JC et al. Paradoxical effect of thalidomide prophylaxis on chronic graft-versus-host disease. Biol Blood Marrow Transplant 1996; 2: 86–92.
Forsyth CJ, Cremer PD, Torzillo P et al. Thalidomide responsive chronic pulmonary GVHD. Bone Marrow Transplant 1996; 17: 291–293.
Vacca A, Singhal S, Ribatti D, Dammacco F . Angiogenesis in plasma cell disorders. In: Mehta J, Singhal S (eds). Myeloma. Martin Dunitz: London, 2002.
Acknowledgements
This study was supported by the Bud Flanagan Leukaemia Fund, the David Adams Leukaemia Fund, the Cancer Research Campaign and the Institute of Cancer Research.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kulkarni, S., Powles, R., Sirohi, B. et al. Thalidomide after allogeneic haematopoietic stem cell transplantation: activity in chronic but not in acute graft-versus-host disease. Bone Marrow Transplant 32, 165–170 (2003). https://doi.org/10.1038/sj.bmt.1704033
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1704033
Keywords
This article is cited by
-
Phase-1/-2 study of pomalidomide in chronic GvHD
Bone Marrow Transplantation (2016)
-
Chronic GVHD: Where are we? Where do we want to be? Will immunomodulatory drugs help?
Bone Marrow Transplantation (2013)
-
Therapeutic effects of thalidomide in hematologic disorders: a review
Frontiers of Medicine (2013)
-
Bronchiolitis obliterans after allo-SCT: clinical criteria and treatment options
Bone Marrow Transplantation (2012)
-
Targeted treatments to improve stem cell outcome: old and new drugs
Bone Marrow Transplantation (2007)
