
Abstract
Objective:
Goiter is endemic in Iran. The iodine deficiency disorders program was begun a few years ago in Iran, and the coverage of iodized salt is sufficient now. But, in a periodic yearly medical examination of primary school girls in Qom, the prevalence of goiter was above 30% in 2002. This survey was designed to study the risk factors of goiter in those students.
Design:
The study was a randomized (multistage, proportional simple random sampling) case–control study.
Subjects and interventions:
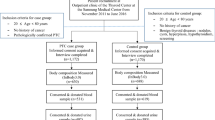
We selected and performed thyroid examinations in 1050 girl students in primary schools in Qom city of Iran in 2002. We found 284 cases: girls in primary schools had goiter in accordance with the clinical exam of World Health Organization classification. Among students who did not present with goiter in the clinical exam, we randomly selected 288 students as the control group. We used a questionnaire to evaluate them for the risk factors of goiter.
Results:
The mean±s.d. ages of cases and controls were 8.7±1.3 and 8.9±1.3 years, respectively. There is no significant difference between the two groups regarding history of soya, kale, turnip, fish, daily iodized salt usage, education and job of mothers, monthly family income, nationality, immigration and residential situation. By using multinomial logistic regression, we found that storage of iodized salt in open containers, odds ratio (OR): 2.201 (1.412–3.428); P-value <0.0001, medium socioeconomic situation (SES) of family, OR: 2.099 (1.029–4.282), P-value=0.041, district 2 of Qom city, OR: 2.880 (1.376–6.027), P-value=0.005, and district 3 of Qom city, OR: 2.051(1.032–4.078), P-value=0.041, were the major risk factors for goiter in this population.
Conclusions:
In this study, the main risk factors for goiter were storage of iodized salt in open containers, medium SES and also living in specific districts of Qom city. As the coverage of iodinized salt is over 95% in Iran, we advise the education of the family about storage of iodized salt in closed containers. We also recommend the study of the other risk factors of goiter in the different geographical areas of Iran, because of differences in the SES and nutritional habits.
Sponsorship:
This study was supported by issuing permission letters for our activities: (not funding support) Qom Health Network and Medical Services, Qom Medical University, Qom Primary School Education Office, Fathemieh Medical University.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Adou P, Aka D, Ake M, Koffi M, Tebi A, Diarra-Nama AJ (2002). Assessment of iodine content of dietary salt in Abidjan (Cote d'Ivoire) Sante 12, 18–21.
Aminorroaya A, Amini M, Rezvanian H, Kachoie A, Sadri G, Mirdamadi M et al. (2001). Effects of iodized salt consumption on goiter prevalence in Isfahan: the possible role of goitrogens. Endocr Pract 7, 95–98.
Aminorroaya A, Rohani S, Sattari G, Haghighi S, Amini M (2004). Iodine repletion, thyrotoxicosis and atrial fibrillation in Isfahan, Iran. Ann Saudi Med 24, 13–17.
Aydin K, Kendirci M, Kurtoglu S, Karakucuk EI, Kiris A (2002). Iodine and selenium deficiency in school-children in an endemic goiter area in Turkey. J Pediatr Endocrinol Metab 15, 1027–1031.
Azizi F, Hedayati M, Rahmani M, Sheikholeslam R, Allahverdian S, Salarkia N (2005). Reappraisal of the risk of iodine-induced hyperthyroidism: an epidemiological population survey. J Endocrinol Invest 28, 23–29.
Azizi F, Mirmiran P, Sheikholeslam R, Hedayati M, Rastmanesh R (2002). The relation between serum ferritin and goiter, urinary iodine and thyroid hormone concentration. Int J Vitam Nutr Res 72, 296–299.
Azizi F, Navai L, Fattahi F (2002). Goiter prevalence, urinary iodine excretion, thyroid function and anti-thyroid function and anti-thyroid antibodies after 12 years of salt iodization in Shahriar, Iran. Int J Vitam Nutr Res 72, 291–295.
Azizi F, Rahmani M, Allahverdian S, Hedayati M (2001a). Effects of salted food consumption on urinary iodine and thyroid function tests in two provinces in the Islamic Republic of Iran. East Mediterr Health J 7, 115–120.
Azizi F, Shaikholeslam R, Hedayati M, Mirmiran P (2001b). Goiter and urinary iodine in Iranian school children. Teb-va-Tazkiyeh 40, 44–51.
Azizi F, Sheikholeslam R, Hedayati M, Mirmiran P (2001c). Monitoring of goiter and urinary iodine in primary students of Lorestan province. Lorestan Univ Health Med J 8, 49–53.
Biber FZ, Unak P, Yurt F (2002). Stability of iodine content in iodized salt. Isotopes Environ Health Stud 38, 87–93.
Deshad H, Satari M, Monsef A (1998). Thyroid single nodule in Hamadan province. Sci J Hamadan Univ 11, 5–9.
Emami A, Shahbazi H, Sbzevari M et al. (1969). Goiter in Iran. Am J Clin Nutr 22, 1584.
Ghamie S (1997). Prevalence study of goiter in 11–14 years old school girls in Shiraz, Iran. MS Thesis, School of Medicine, Shiraz University of Medical Sciences (unpublished data).
Hess SY, Zimmermann MB, Adou P, Torresani T, Hurrell RF (2002). Treatment of iron deficiency in goitrous children improves the efficacy of iodized salt in Cote d'Ivoire. Am J Clin Nutr 75, 743–748.
Hetzel BS (1993). The control of iodine deficiency. Am J Public Health 83, 494–495.
ICCIDD/UNICEF/WHO (1990). A Practical Guide to the Correction of Iodine Deficiency. Manual No. 3.
IDD Key Messages Generic Tool Kit 4. http://www.tulane.edu/~icec/iddcommguidetk4.htm.
IDD News letter (1996) Vol. 12, No. 4, November.http://www.people.virginia.edu/~jtd/iccidd/newsletter/idd1196.htm.
Iran Epidemiological Data – Iodine. http://www.tulane.edu/~internut/Countries/Iran/iraniodine.html.
Janghah A (1997). Prevalence study of IDD among primary school girls in Shiraz, Iran. Pediatric Thesis (Persian), School of Medicine, Shiraz University of Medical Sciences (unpublished data).
Kimiagar M, Azizi F, Navai L, Yassai M, Nafarabadi T (1990). Survey of iodine deficiency in a rural area near Tehran: association of food intake and endemic goitre. Eur J Clin Nutr 44, 17–22.
Mirmiran P, Hajipour R, Azizi F (2003). Iodized salt consumption maintains euthyroidism in iodine-deficient hypothyroid subjects. Int J Vitam Nutr Res 73, 187–191.
Mirmiran P, Kimiagar M, Azizi F (2002). Three-year survey of effects of iodized oil injection in schoolchildren with iodine deficiency disorders. Exp Clin Endocrinol Diabetes 110, 393–397.
Navaei L, Kimiagar M, Azizi F (1986). Epidemiology of goiter in Shahriyar. Med J Shaheed Beheshti Univ Health Med Serv 10, 8–11.
Noorbala A, Mohammad K, Malekafzali H, Majdzadeh SR, Karimloo M, Mirjafari Firoozabadi SJ et al. (2000). Health and Disease Survey in Iran. Ministry of Health, National Medical Research Center: Iran, pp 104–105.
Nouarie M, Pourshams A, Kamangar F, Sotoudeh M, Derakhshan MH, Akbari MR et al. (2004). Ecologic study of serum selenium and upper gastrointestinal cancers in Iran. World J Gastroenterol 10, 2544–2546.
Punia D, Yadav SK, Gupta M, Khetarpaul N (2002). Note: storage practices, salt intake and iodine content of salt consumed in rural households of Haryana State, North India. Nutr Health 16, 337–342.
Rajabian R, Abdinegad A, Praizadeh J, Shahbazi H, Sayadpoor K, Abdolsalami HR (1996). IDD in Mashhad and Neishboor. Iran J Med Assoc 15, 25–30.
Raie RM (1996). Regional variation in As, Cu, Hg, and Se and interaction between them. Ecotoxicol Environ Saf 35, 248–252.
Ravanshad Sh, Setoudeh Maram E, Nader F, Mostafavy H (2003). Prevalence study of iodine deficiency disorders among high school girls in Shiraz, Islamic Republic of Iran, 1996–1997. Pak J Med Sci 19, 70–74.
Salarkia N, Hedayati M, Mirmiran P, Kimiagar M, Azizi F (2003). Evaluation of the impact of an iodine supplementation programme on severely iodine-deficient schoolchildren with hypothyroidism. Public Health Nutr 6, 529–533.
Sheikholeslam R, Azizi F (1992). Prevention of iodine deficiency disorders. A report about IDD activities in Iran. Daroo Darman J 9, 29–32.
Sheikholeslam R, Sadvandian S (1993). Iodine Deficiency Disorders for Health Worker Education. Nutrition, Health and Family Planning Office, Ministry of Health and Medical Education: Iran, pp 36–37.
Taga I, Massouke DD, Ndomou M, Yonkeu JN (2004). Iodized salt in Cameroon. Sante 14, 161–165.
World Health Organization Document (1994). Indictors for Assessing Iodine Deficiency Disorders and Their Control Through Salt Iodization. World Health Organization: Geneva. (document no. WHO/NUT/94.6).
Yavuz O, Yavuz T, Kahraman C, Yesildal N, Bundak R (2004). The relationship between iron status and thyroid hormones in adolescents living in an iodine deficient area. J Pediatr Endocrinol Metab 17, 1443–1449.
Zahedi AS, Saboor H, Poorseraj S (1995). A hyper endemic region for goiter in Khozestan province. Med J Shaheed Beheshti Univ Health Med Serv 19, 35–41.
Zali MR, Mohammad K, Azam K, Masgedi MR (1994). Thyroid situation in Iran according to Health and Disease Survey – 1990. Iranian J Med Assoc 13, 113–122.
Zimmermann MB, Zeder C, Chaouki N, Torresani T, Saad A, Hurrell RF (2002). Addition of microencapsulated iron to iodized salt improves the efficacy of iodine in goitrous, iron-deficient children: a randomized, double-blind, controlled trial. Eur J Endocrinol 147, 747–753.
Acknowledgements
This study had been supported by permission letters for our activities (not funding support) from Qom Health Network and Medical Services, Qom Medical University and Qom Primary School Education Office, Fathemieh Medical University. We wish to thank the anonymous reviewers of the journal for their helpful comments on previous versions of the manuscript, and Ms Zinat Sadat Mousavi for her comments on correcting the English text of this article, Ms Somayeh Asbaghi Namini for the kind attention and many practical comments about the nutrition items of the article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Guarantor: SM Mousavi. Contributors: SMM, NT, and FM.
Rights and permissions
About this article
Cite this article
Mousavi, S., Tavakoli, N. & Mardan, F. Risk factors for goiter in primary school girls in Qom city of Iran. Eur J Clin Nutr 60, 426–433 (2006). https://doi.org/10.1038/sj.ejcn.1602335
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1602335
Keywords
This article is cited by
-
Iodine deficiency and associated factors among school children: a cross-sectional study in Ethiopia
Archives of Public Health (2016)
-
Iodine nutritional status and risk factors for goitre among schoolchildren in South Tajikistan
BMC Endocrine Disorders (2013)
