
Abstract
Currently, the relationship between household size and incident dementia, along with the underlying neurobiological mechanisms, remains unclear. This prospective cohort study was based on UK Biobank participants aged ≥ 50 years without a history of dementia. The linear and non-linear longitudinal association was assessed using Cox proportional hazards regression and restricted cubic spline models. Additionally, the potential mechanisms driven by brain structures were investigated by linear regression models. We included 275,629 participants (mean age at baseline 60.45 years [SD 5.39]). Over a mean follow-up of 9.5 years, 6031 individuals developed all-cause dementia. Multivariable analyses revealed that smaller household size was associated with an increased risk of all-cause dementia (HR, 1.06; 95% CI 1.02–1.09), vascular dementia (HR, 1.08; 95% CI 1.01–1.15), and non-Alzheimer’s disease non-vascular dementia (HR, 1.09; 95% CI 1.03–1.14). No significant association was observed for Alzheimer’s disease. Restricted cubic splines demonstrated a reversed J-shaped relationship between household size and all-cause and cause-specific dementia. Additionally, substantial associations existed between household size and brain structures. Our findings suggest that small household size is a risk factor for dementia. Additionally, brain structural differences related to household size support these associations. Household size may thus be a potential modifiable risk factor for dementia.
Similar content being viewed by others


Introduction
Dementia is a major and severe public health issue that greatly reduces the health-related quality of life, significantly increases the mortality rate, and poses a tremendous social and economic burden1. The dementia diagnosis rate in England was 64.6% in December 2023. By 2050, the global prevalence of dementia will soar to 150 million cases2. Given that modifiable risk factors accounting for approximately 40% of dementia cases, addressing these preventable risk factors has become a crucial priority in alleviating the global burden of dementia2,3.
Household size is increasingly recognized as a crucial social factor related to social networks, lifestyles, and socioeconomic characteristics4,5. Although previous research has reported an association between living alone and dementia6,7, the influence of household size on dementia incidence remains unclear. One cross-sectional study found that large household size was associated with a lower risk of dementia8. However, this study had limitations, including a small sample size, regional focus (limited to inhabitants of eastern Uttar Pradesh, India), and lack of long-term follow-up. To address this gap, a large population-based prospective cohort study is needed to examine whether household size is associated with the risk of dementia.
Moreover, little is known about the imaging biomarkers underlying the association of household size with dementia and preclinical changes in brain structure, which may reflect the cognitive benefits of living with large household size9,10. Previous studies have demonstrated the potential effects of living alone on the brain and white matter hyperintensity (WMH) volumes derived from magnetic resonance imaging (MRI)11,12. However, the associations of household size with total and regional brain volumes, WMH volumes, and white matter microstructure require further investigation. Recently, MRI modalities have been widely used to identify biomarkers for neurodegenerative diseases such as Alzheimer’s disease (AD) and age-related cognitive decline10,13. These pathology MRI biomarkers could be used to improve diagnostic sensitivity and accuracy, and might lead to novel molecular-based treatment interventions14. Therefore, identifying the factors that affect MRI indices related to cognitive function is crucial.
With this background, we aimed to explore the associations of household size with incident dementia after controlling for various confounders such as biological, social, and psychological factors. We utilized data from the extensive UK Biobank cohort. Additionally, we examined the impact of household size on neuroanatomical indices to uncover underlying mechanisms related to dementia risk.
Methods
Participants
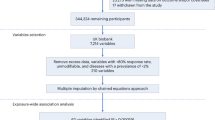
The UK Biobank is a health-oriented, population-based prospective cohort study that recruited more than 500,000 participants aged between 40 and 69 years from 2006 to 2010 in the UK15. Ethical approvals of the UK Biobank were obtained from the National Information Governance Board for Health and Social Care and the North West Multi-Centre Research Ethics Committee16. All research was performed in accordance with the relevant guidelines and regulations. This study was approved under the UK Biobank application number 94885. For our analysis, we included participants who attended a baseline assessment center visit and excluded those with missing exposure variable data (specifically, responses such as “Do not know” or “Prefer not to answer” regarding household size) (n = 4549), a history of dementia (n = 283), without confounder data (n = 57,716), < 50 years old (n = 101,026), or without data of follow-up (n = 63,284). These exclusions resulted in a study sample of 275,629 participants. Neuro-imaging analyses were performed in 40,645 participants with quality-controlled MRI data and complete confounder information. The flowchart of the cohort and the study design is shown in Figure S1.
Exposures
Information regarding household size was obtained from the Touchscreen questionnaire. Number in household was collected via a self-report question: “Including yourself, how many people are living together in your household? (Include those who usually live in the house such as students living away from home during term, partners in the armed forces or professions such as pilots)”. Responses falling below 1 or exceeding 100 were rejected. If a participant’s answer exceeded 12, they were prompted to confirm their response. In the primary analysis, we treated the number of individuals in the household as a continuous variable. In sensitivity analyses, we classified participants with the number of household = 1 as living alone (0) and those with the number of household > 1 as living with someone (1).
Dementia diagnosis
The outcome of interest in this study was all-cause and cause-specific dementia, which were obtained from algorithmically (Category 47) defined outcomes in UK Biobank datasets. The International Classification of Diseases 10th revision (ICD-10) codes F00, F01, F02, F03, G30, G31, and ICD-9 were used to identify participants with incident dementia if any of these codes were recorded as a primary or secondary diagnosis in the health records. AD was identified by ICD-10 codes F00, G30, and ICD-9 code 290; vascular dementia (VD) was identified by ICD-10 code F01; and non-Alzheimer’s disease non-vascular (non-AD non-VD) dementia was identified by ICD-10 codes F02, F03, F05, F10, G31. Follow-up visits extended from the initial attendance at the assessment center until the earliest date of dementia diagnosis, death, or the last available date from the hospital inpatient data as of January 2022.
Brain imaging data
For this study, the brain imaging information was obtained from three dedicated, identical imaging centers. Details of MRI acquisition protocol are available online17. All structural MRI data were preprocessed using a standard Siemens Skyra 3 T running VD13A SP4, with a standard Siemens 32-channel RF receive head coil, and quality-checked these data18. All images were subjected to nonlinear modulations and normalized for each individual head size19,20. Images were then smoothed with an 8 mm full width at half maximum Gaussian kernel with a resulting voxel size of 1.5 mm3. In this study, we focused our analyses on brain volume, WMH, white matter microstructure, cortical, and subcortical regions excluding the cerebellum.
Covariates
The covariates for this analysis were selected based on previous literature and availability at baseline21,22. Sociodemographic factors included age, sex, ethnicity (White, Asian or Asian British, Black or Black British, other), educational level (≤ 10, 11–12, > 12 years), and socioeconomic status (SES). SES was measured by the Townsend deprivation index (TDI) representing area level deprivation categorized into 4 quintiles. Lifestyle factors were obtained by self-reported questions: smoking status (never, former, current smoking), alcohol intake (daily or almost daily, 3–4, 1–2 times/week, occasionally, never), and physical activity level (low, moderate, high). Biological factors comprised body mass index (BMI) (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30.0 kg/m2)23, APOE genotype (non-ε4-carrier, one-ε4-carrier, two-ε4-carrier)24,25, diabetes, stroke and high blood pressure. Depressed mood (not at all, several days, more than half the days, nearly every day) was tested using a self-reported question: “Over the past 2 weeks, how often have you felt down, depressed, or hopeless?”. Social isolation was quantified by three questions: number of people living together in the household (1 point if living alone), frequency of visits to or by friends or family (1 point if friends/family visits less than once a month), and engagement in leisure or social activities (1 point if no participation at least weekly)15. Participants with a total score of 2 or 3 were classified as with social isolation, while those with a total score of 0 or 1 were not. Detailed information on covariate definitions and collection is given in the appendix (Table 1).
Statistical analysis
Cox proportional hazard model
The Cox proportional hazards model was used to estimate the hazard ratios (HRs) and confidence intervals (CIs) for the relation of household size to incident dementia. The primary analyses were aimed to assess the relation of household size to all-cause dementia, followed by separate analyses with dementia subtypes of AD, VD, and non-AD non-VD dementia. We adjusted the models in several steps. Model 1 was adjusted for age. Model 2 was further adjusted for sex, ethnicity, APOE allele status, and education. Model 3 included Model 2 additionally adjusted for smoking status, alcohol intake, physical activity, BMI, and TDI. Model 4 was additionally adjusted for hypertension status, diabetes status, stroke history, and depressive symptoms, besides covariates in Model 3. Restricted cubic spline curves based on Cox analysis were used to investigate the potential of non-linearity, adjusted for covariates as in Model 4. In subgroup analysis, we examined the interaction between household size and different strata factors. We used the likelihood ratio test for multiplicative interaction analysis. If the p-value associated with the interaction term is < 0.05, we conclude that the interaction effect is significant. We performed stratified analyses to estimate potential modification effects according to age (≥ 65, < 65 years), TDI (Q1, Q2, Q3, Q4), smoking status (never, previous, current), and education level (≤ 10, 11–12, > 12 years). Several sensitivity analyses were conducted to analyze the robustness of our findings. Firstly, we additionally adjusted for social isolation in Model 4, since social isolation is a risk factor for dementia21. Secondly, we repeated the analyses among the participants without stroke history. Thirdly, we only included dementia events that occurred at least 5 years after baseline to minimize the influence of reverse causation as suggested by previous studies26,27,28. Finally, we classified participants as living alone and living with someone.
Brain imaging analysis
We employed linear regression models to explore the cross-sectional relationship between household size and brain morphometric measures. Our covariate adjustments followed the same approach as in Model 4. Two sensitivity analyses were performed: (1) classifying participants as living alone and living with someone; (2) excluding participants with nervous system disorders (e.g., dementia, stroke, brain surgery, multiple sclerosis, encephalitis, myelitis, encephalomyelitis, intracranial and intraspinal abscess and granuloma, acute disseminated demyelination and other demyelinating diseases of central nervous system) (n = 8,907). Owing to the number of statistical tests we performed, a Bonferroni correction for multiple testing was applied29. 21 independent brain MRI indices were tested. Therefore, the significance level P = 0.05 was divided by 21, which provides a significance level corrected for multiple testing: P = 0.002430.
All statistical analyses were conducted using SPSS 23 and R (version 4.2.3). All P values listed below were adjusted.
Informed consent
The participants of this study were from the UK biobank database. All participants gave informed consent through electronic signature before joining the UK biobank research project.
Results
Participant characteristics
Table 2 shows the baseline characteristics of the 275,629 dementia-free participants in the primary analyses. The mean (SD) age of participants was 60.45 (5.39) years and the average (SD) number in household was 2.20 (1.15). Women accounted for 52.63% of the sample. During a mean follow-up time of 9.50 years, 6,031 (2.19%) incidences developed all-cause dementia, including 2,565 cases of AD, 1,347 cases of VD, and 2,414 cases of non-AD non-VD dementia. At the imaging visit, 40,645 individuals without outliers were included, in which they had a mean (SD) age and household size of 55.97 (7.52) years and 2.55 (1.21), respectively. Women made up 52.43% of this subgroup.
Household size and dementia risk
In the unadjusted model, the HR for the incidence of all-cause dementia was 0.76 (95% CI, 0.74–0.79) for larger household size compared with small household size. However, after adjusting for various risk factors, this association was attenuated. The overall HR, accounting for all covariates, was 0.95 (95% CI, 0.92–0.98) (Table 3). The results for AD showed no significant association with household size in fully adjusted models. The results for VD and non-AD non-VD dementia showed consistent trends with those for all-cause dementia, that is, the risk of VD (HR, 0.93; 95% CI, 0.87–0.99) and non-AD non-VD dementia (HR, 0.92; 95% CI, 0.88–0.97) decreased with the increasing number of people in household in fully adjusted models (Table 3). The restricted cubic spline models revealed a reversed J-shaped association between household size and the risk of all-cause dementia, VD, and non-AD non-VD dementia. The lowest risk occurred at approximately 4 individuals in the household, after which the risk plateaued (Figure S2).
We observed multiplicative interactions between household size and several factors in relation to the risk of all-cause dementia (Fig. 1). The association between household size and dementia risk was significant in older individuals (in ≥ 65 years: HR 0.93 [95% CI, 0.89–0.97]) and more TDI deprived groups (in Q3: HR 0.90 [95% CI, 0.84–0.96]; in Q4: HR 0.93 [95% CI, 0.88–0.97]). In the never smoking (HR, 0.96; 95% CI, 0.92–0.99) and previous smoking (HR, 0.94; 95% CI, 0.89–0.99) groups, the association was significant. Furthermore, the association was significant for individuals with in the education ≤ 10 years (HR, 0.92; 95% CI, 0.87–0.97) and > 12 years (HR, 0.95; 95% CI, 0.90–0.99). The associations of household size with VD and non-AD non-VD dementia did not appreciably vary between subgroups. In most subgroup analyses, there is sufficient statistical power to detect effects (Figure S3).

Associations of household size with all-cause and cause-specific dementia by age, TDI, smoking status, and education level. TDI, Townsend deprivation index; CI, confidence interval; HR, hazard ratio. In each model, potential confounders the same as Model 4 in Table 2 were adjusted.
In sensitivity analysis, we excluded participants who had a history of stroke (n = 5,315) or those who developed dementia within 5 years (n = 536) of baseline assessment. Remarkably, the results remained consistent with the main analyses (Table S1 and Table S2). Additionally, when we further adjusted for social isolation in Model 4, the patterns of results remained similar (Table S3). After classifying participants as living alone and living with someone, the effects of living situation on dementia risk were even stronger (fully-adjusted HR 0.85; 95% CI 0.81–0.92) (Table S4).
Associations of household size with brain structure
Whole-brain analyses revealed that total brain (grey and white) volume, total grey volume (GM), and the volumes of subcortical regions such as the thalamus, and accumbens were positively associated with household size (Table 4). WMH volume and white matter tract integrity indices (mean diffusivity [MD]) were negatively associated with household size. These findings remained robust when participants were classified as living alone or living with someone, and when patients with nervous system disorders were excluded.
Discussion
In this 9.5-year follow-up study of 275,629 UK Biobank participants, we found that small household size was associated with a higher risk of all-cause dementia, VD, and non-AD non-VD dementia. Additionally, smaller household size correlated with increased WMH load and reduced GMVs in brain regions related to learning and memory, which might partly mediate the relationship between household size and cognitive function. These findings underscore the potential impact of household size on dementia risk.
To our knowledge, this is the first large-scale longitudinal cohort study controlling for various risk factors to investigate the associations between household size and dementia risk. Consistent with a previous cross-sectional study8, we found that small household size was associated with a 1.05-fold increased risk of developing dementia. Our results also revealed strong associations between household size and specific dementia subtypes: VD and non-AD non-VD. Notably, the risk reduction associated with larger household size was more pronounced for non-AD non-VD dementia than for VD. Interestingly, we observed a reverse J-shaped association between household size and dementia risk. Specifically, as the number of household members decreased, the risk of dementia increased. However, beyond a certain threshold (approximately 4 individuals), further increases in household size did not provide additional protection against dementia. This nuanced relationship highlights the complex interplay between social networks, socioeconomic status, household size, and cognitive health31. Consistent with previous population-based studies, our study reaffirms that living alone is a risk factor for dementia32,33.
We first identified multiple brain regions associated with household size in the largest sample to date. In the UK Biobank, participants with small household sizes had higher WMH volumes, reduced white matter tract integrity, and lower GMVs in several regions, including frontal pole, temporal cortex, angular gyrus, thalamus, precuneus cortex, putamen, and accumbens. Higher WMH volumes are a key predictive marker of cognitive decline progression34,35. Decreased FA and increased MD and ISOVF are associated with memory and executive dysfunction36. The frontal pole, temporal cortex, and other subcortical volume reductions are involved in cognitive functions, emotional processing, and social perception37.
The potential mechanisms linking household size with dementia may be elucidated by the following information. Living with others provides a persistent companionship and engagement, whereas living alone is a reliable proxy for social isolation15,21. Cognitive reserve theory suggests that lacking day-to-day companionship and social isolation may reduce mental stimulation and weaken neural connectivity, potentially leading to cognitive decline38,39. In addition, social isolation resulting from small household sizes may lead to stress responses, including chronic HPA axis hyperactivity and inflammation, both associated with an increased dementia risk40. Moreover, cognitive impairment often lead to increased social isolation, as individuals with declining cognitive abilities exhibit behavioral changes and a tendency to withdraw.
The following issues should be taken into account when interpreting our findings. Firstly, it’s worth noting that participants in the UK Biobank study were predominantly female, reported fewer health conditions, and tended to reside in less socioeconomically deprived areas compared to the broader population41. While previous research suggests that the lack of representativeness may not significantly affect the generalizability of exposure-mortality relationships42, the potential impact of selection bias on the associations between household size and dementia risk remains uncertain. Secondly, relying on participants’ health-related records to identify dementia cases in the UK Biobank study could introduce misclassification bias, particularly for early or mild dementia. Nevertheless, it’s important to note that this method demonstrated a relatively high positive predictive value (82.5%) for all-cause dementia43. Thirdly, the neuroimaging analyses included a population-based sample of participants, with only 10 cases of incident dementia. Consequently, the observed associations between household size, WMH, reduced white matter tract integrity, and GMVs were not directly linked to dementia incidence in our current study. Additionally, there is a time gap of 9.43 ± 2.01 years between the imaging data and baseline characteristics information for participants in the image analysis. Over time, changing confounding factors may influence the results. Fourthly, our study did not consider cultural factors that could impact household size and behavior38. Notably, individualistic cultures tend to exhibit a higher prevalence of individuals living alone and a lower frequency of marriage and childbearing. Fifthly, although plasma proteins can predict dementia risk up to 10 years in advance, the impact of dementia latent period on the associations between household size and dementia remains uncertain due to our lack of participant predictions44. Furthermore, among individuals who live alone or have limited support from relatives, the clinical manifestations of dementia may be more pronounced, especially if these relatives are of the same generation and have limitations in their caregiving functions. Therefore, the estimated prevalence of dementia within this population may be overestimated. Additionally, due to the limited availability of data on time-varying variables, we were unable to account for time-varying confounders in our study. This limitation is common in most cohort studies22. Moreover, if household size changed over time (with older adults having fewer family members)45, our observed association between household size and dementia risk might have been underestimated. Specifically, living alone could potentially be even more strongly linked to the outcome.
We revealed that small household size was associated with an increased risk of dementia, independent of various potential risk factors. By integrating neuroimaging data, we demonstrated that smaller household size was related to lower GMVs, and higher WMH, coupled with changes in white matter tract integrity. These structural differences might partly mediate the association between household size and dementia risk. Consequently, our results highlight the importance of interventions targeting small household sizes.
Data availability
https://www.ukbiobank.ac.uk.The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Vingston, G. et al. Dementia prevention, intervention, and care. Lancet 390(10113), 2673–2734 (2017).
Livingston, G. et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet 396, 413–446 (2020).
Winblad, B. et al. Defeating Alzheimer’s disease and other dementias: A priority for European science and society. Lancet Neurol. 15(5), 455–532 (2016).
Ohida, T. et al. Household size related to prevalence of smoking in women in Japan. J Epidemiol. 10(5), 305–309 (2000).
Kissinger, M. & Damari, Y. Household metabolism: Integrating socio-economic characteristics and lifestyles on individual and national scales as a mean for advancing environmental management. J. Environ. Manage. 279, 111526 (2021).
Desai, R., John, A., Stott, J. & Charlesworth, G. Living alone and risk of dementia: A systematic review and meta-analysis. Ageing Res. Rev. 62, 101122 (2020).
Grande, G. et al. Living alone and dementia incidence: A clinical-based study in people with mild cognitive impairment. J. Geriatr. Psychiatr. Neurol. 31(3), 107–113 (2018).
Poddar, K., Kant, S., Singh, A. & Singh, T. B. An epidemiological study of dementia among the habitants of eastern Uttar Pradesh India. Ann. Indian Acad. Neurol. 14(3), 164–168 (2011).
Veldsman, M. et al. Cerebrovascular risk factors impact frontoparietal network integrity and executive function in healthy ageing. Nat. Commun. 11(1), 4340 (2020).
Chandra, A., Dervenoulas, G. & Politis, M. Alzheimer’s Disease Neuroimaging Initiative. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J. Neurol. 266(6), 1293–1302 (2019).
Grosu, S. et al. Associated factors of white matter hyperintensity volume: a machine-learning approach. Sci. Rep. 11(1), 2325 (2021).
Kokubun, K., Pineda, J. C. D. & Yamakawa, Y. Unhealthy lifestyles and brain condition: Examining the relations of BMI, living alone, alcohol intake, short sleep, smoking, and lack of exercise with gray matter volume. PLoS One. 16(7), e0255285 (2021).
Elliott, M. L. MRI-based biomarkers of accelerated aging and dementia risk in midlife: How close are we?. Ageing Res. Rev. 61, 101075 (2020).
Elliott, M. L. et al. Brain-age in midlife is associated with accelerated biological aging and cognitive decline in a longitudinal birth cohort. Mol. Psychiatr. 26(8), 3829–3838 (2021).
Jiang, F. et al. Retracted: Association between hearing aid use and all-cause and cause-specific dementia: An analysis of the UK Biobank cohort. Lancet. Public Health. 8(5), e329–e338 (2023).
Sudlow, C. et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12(3), e1001779 (2015).
UK Biobank brain scan protocol. Available: http:// biobank.ctsu.ox.ac.uk/crysta- l/refer.cgi?id=2367
Alfaro-Almagro, F. et al. Image processing and quality control for the first 10,000 brain imaging datasets from UK Biobank. Neuroimage. 166, 400–424 (2018).
Miller, K. L. et al. Multimodal population brain imaging in the UK Biobank prospective epidemiological study. Nat. Neurosci. 19, 1523–1536 (2016).
Smith SM, Alfaro-Almargo F, Miller K. Brain imaging documentation. 2020. Accessed January 15, 2022.Available from: https://biobank.ctsu.ox.ac.uk/crystal/ukb/docs/brain_mri.pdf
Shen, C. et al. Associations of social isolation and loneliness with later dementia. Neurology. 99(2), e164–e175. https://doi.org/10.1212/WNL.0000000000200583 (2022).
Yang, Z. et al. Association between regular laxative use and incident dementia in UK biobank participants. Neurology. 100(16), e1702–e1711 (2023).
Parra-Soto, S. et al. Combined association of general and central obesity with incidence and mortality of cancers in 22 sites. Am. J. Clin. Nutr. 113(2), 401–409 (2021).
Lumsden, A. L. et al. Apolipoprotein E (APOE) genotype-associated disease risks: A phenome-wide, registry based, case-control study utilising the UK Biobank. EBioMedicine. 59, 102954 (2020).
Bycroft, C. et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 562, 203–209 (2018).
Mooldijk, S. S., de Crom, T. O., Ikram, M. K., Ikram, M. A. & Voortman, T. Adiposity in the older population and the risk of dementia: The Rotterdam study. Alzheimer’s Dement. 19(5), 2047–2055 (2023).
Lee, C. M. et al. Association of anthropometry and weight change with risk of dementia and its major subtypes: A meta-analysis consisting 2.8 million adults with 57 294 cases of dementia. Obes. Rev. 21(4), e12989 (2020).
Iso-Markku, P. et al. Physical activity as a protective factor for dementia and Alzheimer’s disease: systematic review, meta- analysis and quality assessment of cohort and case–control studies. Br. J. Sports Med. 56, 701–709 (2022).
Chen, S. Y., Feng, Z. & Yi, X. A general introduction to adjustment for multiple comparisons. J. Thorac. Dis. 9(6), 1725–1729 (2017).
Li, J. et al. SGLT2 inhibition, circulating metabolites, and atrial fibrillation: A Mendelian randomization study. Cardiovasc. Diabetol. 22(1), 278 (2023).
Fischer, D. G. Family size and delinquency. Percept. Mot. Skills. 58(2), 527–534. https://doi.org/10.2466/pms.1984.58.2.527 (1984).
Fratiglioni, L., Paillard-Borg, S. & Winblad, B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol. 3(6), 343–353 (2004).
Wang, H. X., Karp, A., Winblad, B. & Fratiglioni, L. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: A longitudinal study from the Kungsholmen project. Am. J. Epidemiol. 155(12), 1081–1087 (2002).
Altamura, C. et al. Regional MRI diffffusion, white-matter hyperintensities, and cognitive function in Alzheimer’s disease and vascular dementia. J. ClinNeurol. 12, 201–208 (2016).
van Straaten, E. C. et al. Periventricular white matter hyperintensities increase the likelihood of progression from amnestic mild cognitive impairment to dementia. J. Neurol. 255(9), 1302–1308 (2008).
Suzuki, H. et al. Abnormal brain white matter microstructure is associated with both pre-hypertension and hypertension. PLoS One. 12(11), e0187600 (2017).
Sandi, C. & Haller, J. Stress and the social brain: Behavioural effffects and neurobiological mechanisms. Nat. Rev. Neurosci. 16(5), 290–304 (2015).
Evans, I. E. M. et al. Social isolation, cognitive reserve, and cognition in healthy older people. PLoS One. 13(8), e0201008. https://doi.org/10.1371/journal.pone.0201008 (2018).
Shaw, B. A., Yang, T. C. & Kim, S. Living alone during old age and the risk of dementia: Assessing the cumulative risk of living alone. J. Gerontol. B. Psychol. Sci. Soc. Sci. 78(2), 293–301 (2023).
Bougea, A., Anagnostouli, M., Angelopoulou, E., Spanou, I. & Chrousos, G. Psychosocial and trauma-related stress and risk of dementia: A meta-analytic systematic review of longitudinal studies. J. Geriatr. Psychiatry Neurol. 35(1), 24–37 (2022).
Fry, A. et al. Comparison of sociodemographic and health related characteristics of UK Biobank participants with those of the general population. Am. J. Epidemiol. 186(9), 1026–1034 (2017).
Batty, G. D., Gale, C. R., Kivimäki, M., Deary, I. J. & Bell, S. Comparison of risk factor associations in UK Biobank against representative, general population based studies with conventional response rates: Prospective cohort study and individual participant meta-analysis. BMJ. 12, 368 (2020).
Wilkinson, T. et al. Identifying dementia outcomes in UK Biobank: A validation study of primary care, hospital admissions and mortality data. Eur. J. Epidemiol. 34(6), 557–565 (2019).
Guo, Y. et al. Plasma proteomic profiles predict future dementia in healthy adults. Nat. Aging. 4(2), 247–260 (2024).
Rook, K. S. Gaps in social support resources in later life: An adaptational challenge in need of further research. J. Soc. Pers. Relat. 26(1), 103–112 (2009).
Acknowledgements
This research was conducted under application number 94885 for UK Biobank Resource. Special thanks to all the participants and professionals contributing to the UK Biobank. This study was supported by grants from the National Natural Science Foundation of China (82071282 to JS), the Rare Disease Registration Platform of Shanghai Ninth People’s Hospital, ShanghaiJiao Tong University School of Medicine (JYHJB08 to JS), the Horizontal Research Project from Shanghai Ninth People’s Hospital (JYHX2021001 to JS), the Research Discipline Fund of the Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine (YJXKB202009), the Horizontal Research Projects from Shanghai Ninth People’s Hospital (JYHX2021022 to YQ) and the 200 Talent project from Shanghai Municipal Education Commission-Gaofeng Clinical Medicine Grant Support (20161422). The funding sources had no role in the study design, collection, analysis, and interpretation of the data, decision to publish, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
J.J.S. and J.R.L. conceived the study and contributed to the interpretation of the results. Concept and design: J.J.S., J.R.L., and C.H.C. Analyses and drafting of the manuscript: C.H.C., P.L.L., Y.Q., and L.Z. Critical revision of the manuscript: Y.N.L., J.T.Y., X.R.Z. Administrative, technical, or material support: Y.N.L., J.T.Y., S.T., S.S.C. All authors had access to the data in the study and had final responsibility for the decision to submit for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cong, CH., Li, PL., Qiao, Y. et al. Association between household size and risk of incident dementia in the UK Biobank study. Sci Rep 14, 11026 (2024). https://doi.org/10.1038/s41598-024-61102-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-61102-6
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
