
Abstract
The combination of metformin and the peroxisome proliferator-activated receptors (PPAR) agonists offers a promising avenue for managing type 2 diabetes (T2D) through their potential complementary mechanisms of action. The results from randomized controlled trials (RCT) assessing the efficacy of PPAR agonists plus metformin versus metformin alone in T2D are inconsistent, which prompted the conduct of the systematic review and meta-analysis. We searched MEDLINE and EMBASE from inception (1966) to March 2023 to identify all RCTs comparing any PPAR agonists plus metformin versus metformin alone in T2D. Categorical variables were summarized as relative risk along with 95% confidence interval (CI). Twenty RCTs enrolling a total of 6058 patients met the inclusion criteria. The certainty of evidence ranged from moderate to very low. Pooled results show that using PPAR agonist plus metformin, as compared to metformin alone, results in lower concentrations of fasting glucose [MD = − 22.07 mg/dl (95% CI − 27.17, − 16.97), HbA1c [MD = − 0.53% (95% CI − 0.67, − 0.38)], HOMA-IR [MD = − 1.26 (95% CI − 2.16, − 0.37)], and fasting insulin [MD = − 19.83 pmol/L (95% CI − 29.54, − 10.13)] without significant increase in any adverse events. Thus, synthesized evidence from RCTs demonstrates the beneficial effects of PPAR agonist add-on treatment versus metformin alone in T2D patients. In particular, novel dual PPARα/γ agonist (tesaglitazar) demonstrate efficacy in improving glycaemic and lipid concentrations, so further RCTs should be performed to elucidate the long-term outcomes and safety profile of these novel combined and personalized therapeutic strategies in the management of T2D.
PROSPERO registration no. CRD42023412603.
Similar content being viewed by others


Introduction
Type 2 diabetes mellitus is a chronic disease characterized by insulin resistance and inadequate pancreatic insulin secretion, resulting in hyperglycemia, and requiring continuous medical care. Approximately 462 million people (6.3% of the global population) were affected by type 2 diabetes in 20171 and it is expected that about 643 million people (11.3% of the global population) will be diagnosed with diabetes by 20302. The management of type 2 diabetes involves a multifaceted approach, including lifestyle modifications, pharmacotherapy, and personalized treatment approach. Current clinical practice recommendations by the American Diabetes Association (ADA) recommends metformin as the first-line therapy, with sulfonylurea, thiazolidinedione (TZD), alpha-glucosidase inhibitors, benzoic acid derivatives, glucagon-like peptide 1 receptor agonists, dipeptidyl peptidase-4 inhibitors, and sodium glucose cotransporter 2 inhibitors as the second-line treatment options, often included in combination therapy3,4. By using drugs with different mechanisms of action, the diverse mechanisms responsible for progression of type 2 diabetes can be addressed, including the management of hyperlipidemia, hypertension, and other related micro- and macrovascular complications. In line with these recent ADA’s Standards of Care recommendations, the selection of drugs added to metformin should be based on the clinical characteristics, including the presence/risk of atherosclerotic cardiovascular disease, heart failure, chronic kidney disease, obesity, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis, and risk for specific adverse drug effects4.
The combination of metformin with peroxisome proliferator-activated receptor (PPAR) agonists has garnered noteworthy attention due to the potential beneficial effects on metabolic control and safety profile through their potential complementary mechanisms of action. Metformin’s glucose-lowering effects are related to reduced mitochondrial respiration, lower hepatic energy production, and decreased glucose production by hepatic cells5,6. PPAR agonists, on the other hand, activate PPARα and/or PPARγ receptors, influencing insulin sensitivity and lipid metabolism. The activation of PPARα decreases triglyceride concentrations, while the activation of PPARγ leads to insulin sensitization and enhanced glucose metabolism7. The fibrate class of hypolipidemic drugs activates PPARα, while antidiabetic agents thiazolidinediones (glitazones) activate PPARγ receptor-regulated pathways, such as adipogenesis, lipid metabolism, glucose control and inflammation8, as well as demonstrate other pleiotropic effects9. Although TZDs, such as troglitazone and rosiglitazone, lost their approvals due to severe side effects, including CV risk, hepatotoxicity, bone fractures, and bladder cancer, pioglitazone showed cardiovascular benefits10. A recent systematic review and meta-analysis demonstrated no significant effects of pioglitazone on incident major adverse cardiovascular events, all-cause mortality, and hospitalization for heart failure11. Furthermore, it was shown that liver steatosis, inflammation, and insulin resistance were improved in patients with type 2 diabetes following one-year pioglitazone treatment12.
Similarly, dual-acting PPARα/γ agonists (glitazars), such as tesaglitazar, also beneficially affected the glucose metabolism, insulin resistance and atherogenic dyslipidaemia in patients with type 2 diabetes13,14,15. In addition to their beneficial effects in lowering glucose and triglyceride concentrations16, PPARα/γ agonists have been also associated with adverse effects, including myocardial ischemia and congestive heart failure17,18, which led to the discontinued use for most of these drugs18. Saroglitazar is the first approved novel dual PPARα/γ agonist that demonstrated efficacy in improving glycaemic and lipid concentrations in patients with diabetic dyslipidemia, with the relative absence of adverse events19,20,21.
Thus, in line with the person-centered diabetes care recommendations4, the combination of metformin and PPAR agonists might be of interest in the treatment of diabetic patients who, based on their clinical characteristics, would benefit from the reported effects of these oral antidiabetic drugs. Previous studies indicated that insulin resistance was more attenuated upon combined treatment of rosiglitazone and metformin as compared to metformin-treated type 2 diabetic patients22,23. Furthermore, the combination of pioglitazone with metformin was reported to lead to better control of HbA1c and lipid concentrations as compared to diabetic patients who were treated with metformin only24,25. Interestingly, the results of the previous double-blind randomized controlled trial (RCT) showed that add-on treatment with dual PPARα/γ agonist, muraglitazar, resulted in greater improvement in HbA1c and lipid concentrations than when pioglitazone was added to metformin26. However, the weight gain and edema were more common in patients who were treated with combined treatment of metformin and muraglitazar as compared with an addition of pioglitazone to metformin therapy26.
Accordingly, here we performed a systematic review and meta-analysis where we aimed to assess the efficacy of combined treatment of metformin plus PPAR agonists versus metformin treatment alone in improving glycemic control, lipid profile, and adverse events in patients with type 2 diabetes. Our main objective is to synthesize all available evidence to assess the benefits and risks associated with the combined treatment of metformin and PPAR agonists versus metformin alone in the management of type 2 diabetes. The specific question was the following: In adults (≥ 18 years of age) with type 2 diabetes, does combination of any PPAR agonists plus metformin compared with metformin alone result in improved primary (fasting glucose [FG] and HbA1c) and secondary outcomes (fasting insulin [FI], Homeostatic Model Assessment for Insulin Resistance [HOMA-IR], Homeostatic Model Assessment for Beta-cell function [HOMA-B], High-sensitivity C-reactive protein [hs-CRP], high-density lipoprotein cholesterol [HDL-C], low-density lipoprotein cholesterol [LDL-C], total cholesterol [TC], triglycerides [TG], systolic blood pressure [SBP], and diastolic blood pressure [DBP]) without increased risk of adverse events (any and gastrointestinal) associated with the treatments in an outpatient setting?
Methods
This systematic review was performed according to a pre-specified protocol and the standard methods in Cochrane Handbook for Systematic Reviews of Interventions and is reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines27,28. The protocol for this systematic review was registered in PROSPERO (CRD42023412603).
Selection criteria
Any randomized control trial (RCT) enrolling adult patients with type 2 diabetes assessing the efficacy of any PPAR agonists plus metformin versus metformin alone was eligible for inclusion. RCTs in pediatric population or observational study designs were not eligible for inclusion. There were no restrictions on the inclusion according to the language of the publication, location, or date of study.
Outcome measures
The primary outcomes were fasting glucose (FG, mg/dl) and hemoglobin A1C (%) concentrations. The secondary outcomes were fasting insulin (FI, pmol/L), HOMA-IR, HOMA-B, hsCRP, high-density lipoprotein cholesterol (HDL-C, mg/dl), low-density lipoprotein cholesterol (LDL-C, mg/dl), total cholesterol (TC, mg/dl), and triglycerides (TG, mg/dl) as well as systolic blood pressure (SBP), diastolic blood pressure (DBP) and occurrence of any and gastrointestinal (GI) adverse effects.
Search methods
A comprehensive and systematic search of PubMed and EMBASE databases was performed from inception until March 29, 2023. The complete search strategy for the two databases is illustrated in “Supplementary Appendix”. There were no limits for language. Furthermore, references of relevant review articles and included studies were hand searched to identify additional eligible studies.
Data collection and analysis
All the citations obtained from the search was imported into EndNote software29. The duplicate citations were removed using the deduplication function in EndNote program. All the unique citations post deduplication were uploaded into Rayyan citation manager30. Two blinded review authors independently reviewed all titles, abstracts, and full-text reports to determine the eligibility of each reference for the inclusion in the systematic review as per the inclusion criteria using the Rayyan citation manager. Any disagreement in the inclusion was reviewed by the senior authors and resolved by consensus.
Data extraction and management
Two review authors independently extracted data using a paper based standardized data extraction form from all included studies. Data were collected on study characteristics (study design, setting), participant characteristics (number of participants enrolled, age,), intervention: characteristics (PPAR agonist, dose, route, administration schedule, and associated therapies) and outcomes. We did not consider any imputation methods for missing data. We had plans to contact the corresponding author in case of unextractable data. However, following standard approaches we were able to extract data from all reported outcomes. All abstracted data were entered into the Review Manager Package31.
Assessment of risk of bias in included studies
The risk of bias in the included studies was assessed using the Cochrane Risk of Bias assessment tool for RCT32. This tool includes the assessment of the method of randomization, allocation concealment, performance bias, detection bias, attrition bias, reporting bias, and any other bias. The overall certainty of evidence was assessed and summarized using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method. This method separates the quality of evidence based on the risk of bias, inconsistency of results, indirectness of evidence, imprecision, and reporting bias33.
Assessment of heterogeneity and reporting biases
Heterogeneity between pooled studies was assessed using the I2 statistic. An I2 value of 0–40% might not be important; 30–60% may represent moderate heterogeneity, 50–90%: may represent substantial heterogeneity; and 75–100% considerable heterogeneity28.
Statistical analysis
All continuous data prior to analysis were converted into the same metric using the online Omni Health Calculator34. All analyses were performed following the intention-to-treat principle. In studies with multiple arms, we divided in half the subjects in the control groups when comparing against experimental arms. Continuous data were summarized as mean difference (MD) along with 95% confidence interval (CI) for each study. Dichotomous data were summarized as risk ratio (RR) along with a 95% CI for each study. When appropriate, summary estimates from individuals studies were pooled under a random-effects model using the DerSimonian-Laird approach outlined a priori in a protocol35. We decided a priori to use random effects model as the model of choice because it is more conservative compared with fixed effects and also incorporates the between-study variance into the calculation. We planned for stratified analysis by PPAR agonist type only. We did not plan for any other subgroup analysis, meta-regression or assessment of publication bias. All data analyses were performed using Review Manager package31.
Results
Results of the search
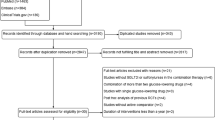
The search strategy identified a total of 3460 citations. As shown in Fig. 1, after applying the inclusion criteria, 20 RCTs involving 23 comparisons and enrolling a total of 6529 patients met the inclusion criteria22,23,24,25,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51.

Study selection flow diagram.
Characteristics of included studies
The total number of participants enrolled was 6058, with 3204 randomized to PPAR agonist plus metformin and 2854 randomized to the metformin-alone arm. As shown in Table 1, 85% of studies (17/20) reported a single comparison22,23,24,25,36,37,38,39,40,42,45,46,47,48,49,50,51, while the remaining 15% of studies (3/20) reported two comparison arms41,43,44. The daily metformin dose in the included studies ranged from 500 to 2550 mg/day. Pioglitazone was studied in 40% of studies (8/20) and the daily dose ranged from 15 to 45 mg/day24,25,36,39,40,42,46,50. Rosiglitazone was studied in 55% of studies (11/20) and the daily dose ranged from 4 to 8 mg/day22,23,37,38,41,44,45,47,48,49,51. Tesaglitazar was studied in 5% of studies (1/20) and the daily dose ranged from 0.5 to 1 mg/day43. The study duration ranged from 8 to 80 weeks. A majority of studies (60%, 12/20) evaluated HbA1c as their primary outcome25,36,37,38,41,43,44,46,47,48,49,51. A majority of studies (70%, 14/20) were sponsored by the pharmaceutical industry24,25,36,37,38,40,41,42,43,46,47,48,49,51, 10% (2/20) were sponsored by government/academia22,45, and 20% of studies (4/20) did not report the source of funding23,39,44,50.
Assessment of methodological quality of included studies
As shown in Supplement Fig. 1, of the 20 RCTs, for the generation of randomization sequence, 5 (25%) RCTs were rated as low risk of bias22,37,39,41,50, and 15 (75%) as unclear risk of bias23,24,25,36,38,40,42,43,44,45,46,47,48,49,51. For the adequacy of allocation concealment, 3 RCTs (15%) were rated as low risk of bias22,39,41, and 17 (85%) as unclear risk of bias23,24,25,36,37,38,40,42,43,44,45,46,47,48,49,51. For the blinding of participants and personnel, 17 (85%) RCTs were rated as low risk of bias23,24,25,36,37,38,39,40,41,42,43,46,47,48,49,51,52, 2 (10%) RCTs as high risk and 1 (5%) as unclear risk of bias44,45. For the blinding of outcomes assessors, 16 (80%) RCTs were rated as low risk of bias23,24,25,36,37,38,39,40,41,42,43,46,47,49,51,52, 1 (5%) as high risk45, and 3 (15%) as unclear risk of bias22,44,48. For the domain of incomplete outcome data, 1 RCT (5%) was rated as low risk of bias42, 17 (85%) RCTs as high risk22,24,25,36,37,38,39,40,41,43,44,45,46,47,48,49,51, and 2 (10%) RCTs as unclear risk23,50. For the domain of selective reporting of outcome, 18 (90%) RCTs were rated as low risk of bias22,23,24,25,36,37,38,39,40,41,42,43,44,45,47,48,49,51 and 2 (10%) RCTs as high risk46,52. All RCTs were rated as low risk of bias for other biases22,23,24,25,36,37,38,39,40,41,42,43,44,45,46,47,48,49,51,53. The overall certainty of evidence of included RCTs ranged from very low to moderate (Table 2).
Outcomes
Fasting glucose
As shown in Fig. 2, fasting glucose (FG) concentrations were reported in 19 RCTs (22 comparisons) enrolling 5647 patients22,23,24,25,36,37,38,39,40,41,42,43,44,45,47,48,49,50,51. The mean FG was significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 22.07 mg/dl, 95% CI = − 27.17, − 16.97; p < 0.001). Heterogeneity among pooled RCTs was substantial (I2 = 83%). The overall certainty in the estimate was low (Table 2).

Fasting glucose.
There was no significant difference between the subgroups (p = 0.82).
Hemoglobin A1c
As shown in Fig. 3, hemoglobin A1c was reported in 18 RCTs (21 comparisons) enrolling 5611 patients22,23,24,25,36,37,38,39,40,41,42,43,44,45,47,48,49,51. The mean HbA1c concentrations were significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 0.53%, 95% CI = − 0.67, − 0.38; p < 0.001). Heterogeneity among pooled RCTs was substantial (I2 = 88%). The overall certainty in the estimate was low (Table 2).

Hemoglobin A1c.
There was no significant difference between the subgroups (p = 0.10).
HOMA-IR
As shown in Supplement Fig. 2, HOMA-IR was reported in 7 RCTs (7 comparisons) enrolling 875 patients22,23,25,42,45,48,50. The mean HOMA-IR was significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 1.26, 95% CI = − 2.16, − 0.37; p = 0.006). Heterogeneity among pooled RCTs was considerable (I2 = 91%). The overall certainty in the estimate was very low (Table 2).
There was no significant difference between the subgroups (p = 0.44).
Fasting insulin
As shown in Supplement Fig. 3, fasting insulin was reported in 14 RCTs (16 comparisons) enrolling 3434 patients22,23,24,25,37,39,41,42,43,45,47,48,49,50. The mean fasting insulin concentrations were significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 19.83 pmol/L, 95% CI = − 29.54, − 10.13; p < 0.001). Heterogeneity among pooled RCTs was considerable (I2 = 93%). The overall certainty in the estimate was very low (Table 2).
There was no significant difference between the subgroups (p = 0.10).
HOMA-B
As shown in Supplement Fig. 4, HOMA-B was reported in 4 RCTs (4 comparisons) enrolling 1487 patients37,42,48,49. The mean HOMA-B was significantly higher in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = 7.45, 95% CI = 3.45, 11.45; p = 0.0003). Heterogeneity among pooled RCTs was substantial (I2 = 65%).
There was a significant difference between the subgroups (p = 0.009).
hsCRP
As shown in Supplement Fig. 5, hsCRP was reported in 9 RCTs (10 comparisons) enrolling 2520 patients22,24,25,37,43,45,47,49,50. The mean hsCRP concentrations were significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 0.62 mg/L, 95% CI = − 0.87, − 0.37; p < 0.001). Heterogeneity among pooled RCTs was substantial (I2 = 76%).
There was no significant difference between the subgroups (p = 0.97).
Total cholesterol
As shown in Supplement Fig. 6, total cholesterol was reported in 18 RCTs (21 comparisons) enrolling 5607 patients22,23,24,25,37,38,40,41,42,43,44,45,46,47,48,49,50,51. The mean total cholesterol concentrations were significantly higher in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = 10.57 mg/dl, 95% CI = 7.19, 13.95; p < 0.001). Heterogeneity among pooled RCTs was considerable (I2 = 97%). The overall certainty in the estimate was low (Table 2).
There was a significant difference between the subgroups (p = 0.008).
High-density lipoprotein cholesterol
As shown in Supplement Fig. 7, HDL-cholesterol was reported in 17 RCTs (21 comparisons) enrolling 5607 patients22,24,25,37,38,40,41,42,43,44,45,46,47,48,49,50,51. The mean HDL-cholesterol concentrations were significantly higher in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = 2.81 mg/dl, 95% CI = 2.00, 3.62; p < 0.001). Heterogeneity among pooled RCTs was considerable (I2 = 94%).
There was no significant difference between the subgroups (p = 0.32).
Low-density lipoprotein cholesterol
As shown in Supplement Fig. 8, LDL-cholesterol was reported in 17 RCTs (20 comparisons) enrolling 5569 patients22,24,25,37,38,40,41,42,43,44,45,46,47,48,49,50,51. The mean LDL-cholesterol concentrations were significantly higher in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = 6.81 mg/dl, 95% CI = 3.28, 10.33; p = 0.0002). Heterogeneity among pooled RCTs was considerable (I2 = 98%). The overall certainty in the estimate was low (Table 2).
There was a significant difference between the subgroups (p = 0.0001).
Triglycerides
As shown in Supplement Fig. 9, triglycerides were reported in 18 RCTs (21 comparisons) enrolling 5507 patients22,23,24,25,37,38,40,41,42,43,44,45,46,47,48,49,50,51. There was no significant difference in mean triglycerides concentrations in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 10.96 mg/dl, 95% CI = − 22.10, 0.18; p = 0.05). Heterogeneity among pooled RCTs was considerable (I2 = 98%).
There was a significant difference between the subgroups (p = 0.003).
Systolic blood pressure
As shown in Supplement Fig. 10, systolic blood pressure (BP) was reported in 6 RCTs (6 comparisons) enrolling 1053 patients22,23,42,45,49,50. The mean systolic BP was significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 3.19 mmHg, 95% CI = − 4.83, − 1.55; p = 0.0001). Heterogeneity among pooled RCTs was not important (I2 = 27%).
There was no significant difference between the subgroups (p = 0.64).
Diastolic blood pressure
As shown in Supplement Fig. 11, diastolic blood pressure (BP) was reported in 6 RCTs (6 comparisons) enrolling 1053 patients22,23,42,45,49,50. The mean diastolic BP was significantly lower in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone (MD = − 2.82 mmHg, 95% CI = − 4.99, − 0.64; p = 0.01). Heterogeneity among pooled RCTs was substantial (I2 = 81%).
There was no significant difference between the subgroups (p = 0.41).
Any adverse events
As shown in Fig. 4, adverse events were reported in 13 RCTs (16 comparisons) enrolling 4841 patients24,25,36,37,38,41,42,43,44,46,48,49,51. The risk of adverse events in patients treated with metformin plus PPAR agonist compared to patients treated with metformin alone was not significant (RR = 1.02, 95% CI = 0.97, 1.08; p = 0.41). Heterogeneity among pooled RCTs was not important (I2 = 14%). The overall certainty in the estimate was moderate (Table 2).

Any adverse event.
There was no significant difference between the subgroups (p = 0.30).
Gastrointestinal intolerance
As shown in Supplement Fig. 12, adverse events were reported in 9 RCTs (10 comparisons) enrolling 4083 patients37,38,42,43,46,47,48,49,51. Patients treated with metformin plus PPAR agonist had a significantly lower risk of gastrointestinal adverse events compared to patients treated with metformin alone (RR = 0.81, 95% CI = 0.73, 0.90; p < 0.001). The heterogeneity among pooled RCTs was not important (I2 = 0%). The overall certainty in the estimate was moderate (Table 2).
There was no significant difference between the subgroups (p = 0.31).
All results from the subgroup analyses by the agent are reported in the supplementary material.
Discussion
The findings from our systematic review and meta-analysis, based on our knowledge, represent the largest body of synthesized evidence to date assessing the outcomes of metformin treatment alone versus combined treatment of metformin with PPAR agonists. The pooled results show that, on average, combination treatment with PPAR agonists compared with metformin alone is associated with significantly improved glycemic control in patients with type 2 diabetes. Specifically, the use of PPAR agonists plus metformin results in significantly lower concentrations of fasting glucose, hemoglobin A1c, fasting insulin, and HOMA-IR as compared to metformin treatment alone. In addition, the effect of combination treatment was consistent across all PPAR agonists types including PPARγ activators, pioglitazone and rosiglitazone, and dual PPARα/γ activator, tesaglitazar. These findings are in line with the previous studies that demonstrate the epidemiological and biological plausibility of these results. The beneficial effects of PPARα and PPARγ activation on glycemic control happens primarily by increasing insulin sensitivity and preserving beta-cell function16,54 and the activation of PPARγ improves insulin sensitization and glucose uptake7,18. Treatment with PPARγ agonists, TZDs, effectively lowers HbA1c concentrations by about 1% as monotherapy and improves insulin sensitivity in patients with type 2 diabetes55. Furthermore, the pioglitazone treatment lowered concentrations of fasting glucose, insulin, and HbA1c in type 2 diabetic patients56, while another TZD, rosiglitazone, improved overall glucose tolerance and increased insulin sensitivity in patients with impaired glucose tolerance and type 2 diabetes57. Previous studies have also reported decreased HOMA-IR index, glucose, insulin, and HbA1c concentrations in diabetic patients upon an addition of rosiglitazone23 and pioglitazone25 to metformin treatment. Also, rosiglitazone provided more durable glycemic control than metformin or sulfonylurea58. Similarly, another study showed that the addition of pioglitazone to metformin-treated type 2 diabetic patients decreased HbA1c and HOMA-IR42 as well as fasting insulin concentrations as compared with the sulfonylurea plus metformin group59.
The results of our meta-analysis demonstrated that treatment with PPARα/γ agonist, tesaglitazar, plus metformin reduced triglyceride (TG) concentrations in patients with type 2 diabetes, as compared to metformin treatment alone. However, treatment with TZDs (PPARγ agonists) plus metformin did not significantly affect TG concentrations. This is in line with the findings that the combined treatment of PPARα/γ agonist muraglitazar with metformin led to more enhanced effect in reducing TG concentrations as compared to the combined treatment of metformin with TZD agent pioglitazone26. Furthermore, results from recent clinical trials demonstrated that saroglitazar therapy decreased triglyceride concentrations by 45% as well as reduced concentrations of other atherogenic lipids, including TC, LDL-C, and VLDL-C19,60. It was also found that saroglitazar treatment improved lipid profile, including reduced TG, LDL-C, VLDL-C, TC, and increased HDL-C concentrations, in patients with type 2 diabetes receiving background metformin therapy61. The combined treatment of saroglitazar and metformin also resulted in a greater reduction of TG concentrations as compared to patients with type 2 diabetes who were treated with fenofibrate plus metformin21.
In addition to reduced triglyceride concentrations, our findings indicate that adding PPARα/γ activator (tesaglitazar) to metformin treatment does not significantly affect the concentrations of TC and LDL-C as compared to the patients with type 2 diabetes who were treated with metformin only. However, our meta-analysis demonstrates increased concentrations of total cholesterol and LDL-C upon treatment with PPARγ activators (TZDs) plus metformin vs metformin treatment alone. The results of the subgroup analysis per agent, showed that rosiglitazone plus metformin increased concentrations of TC and LDL-C, while pioglitazone plus metformin significantly affected TC concentrations only. This is in contrast to the previous studies which demonstrated that rosiglitazone has no significant effect on TG concentrations, while pioglitazone reduced TG and LDL particle size/concentrations62. Furthermore, it was reported that treatment with rosiglitazone plus metformin reduced concentrations of TG and TC23, while an addition of pioglitazone to metformin-treated patients with type 2 diabetes decreased TG, but increased HDL-C concentrations59. Since it was reported that metformin treatment itself reduces LDL-C concentrations in patients with type 2 diabetes62,63, it is possible that upon adding TZDs to metformin, the concentrations of LDL-C and/or TC concentrations increase as observed in our meta-analysis, which might be in line with the adverse effects of TZDs on the cardiovascular system. In line with our results, it was suggested that the potential difference in the risk of myocardial infarction between pioglitazone and rosiglitazone may lie in their different effects on lipoproteins concentrations, with pioglitazone demonstrating more favorable effects (TG decrease, HDL-C increase, with no effect on LDL-C or TC) than rosiglitazone (no effect on TG concentrations, HDL-C increase, but increases in LDL-C and TC concentrations)64,65. The pooled results as well as the results from the subgroup analysis according to the type of PPAR agonist showed the beneficial effects of the combined treatment of PPARα/γ or PPARγ agonists plus metformin vs metformin alone on HDL-C concentrations. This is in line with the previous studies, which also showed that increased HDL-C concentrations upon activation of PPARα7,18 and PPARγ receptors59,66.
Furthermore, our findings also indicated the beneficial effects of combined treatment of PPARγ agonists with metformin, which decreased systolic and diastolic blood pressure in patients with type 2 diabetes. This is in line with previous reports indicating that the activation of PPARγ lowers systemic blood pressure7,18,22,45. Another study also showed a reduction of systolic and diastolic blood pressure at 12 months of combined treatment with rosiglitazone and metformin, which correlated with HOMA-IR index, indicating that rosiglitazone can decrease blood pressure and that the enhancement of insulin sensitivity is associated with the reduction of blood pressure23.
Our findings showed that the concentrations of high-sensitivity C-reactive protein (hsCRP) were decreased following the combined treatment of PPARγ activators (TZDs) with metformin as compared to metformin treatment alone. This is in line with the previous studies, showing decreased concentrations of inflammation and cardiovascular risk markers, such as CRP, in obese and type 2 diabetic patients with TZD intervention67. Additionally, pioglitazone treatment significantly reduced CRP56,68 and hsCRP concentrations52,59. The addition of rosiglitazone to metformin resulted in reduced concentrations of hsCRP as compared to type 2 diabetes patients who were treated only with metformin22,45. It was also reported that the combined treatment of PPARα/γ agonist muraglitazar with metformin led to a more enhanced effect in reducing hsCRP concentrations as compared to combined treatment of metformin with pioglitazone. However, our results demonstrated that there was no significant effect on hsCRP concentrations when another agent from this class of dual PPARα/γ agonist, tesaglitazar, was added to metformin treatment.
Our results of overall and subgroup analysis showed that there were no significant side effects associated with the addition of any PPAR agonist to metformin in patients with type 2 diabetes as compared to metformin, which is contrast to a few studies reporting an increased risk of adverse events associated with the use of PPAR agonists19,58,65,69,70. However, most studies reported either any adverse event or gastrointestinal toxicities, so we could not compare the cardiac and other toxicities possibly associated with addition of PPAR agonists.
Metformin treatment is associated with a high incidence of gastrointestinal (GI) side effects62. Strikingly, our meta-analysis showed that the risk of GI events was reduced after adding PPARγ activator (TZDs) to metformin treatment, while this beneficial effect was not observed upon combined treatment with dual PPARα/γ activator vs metformin treatment alone.
There are a several limitations to this systematic review and meta-analysis. These limitations primarily relate to the conduct and reporting of individual RCTs included here, which may possibly affect the overall results. For example, the overall methodological quality of evidence ranged from very low to moderate due to risk of bias and heterogeneity in pooled estimates. The risk of bias assessment may possibly be a function of reporting and not necessarily conduct. Similarly, the reasons for heterogeneity could be multifactorial, including difference in primary outcomes, study duration, type of PPAR agonist, metformin and PPAR dosing across pooled studies. Most included RCTs did report the sample size assessment details, which possibly reduces the chance of random error, and we suspect that, given the consistency of effects observed across all glycemic outcomes, the results are possibly not influenced by random error and risk of bias. Another important issue limitation relates to generalizability. All RCTs in this systematic review assessed the efficacy of either PPARγ or α/γ agonists and therefore these findings are possibly limited to these specific types only and may not necessarily apply to PPARα or other PPAR agonists. However, our search did not find any RCTs assessing the efficacy of PPARα or other PPAR agonists. Once such RCTs are available this systematic review and meta-analysis will require an update. Nevertheless, despite these limitations, the impact of combination treatment with PPAR agonist compared with metformin alone in patients with type 2 diabetes is plausibly strong.
In conclusion, to the best of our knowledge, this meta-analysis is the largest body of synthesized evidence to date that assesses the outcomes of metformin treatment alone versus combined metformin and PPAR agonists in patients diagnosed with type 2 diabetes. Our findings indicate the beneficial effects of add-on treatment with PPAR agonist on glycemic control, reduced HbA1c concentrations, and ameliorated insulin resistance as compared to monotherapy with metformin. In addition, this combination also showed the favorable effects on type 2 diabetes-associated traits, including hypertension, increased concentrations of inflammatory markers, and dyslipidemia. Our meta-analysis demonstrated more favorable effects of combined metformin treatment with PPARα/γ activator (tesaglitazar) on lipid profile by lowering the concentrations of TG, increasing HDL-C concentrations and not increasing the concentrations of LDL-C and TC observed upon adding TZDs to metformin treatment. This might be in line with the adverse effects of TZDs on the cardiovascular system. However, our results also indicate that adding TZDs to metformin treatment results in a more favorable safety profile by reducing the number of GI adverse events as compared to type 2 diabetic patients who were treated with metformin only. Thus, it is crucial to consider the beneficial as well as the potential adverse events, such as gastrointestinal and cardiovascular events, which are related to use of the combination of metformin and PPAR agonists that would require monitoring and the potential adjustment of the prescribed medication or its dose. Further studies are warranted to elucidate the long-term outcomes and optimal usage of combined metformin and PPAR agonist in the management of type 2 diabetes, with continued research exploring optimal dosing regimens, long-term effects, and personalized treatment approaches. In addition, the potential for novel PPAR agonists with improved safety profiles warrants further investigation.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary files.
Abbreviations
- DBP:
-
Diastolic blood pressure
- FG:
-
Fasting glucose
- FI:
-
Fasting insulin
- GI:
-
Gastrointestinal
- HDL-C:
-
High density lipoprotein-cholesterol
- hsCRP:
-
High-sensitivity C-reactive protein
- LDL-C:
-
Low density lipoprotein-cholesterol
- MD:
-
Mean difference
- PPAR:
-
Peroxisome proliferator-activated receptor
- RCT:
-
Randomized control trial
- SBP:
-
Systolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- TZD:
-
Thiazolidinedione
References
Khan, M. A. B. et al. Epidemiology of type 2 diabetes—Global burden of disease and forecasted trends. J. Epidemiol Glob. Health 10(1), 107–111 (2020).
IDF, International Diabetes Federation. IDF Diabetes Atlas—10th Edition (2021).
Manu, P., Rogozea, L. M. & Cernea, S. Pharmacological management of diabetes mellitus: A century of expert opinions in Cecil Textbook of Medicine. Am. J. Ther. 28(4), e397–e410 (2021).
ElSayed, N. A. et al. 9. Pharmacologic approaches to glycemic treatment: Standards of care in diabetes-2023. Diabetes Care 46(Suppl 1), S140–S157 (2023).
Ziqubu, K. et al. Anti-obesity effects of metformin: A scoping review evaluating the feasibility of brown adipose tissue as a therapeutic target. Int. J. Mol. Sci. 24(3), 2227 (2023).
Uddin, R. et al. New evidence for the mechanism of action of a type-2 diabetes drug using a magnetic bead-based automated biosensing platform. ACS Sens. 2(9), 1329–1336 (2017).
Balakumar, P., Mahadevan, N. & Sambathkumar, R. A contemporary overview of PPARalpha/gamma dual agonists for the management of diabetic dyslipidemia. Curr. Mol. Pharmacol. 12(3), 195–201 (2019).
Brown, J. D. & Plutzky, J. Peroxisome proliferator-activated receptors as transcriptional nodal points and therapeutic targets. Circulation 115(4), 518–533 (2007).
Giglio, R. V. et al. An update on the current and emerging use of thiazolidinediones for type 2 diabetes. Medicina 58(10), 1475 (2022).
Engler, C. et al. Long-term trends in the prescription of antidiabetic drugs: Real-world evidence from the Diabetes Registry Tyrol 2012–2018. BMJ Open Diabetes Res. Care 8(1), e001279 (2020).
Mannucci, E. et al. Effects of pioglitazone on cardiovascular events and all-cause mortality in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 32(3), 529–536 (2022).
Della Pepa, G. et al. Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: Clinical and pathophysiological insights from a subgroup of the TOSCA.IT randomised trial. Diabetes Res. Clin. Pract. 178, 108984 (2021).
Fagerberg, B. et al. Tesaglitazar, a novel dual peroxisome proliferator-activated receptor alpha/gamma agonist, dose-dependently improves the metabolic abnormalities associated with insulin resistance in a non-diabetic population. Diabetologia 48(9), 1716–1725 (2005).
Schuster, H. et al. Tesaglitazar, a dual peroxisome proliferator-activated receptor alpha/gamma agonist, improves apolipoprotein levels in non-diabetic subjects with insulin resistance. Atherosclerosis 197(1), 355–362 (2008).
Goldstein, B. J. et al. Effect of tesaglitazar, a dual PPAR alpha/gamma agonist, on glucose and lipid abnormalities in patients with type 2 diabetes: A 12-week dose-ranging trial. Curr. Med. Res. Opin. 22(12), 2575–2590 (2006).
Chatterjee, S., Majumder, A. & Ray, S. Observational study of effects of Saroglitazar on glycaemic and lipid parameters on Indian patients with type 2 diabetes. Sci. Rep. 5, 7706 (2015).
Lincoff, A. M. et al. Effect of aleglitazar on cardiovascular outcomes after acute coronary syndrome in patients with type 2 diabetes mellitus: The AleCardio randomized clinical trial. JAMA 311(15), 1515–1525 (2014).
Kalliora, C. & Drosatos, K. The glitazars paradox: Cardiotoxicity of the metabolically beneficial dual PPARalpha and PPARgamma activation. J. Cardiovasc. Pharmacol. 76(5), 514–526 (2020).
Pai, V. et al. A multicenter, prospective, randomized, double-blind study to evaluate the safety and efficacy of Saroglitazar 2 and 4 mg compared to Pioglitazone 45 mg in diabetic dyslipidemia (PRESS V). J. Diabetes Sci. Technol. 8(1), 132–141 (2014).
Agrawal, R. The first approved agent in the Glitazar’s class: Saroglitazar. Curr. Drug Targets 15(2), 151–155 (2014).
Ghosh, A. et al. Comparison of effectiveness and safety of add-on therapy of Saroglitazar and Fenofibrate with metformin in Indian patients with diabetic dyslipidaemia. J. Clin. Diagn. Res. 10(3), FC01–FC04 (2016).
Kadoglou, N. P. et al. Effects of rosiglitazone and metformin treatment on apelin, visfatin, and ghrelin levels in patients with type 2 diabetes mellitus. Metabolism 59(3), 373–379 (2010).
Negro, R. et al. Rosiglitazone effects on blood pressure and metabolic parameters in nondipper diabetic patients. Diabetes Res. Clin. Pract. 70(1), 20–25 (2005).
Hanefeld, M. et al. Double-blind, randomized, multicentre, and active comparator controlled investigation of the effect of pioglitazone, metformin, and the combination of both on cardiovascular risk in patients with type 2 diabetes receiving stable basal insulin therapy: The PIOCOMB study. Cardiovasc. Diabetol. 10, 65 (2011).
Kaku, K. Efficacy and safety of therapy with metformin plus pioglitazone in the treatment of patients with type 2 diabetes: A double-blind, placebo-controlled, clinical trial. Curr. Med. Res. Opin. 25(5), 1111–1119 (2009).
Kendall, D. M. et al. Improvement of glycemic control, triglycerides, and HDL cholesterol levels with muraglitazar, a dual (alpha/gamma) peroxisome proliferator-activated receptor activator, in patients with type 2 diabetes inadequately controlled with metformin monotherapy: A double-blind, randomized, pioglitazone-comparative study. Diabetes Care 29(5), 1016–1023 (2006).
Page, M. J. et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 372, n160 (2021).
Higgins, J. P. T, Chandler, J., Cumpston, M., Li, T., Page, M. J., Welch. V. A. (eds). Cochrane Handbook for Systematic Reviews of Interventions, version 6.4 (updated August 2023). Cochrane, 2023; www.training.cochrane.org/handbook.
The EndNote Team. 2023, Clarivate: Philadelphia, PA.
Ouzzani, M. et al. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 5(1), 210 (2016).
Review Manager (RevMan) 2020, The Cochrane Collaboration
Higgins, J. P. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
Schünemann, H., Guyatt, G., Oxman, A., (eds.) GRADE handbook for grading quality of evidence and strength of recommendations. 2013; https://gdt.gradepro.org/app/handbook/handbook.html.
Koperska, M., Omni Health Calculator. 2024.
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 7(3), 177–188 (1986).
Efficacy of Pioglitazone and Fortamet Combination Therapy in Subjects With Type 2 Diabetes. 2008, Takeda Global Research & Development Center.
Bailey, C. J. et al. Rosiglitazone/metformin fixed-dose combination compared with uptitrated metformin alone in type 2 diabetes mellitus: A 24-week, multicenter, randomized, double-blind, parallel-group study. Clin. Ther. 27(10), 1548–1561 (2005).
Borges, J. L. et al. A randomized, parallel group, double-blind, multicentre study comparing the efficacy and safety of Avandamet (rosiglitazone/metformin) and metformin on long-term glycaemic control and bone mineral density after 80 weeks of treatment in drug-naive type 2 diabetes mellitus patients. Diabetes Obes. Metab. 13(11), 1036–1046 (2011).
Derosa, G. et al. Direct comparison among oral hypoglycemic agents and their association with insulin resistance evaluated by euglycemic hyperinsulinemic clamp: The 60’s study. Metabolism 58(8), 1059–1066 (2009).
Einhorn, D. et al. Pioglitazone hydrochloride in combination with metformin in the treatment of type 2 diabetes mellitus: A randomized, placebo-controlled study. The Pioglitazone 027 Study Group. Clin. Ther. 22(12), 1395–409 (2000).
Fonseca, V. et al. Effect of metformin and rosiglitazone combination therapy in patients with type 2 diabetes mellitus: A randomized controlled trial. JAMA 283(13), 1695–1702 (2000).
Genovese, S. et al. Pioglitazone randomised Italian Study on Metabolic Syndrome (PRISMA): Effect of pioglitazone with metformin on HDL-C levels in type 2 diabetic patients. J. Endocrinol. Invest. 36(8), 606–616 (2013).
Goke, B. et al. The effects of tesaglitazar as add-on treatment to metformin in patients with poorly controlled type 2 diabetes. Diab. Vasc. Dis. Res. 4(3), 204–213 (2007).
Gomez-Perez, F. J. et al. Efficacy and safety of rosiglitazone plus metformin in Mexicans with type 2 diabetes. Diabetes Metab. Res. Rev. 18(2), 127–134 (2002).
Kadoglou, N. P. et al. Effects of rosiglitazone/metformin fixed-dose combination therapy and metformin monotherapy on serum vaspin, adiponectin and IL-6 levels in drug-naive patients with type 2 diabetes. Exp. Clin. Endocrinol. Diabetes 119(2), 63–68 (2011).
Perez, A. et al. Efficacy and safety of pioglitazone/metformin fixed-dose combination therapy compared with pioglitazone and metformin monotherapy in treating patients with T2DM. Curr. Med. Res. Opin. 25(12), 2915–2923 (2009).
Rosenstock, J. et al. Initial treatment with rosiglitazone/metformin fixed-dose combination therapy compared with monotherapy with either rosiglitazone or metformin in patients with uncontrolled type 2 diabetes. Diabetes Obes. Metab. 8(6), 650–660 (2006).
Scott, R. et al. Efficacy and safety of sitagliptin when added to ongoing metformin therapy in patients with type 2 diabetes. Diabetes Obes. Metab. 10(10), 959–969 (2008).
Stewart, M. W. et al. Effect of metformin plus roziglitazone compared with metformin alone on glycaemic control in well-controlled Type 2 diabetes. Diabet. Med. 23(10), 1069–1078 (2006).
Wang, C. H. et al. Pioglitazone increases the numbers and improves the functional capacity of endothelial progenitor cells in patients with diabetes mellitus. Am. Heart J. 152(6), 1051.e1-1051.e8 (2006).
Weissman, P. et al. Effects of rosiglitazone added to submaximal doses of metformin compared with dose escalation of metformin in type 2 diabetes: The EMPIRE Study. Curr. Med. Res. Opin. 21(12), 2029–2035 (2005).
Wang, Z. et al. Pioglitazone attenuates drug-eluting stent-induced proinflammatory state in patients by blocking ubiquitination of PPAR. PPAR Res. 2016, 7407153 (2016).
Wilding, J. P. et al. Tesaglitazar, as add-on therapy to sulphonylurea, dose-dependently improves glucose and lipid abnormalities in patients with type 2 diabetes. Diab. Vasc. Dis. Res. 4(3), 194–203 (2007).
Cox, S. L. Tesaglitazar: A promising approach in type 2 diabetes. Drugs Today 42(3), 139–146 (2006).
Yau, H. et al. The future of thiazolidinedione therapy in the management of type 2 diabetes mellitus. Curr. Diab. Rep. 13(3), 329–341 (2013).
Satoh, N. et al. Antiatherogenic effect of pioglitazone in type 2 diabetic patients irrespective of the responsiveness to its antidiabetic effect. Diabetes Care 26(9), 2493–2499 (2003).
Osei, K., Gaillard, T. & Schuster, D. Thiazolidinediones increase hepatic insulin extraction in African Americans with impaired glucose tolerance and type 2 diabetes mellitus. A pilot study of rosiglitazone. Metabolism 56(1), 24–29 (2007).
Kahn, S. E. et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N. Engl. J. Med. 355(23), 2427–2443 (2006).
Lin, K. D. et al. Thiazolidinedione addition reduces the serum retinol-binding protein 4 in type 2 diabetic patients treated with metformin and sulfonylurea. Transl. Res. 151(6), 309–314 (2008).
Jani, R. H. et al. A multicenter, prospective, randomized, double-blind study to evaluate the safety and efficacy of Saroglitazar 2 and 4 mg compared with placebo in type 2 diabetes mellitus patients having hypertriglyceridemia not controlled with atorvastatin therapy (PRESS VI). Diabetes Technol. Ther. 16(2), 63–71 (2014).
Krishnappa, M. et al. Effect of saroglitazar 2 mg and 4 mg on glycemic control, lipid profile and cardiovascular disease risk in patients with type 2 diabetes mellitus: A 56-week, randomized, double blind, phase 3 study (PRESS XII study). Cardiovasc. Diabetol. 19(1), 93 (2020).
Tarry-Adkins, J. L. et al. Efficacy and side effect profile of different formulations of metformin: A systematic review and meta-analysis. Diabetes Ther. 12(7), 1901–1914 (2021).
Abdalla, M. A. et al. Effect of pharmacological interventions on lipid profiles and C-reactive protein in polycystic ovary syndrome: A systematic review and meta-analysis. Clin. Endocrinol. 96(4), 443–459 (2022).
Chiquette, E., Ramirez, G. & Defronzo, R. A meta-analysis comparing the effect of thiazolidinediones on cardiovascular risk factors. Arch. Intern. Med. 164(19), 2097–2104 (2004).
Soccio, R. E., Chen, E. R. & Lazar, M. A. Thiazolidinediones and the promise of insulin sensitization in type 2 diabetes. Cell Metab. 20(4), 573–591 (2014).
Goldberg, R. B. et al. A comparison of lipid and glycemic effects of pioglitazone and rosiglitazone in patients with type 2 diabetes and dyslipidemia. Diabetes Care 28(7), 1547–1554 (2005).
Consoli, A. & Devangelio, E. Thiazolidinediones and inflammation. Lupus 14(9), 794–797 (2005).
Agarwal, R. Anti-inflammatory effects of short-term pioglitazone therapy in men with advanced diabetic nephropathy. Am. J. Physiol. Renal. Physiol. 290(3), F600–F605 (2006).
Kahn, S. E. et al. Rosiglitazone-associated fractures in type 2 diabetes: An Analysis from A Diabetes Outcome Progression Trial (ADOPT). Diabetes Care 31(5), 845–851 (2008).
Nissen, S. E. & Wolski, K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N. Engl. J. Med. 356(24), 2457–2471 (2007).
Acknowledgements
This study was supported by the Khalifa University research grant.
Funding
This study was supported by the Khalifa University research grant.
Author information
Authors and Affiliations
Contributions
S.S., S.A., A.K., F.S., T.R., and Z.V.A. were responsible for the study concept, including formulation and evolution of overarching research aims. S.A., S.A.A., A.K., and T.R. were responsible for data curation. All authors were responsible for the investigation. S.A., T.R., and T.S. conducted data analysis. All authors interpreted the data. S.A., T.R., A.K., and S.S. were engaged in the writing of the initial draft of the manuscript, which was reviewed and edited by all authors. T.R. and A.K. were responsible for data visualization. S.S. acquired the funding for the study leading to this publication. S.S. and A.K. supervised the study. All authors revised the manuscript critically for its important intellectual content and gave final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alnuaimi, S., Reljic, T., Abdulla, F.S. et al. PPAR agonists as add-on treatment with metformin in management of type 2 diabetes: a systematic review and meta-analysis. Sci Rep 14, 8809 (2024). https://doi.org/10.1038/s41598-024-59390-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-59390-z
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
