
Abstract
Several brain regions have been implicated in human painful experiences, but none have been proven to be specific to pain. We exploited arterial spin-labeling quantitative perfusion imaging and a newly developed procedure to identify a specific role for the dorsal posterior insula (dpIns) in pain. Tract tracing studies in animals identify a similar region as fundamental to nociception, which suggests the dpIns is its human homolog and, as such, a potential therapeutic target.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


Change history
26 March 2015
In the version of this article initially published, the labels were reversed for the solid and dotted lines in Figure 2c. The error has been corrected in the HTML and PDF versions of the article.
References
Rainville, P. et al. Science 277, 968–971 (1997).
Ploghaus, A. et al. Science 284, 1979–1981 (1999).
Wiech, K. et al. J. Neurosci. 30, 16324–16331 (2010).
Wager, T.D. et al. N. Engl. J. Med. 368, 1388–1397 (2013).
Denk, F., McMahon, S.B. & Tracey, I. Nat. Neurosci. 17, 192–200 (2014).
Mouraux, A. et al. Neuroimage 54, 2237–2249 (2011).
Craig, A.D. Comp. Neurol. 522, 36–63 (2014).
Evrard, H.C., Logothetis, N.K. & Craig, A.D. J. Comp. Neurol. 522, 64–97 (2014).
Brooks, J.C. et al. Neuroimage 27, 201–209 (2005).
Henderson, L.A. et al. Pain 128, 20–30 (2007).
Baumgärtner, U. et al. J. Neurophysiol. 104, 2863–2872 (2010).
Mazzola, L. et al. Pain 146, 99–104 (2009).
Garcia-Larrea, L. et al. Brain 133, 2528–2539 (2010).
Greenspan, J.D., Lee, R.R. & Lenz, F.A. Pain 81, 273–282 (1999).
Garcia-Larrea, L. & Peyron, R. Pain 154, S29–S43 (2013).
Mezue, M. et al. J. Cereb. Blood Flow Metab. 34, 1919–1927 (2014).
Smith, S.M. et al. Neuroimage 23 (suppl. 1), S208–S219 (2004).
Buxton, R.B. & Frank, L. J. Cereb. Blood Flow Metab. 17, 64–72 (1997).
Chappell, M. et al. IEEE Trans. Signal Process 57, 223–236 (2009).
Acknowledgements
We would also like to acknowledge F. Eippert, K. Wiech and M. Chappell for their insights into the work. The research was funded by the Medical Research Council of Great Britain and Northern Ireland, the National Institute for Health Research Oxford Biomedical Research Centre, the Wellcome Trust, and the Innovative Medicines Initiative joint undertaking, under grant agreement no 115007, resources of which are composed of financial contribution from the European Union's Seventh Framework Programme (FP7/2007-2013) and European Federation of Pharmaceutical Industries and Associations (EFPIA) companies' in-kind contribution.
Author information
Authors and Affiliations
Contributions
All authors designed the study. A.R.S., M.M. and J.T.F. collected the data. A.R.S. and M.M. analyzed the data. All authors interpreted the data. A.R.S., M.M. and I.T. wrote the manuscript. All authors contributed to the revisions.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Integrated supplementary information
Supplementary Figure 1 Innocuous, ongoing vibration induced CBF changes.
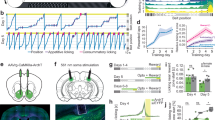
a) Schematic of the vibration scan paradigm design that consisted of two identical multi-TI pCASL scans (parameters identical to those described in the methods section). The baseline scan consisted of no vibration stimulation (grey); while the vibration scan (blue) consisted of a continuously oscillating non-noxious stimulation of the subject’s foot for the duration of the 7min scan. To minimize habituation effects, the vibration stimulus frequency was oscillated between 1-2.0 Hz (fixed amplitude of 1mA) using 0.5Hz step changes, at pseudorandom intervals between 20-60 seconds. Subjects were prompted to rate the stimulus intensity using a COVAS scale as discussed previously. None of the subjects reported the vibration stimulation as painful (group mean pain intensity = 0). The group mean vibration saliency rating for the full vibration scan was 3.12 (s.e.m. =0.265). For clarity, a plot of vibration frequency over time is displayed in Figure (a) above. b) No significant correlation was observed between absolute CBF and either the ongoing vibration intensity levels applied or with the ongoing perceived stimulus intensity levels reported by the subjects (Mixed Effects, z>2.3, p<0.05; cluster corrected; n=12). However, sub-threshold activation clusters are visible within the contralateral medial operculum; a subsection of the "posterior insular and adjoining medial operculum" (PIMO) region that Garcia-Larrea and others have highlighted as being linked to non-noxious sensory processing. For clarity, the non-significant sub-threshold clusters are shown in (b): red pixels represent the absolute CBF increases correlated with the ongoing vibration stimulus intensity applied to the subject’s foot (i.e. stimulus frequency). Blue pixels represent the absolute CBF increases correlated with the perceived stimulus intensity ratings reported by the subjects. The cluster in green represents the peak dpIns cluster that shows a strong positive correlation with ongoing pain intensity reported in the current study. Statistical maps were overlaid on selected slices of the MNI brain. Radiological convention is used (L: left; R: right).
Supplementary Figure 2 Peak pain period perfusion changes.
Absolute CBF changes during the 7-minute peak of the pain experience (peak pain period only vs baseline; Mixed Effects: z>2.3,p<0.05). Statistical maps were overlaid on selected slices of the MNI brain. Radiological convention is used. Orange pixels represent supra-threshold absolute CBF increases while blue pixels represent decreases. The anatomical locations for significant changes in CBF are listed in Supplementary table 2. These data highlight that the peak capsaicin pain relative to baseline is linked to positive and negative perfusion changes in a select group of brain regions, some of which have been previously shown as involved in pain processing (ref. 5 and Baliki, M.N. et al. Nat. Neurosci. 15, 1117–1119, 2012). Importantly, the region that shows maximal hyper-perfusion during the ‘peak pain’ compared to baseline is localized to the contralateral dpIns (mean CBF change ± s.e.m; 15 ± 4.1% or 6.9 ± 1.9 ml / 100 g blood / min). This data supports the results from the regression analysis displayed in Figure 2; where the dpIns cluster reaches a peak of activity at the time point of maximum capsaicin-induced pain. Importantly, none of the other regions identified here show a significant correlation with the ongoing pain ratings, as we found was the case for the dpIns, even with a less strict statistical threshold. Radiological convention is used. L, left; R, right; dpIns, dorsal posterior insula; Ant. Ins, anterior insula; NAc, nucleus accumbens; PCC, posterior cingulate.
Supplementary information
Supplementary Text and Figures
Supplementary Figures 1 and 2 and Supplementary Tables 1 and 2 (PDF 3281 kb)
Rights and permissions
About this article

Cite this article
Segerdahl, A., Mezue, M., Okell, T. et al. The dorsal posterior insula subserves a fundamental role in human pain. Nat Neurosci 18, 499–500 (2015). https://doi.org/10.1038/nn.3969
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nn.3969
This article is cited by
-
Post-injury pain and behaviour: a control theory perspective
Nature Reviews Neuroscience (2023)
-
Pain-preferential thalamocortical neural dynamics across species
Nature Human Behaviour (2023)
-
A sleep-active basalocortical pathway crucial for generation and maintenance of chronic pain
Nature Neuroscience (2023)
-
Optogenetic Inhibition of Glutamatergic Neurons in the Dysgranular Posterior Insular Cortex Modulates Trigeminal Neuropathic Pain in CCI-ION Rat
NeuroMolecular Medicine (2023)
-
A systematic review and meta-analysis of voxel-based morphometric studies of migraine
Journal of Neurology (2023)
