
A technique called somatic-cell nuclear transfer has been applied to human oocytes, resulting in the generation of personalized stem cells, albeit genetically abnormal ones. Two experts discuss the biomedical significance of this work and the ethical issues surrounding the use of human oocytes in research. See Article p.70
The paper in brief
-
Somatic-cell nuclear transfer (SCNT) involves replacing the genome of an oocyte with that of an adult cell.
-
Once the 'reconstructed' cell has developed into a blastocyst (a mass of 70–100 cells), stem-cell lines can be derived.
-
Human oocytes manipulated by SCNT do not develop to the blastocyst stage.
-
To overcome this problem, Noggle et al.1 (page 70) added the nucleus of a differentiated adult cell to an oocyte that still contained its nucleus (Fig. 1).
Figure 1: Three genomes are better than two? 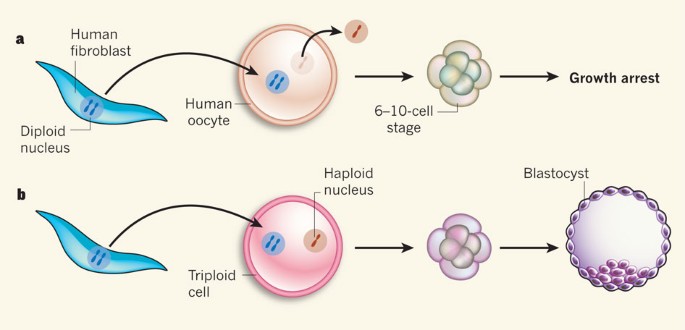
a, Typically, when the diploid nucleus of a differentiated adult human cell such as a skin fibroblast is transferred into a nucleus-free human oocyte, the resulting cell does not develop to the desired blastocyst stage. b, Noggle and colleagues1 show that leaving the haploid nucleus of the oocyte behind results in the generation of triploid cells that develop to the blastocyst stage. The authors isolated stem cells from these blastocysts (not shown) and found that the derived cells could differentiate into various cell types.
-
This allowed growth to the blastocyst stage, but, undesirably, the resulting cells had three genome copies — one from the haploid oocyte and two from the diploid differentiated cell.
-
Nonetheless, the adult genome copies reverted to gene-expression programs characteristic of embryonic stem cells.
-
Moreover, the stem cells isolated from the blastocysts could differentiate into cells of all three germ layers, from which all the tissues and organs of the body develop.
-
Noggle and colleagues paid women for their oocytes.
-
There are significant legal and social concerns about obtaining human oocytes for research and even therapy.

Imperfect yet striking
George Q. Daley
Noggle and colleagues' study1 is noteworthy for generating the first — albeit genetically abnormal — human pluripotent stem cells through oocyte-mediated reprogramming and for highlighting major technical barriers to SCNT using human eggs.
Since the first isolation of human embryonic stem (ES) cells in 1998, a compelling strategy for the future envisaged exploiting SCNT to generate personalized embryonic stem cells. The aim has been to reprogram a patient's differentiated cells to pluripotency — the potential to produce any tissue — and then to coax the resulting SCNT-ES cells to develop into disease-relevant cells, either for mechanistic studies or for combined gene and cell therapy2. Realistically, however, SCNT is a cumbersome process that cannot be readily scaled to allow widespread therapeutic use.
One breakthrough was the discovery that skin cells can be reprogrammed to a pluripotent state by enforced expression of only four transcription factors linked to pluripotency in ES cells3. The resulting induced pluripotent stem (iPS) cells, whether mouse or human, are functionally comparable to ES cells and provide an alternative to SCNT for generating personalized stem cells for disease modelling or cell-based therapies free of the problems of rejection.
Despite enthusiasm for iPS cells, however, closer scrutiny of their genetic integrity and differentiation behaviour has revealed subtle yet potentially significant differences from ES cells. As well as provoking rogue genetic changes, reprogramming can leave vestiges of the original differentiated (somatic) cell's identity — known as epigenetic memory — through faulty remodelling of chemical modifications on DNA and its associated proteins4.
Although it is premature to conclude that these foibles of iPS cells pose insurmountable risks, comparative studies of mouse stem cells suggest that SCNT may be more effective than forced expression of transcription factors in reprogramming cells to a pristine state of pluripotency and erasing epigenetic memory5,6. But until now, discussions of the relative merits of human SCNT-ES cells and iPS cells have been purely theoretical: although successful in non-human primates7, the generation of ES cells through SCNT has thus far failed in humans, largely because human oocytes have not been readily available for research.
With the advantage of ready access to a large number (270) of donor oocytes, Noggle et al.1 performed a rigorous exploration of SCNT and identified obstacles to the generation of normal human blastocysts by this technique. The researchers found that products of SCNT in humans stop dividing at the 6–10-cell stage, because removal of the oocyte genome apparently depletes the cell of factors that are essential for embryonic cell division or expression of genes from the somatic genome. Frustratingly, they could not overcome this cleavage arrest unless they left the oocyte genome in place; the cells they derived from the resulting blastocysts were therefore triploid somatic–oocyte pluripotent stem cells. Nonetheless, the authors' sophisticated analysis revealed that the transplanted genome was fully reprogrammed, with no signs of epigenetic memory. Thus, although falling short of its ultimate goal, the paper1 stands as a stepping stone towards success, and raises the provocative question of how human SCNT-ES cells might perform relative to iPS cells.
Persons versus things
Jan Helge Solbakk
What are oocytes? What is their nature? What conceptual labels should be attached to such entities? What regulatory frameworks should be in place to regulate their procurement for reproduction or research? And how should such transactions be acknowledged? These are some of the questions that came to my mind when reading Noggle and colleagues' paper1.
Since the time of Roman law, legal thinking has operated with a fundamental distinction between person and thing. Even today, the entities subject to regulation are either persons or things, and there is no third option8. This conceptual lacuna continues to generate regulatory paradoxes in the health and life sciences, because many of the entities subject to regulation — including bodies, body parts, organs and tissues, and sperm and oocytes — cannot be considered either persons or mere things.
How, then, should researchers proceed to procure oocytes? The approach Noggle et al. have taken is to pay 16 women for their oocytes and acknowledge their contribution as study participants. I believe this is a step in the right direction for three reasons: first, it transfers the focus from the entities procured to the subjects providing them; second, this refocusing avoids reducing the oocytes to mere things or commodities open for transactions according to the rules of the market; and finally, the word 'participation' paves the way for acknowledging the women's contribution as a piece of work for which they should be duly paid.
The standard argument against paying gamete donors is that the contribution is only material — and therefore marginal — compared with that of the researchers involved. But whether a differential valuation between intellectual input and input of a material or manual kind is justified is questionable. As bioethicist Søren Holm wrote9: “In a future situation where there are many groups deriving stem cells, and many donors providing embryos or gametes for the derivation, everyone's contributions will be equally accidental and contingent...”. If one group of accidental contributors (the researchers) is entitled to benefit financially from their contribution, why deny payment to another group of accidental contributors (the oocyte providers) for their work?
Another argument against paying oocyte providers is that this would undermine the voluntary nature of the consent process and give an undue incentive to participate in such research10. This argument also seems to be based on questionable grounds, because the prospect of obtaining future financial benefits from participating in research may also represent a sort of undue inducement for the researchers. Besides, an indication that the women involved in the present study1 did not necessarily participate for financial gain is that they were all fully employed.
The way Noggle et al.1 have chosen to deal with the oocyte issue does not comply neatly with existing regulatory guidelines in the field of stem-cell research. For this, in my view, they deserve praise rather than criticism, because their approach helps to draw attention to a possible way out of the regulatory quagmire resulting from reduction of oocyte providers to 'donors' or 'gift givers' deserving merely compensation for their gifts. The authors' approach represents the first step towards acknowledging women as genuine participants — co-producers even — in the generation of new knowledge.
References
Noggle, S. et al. Nature 478, 70–75 (2011).
Rideout, W. M. et al. Cell 109, 17–27 (2002).
Takahashi, K. & Yamanaka, S. Cell 126, 663–676 (2006).
Pera, M. F. Nature 471, 46–47 (2011).
Brambrink, T., Hochedlinger, K., Bell, G. & Jaenisch, R. Proc. Natl Acad. Sci. USA 103, 933–938 (2006).
Kim, K. et al. Nature 467, 285–290 (2010).
Byrne, J. A. et al. Nature 450, 497–502 (2007).
Lobato de Faria, P. in The Ethics of Research Biobanking (eds Solbakk, J. H., Holm, S. & Hofmann, B.) 263–276 (Springer, 2009).
Holm, S. J. Bioeth. Inquiry 3, 55–68 (2006).
Hyun, I. Nature 442, 629–630 (2006).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
G.Q.D. is a member of the scientific advisory boards and receives consulting fees or holds equity in the following companies: iPierian, Verastem, Epizyme, Solasia, Johnson & Johnson and MPM Capital.
Rights and permissions
About this article
Cite this article
Daley, G., Solbakk, J. Triple genomes go far. Nature 478, 40–41 (2011). https://doi.org/10.1038/478040a
Published:
Issue Date:
DOI: https://doi.org/10.1038/478040a
This article is cited by
-
Finding a home for nuclear transfer
Science-Business eXchange (2013)
