Abandoned
The human cost of neurotechnology failure
When the makers of electronic implants abandon their projects, people who rely on the devices have everything to lose.


Markus Möllmann-Bohle’s left cheek hides a secret that has changed his life. Under the skin, nestled among the nerve fibres that allow him to feel and move his face, is a miniature radio receiver and six tiny electrodes. “I’m a cyborg,” he says, with a chuckle.
This electronic device lies dormant much of the time. But, when Möllmann-Bohle feels pressure starting to gather around his left eye, he retrieves a black plastic wand about the size of a mobile phone, pushes a button and fixes it against his face in a home-made sling. The remote vibrates for a moment, then launches high-frequency radio waves into his cheek.
In response, the implant fires a sequence of electrical pulses into a bundle of nerve cells called the sphenopalatine ganglion. By disrupting these neurons, the device spares 57-year-old Möllmann-Bohle the worst of the agonizing cluster headaches that have plagued him for decades. He uses the implant several times a day. “I need this device to live a good life,” he says.
Cluster headaches are rare, but extraordinarily painful. People are typically affected for life and treatment options are very limited. Möllmann-Bohle experienced his first in 1987 at the age of 22. For decades, he managed sporadic headaches with a mix of painkillers and migraine medication. But in 2006, his condition became chronic, and he would be struck with as many as eight hour-long cluster headaches every day. “I was forced to succumb to the pain again and again,” he says. “I was kept from living my life.”


This article is part of Nature Outlook: Robotics and artificial intelligence, an editorially independent Nature supplement produced with the financial support of third parties. About this content.
This article is part of Nature Outlook: Robotics and artificial intelligence, an editorially independent Nature supplement produced with the financial support of third parties. About this content.
“I was forced to succumb to the pain again and again. I was kept from living my life.”
Möllmann-Bohle, evermore reliant on painkillers and now also taking antidepressants, was hospitalized numerous times. During one of these stays, however, he heard about an electronic implant that some people had started using to control their cluster headaches.
Developed by the start-up Autonomic Technologies (known as ATI) in San Francisco, California, the device had passed a series of placebo-controlled clinical trials with flying colours. “It worked remarkably well,” says Arne May, a neurologist at the University of Hamburg in Germany who led some of those trials on behalf of the start-up. In most people, stimulation reduced the pain of an attack, made attacks less frequent, or both1. Side effects were rare. In February 2012, while US trials continued, the European Medicines Agency granted the company approval to market the device across Europe.
Möllmann-Bohle contacted May, and travelled from his home near Düsseldorf, Germany, to meet him. Filled with hope that this might alleviate his suffering, Möllmann-Bohle underwent surgery to have the device fitted in 2013.
“Once the stimulator was working well, it felt like a rebirth” — Markus Möllmann-Bohle
The implant was a revelation. After the pattern and strength of the stimulation had been tailored to Möllmann-Bohle’s needs, around an hour’s use five or six times a day was enough to prevent attacks from becoming debilitating. “I was reborn,” he says.
But, by the end of 2019, ATI had collapsed. The company’s closure left Möllmann-Bohle and more than 700 other people alone with a complex implanted medical device. People using the stimulator and their physicians could no longer access the proprietary software needed to recalibrate the device and maintain its effectiveness. Möllmann-Bohle and his fellow users now faced the prospect of the battery in the hand-held remote wearing out, robbing them of the relief that they had found. “I was left standing in the rain,” Möllmann-Bohle says.
Markus Möllmann-Bohle’s left cheek hides a secret that has changed his life. Under the skin, nestled among the nerve fibres that allow him to feel and move his face, is a miniature radio receiver and six tiny electrodes. “I’m a cyborg,” he says, with a chuckle.
This electronic device lies dormant much of the time. But, when Möllmann-Bohle feels pressure starting to gather around his left eye, he retrieves a black plastic wand about the size of a mobile phone, pushes a button and fixes it against his face in a home-made sling. The remote vibrates for a moment, then launches high-frequency radio waves into his cheek.
In response, the implant fires a sequence of electrical pulses into a bundle of nerve cells called the sphenopalatine ganglion. By disrupting these neurons, the device spares 57-year-old Möllmann-Bohle the worst of the agonizing cluster headaches that have plagued him for decades. He uses the implant several times a day. “I need this device to live a good life,” he says.

This article is part of Nature Outlook: Robotics and artificial intelligence, an editorially independent Nature supplement produced with the financial support of third parties. About this content.
This article is part of Nature Outlook: Robotics and artificial intelligence, an editorially independent Nature supplement produced with the financial support of third parties. About this content.
Cluster headaches are rare, but extraordinarily painful. People are typically affected for life and treatment options are very limited. Möllmann-Bohle experienced his first in 1987 at the age of 22. For decades, he managed sporadic headaches with a mix of painkillers and migraine medication. But in 2006, his condition became chronic, and he would be struck with as many as eight hour-long cluster headaches every day. “I was forced to succumb to the pain again and again,” he says. “I was kept from living my life.”
Möllmann-Bohle, evermore reliant on painkillers and now also taking antidepressants, was hospitalized numerous times. During one of these stays, however, he heard about an electronic implant that some people had started using to control their cluster headaches.
“I was forced to succumb to the pain again and again. I was kept from living my life.”
Developed by the start-up Autonomic Technologies (known as ATI) in San Francisco, California, the device had passed a series of placebo-controlled clinical trials with flying colours. “It worked remarkably well,” says Arne May, a neurologist at the University of Hamburg in Germany who led some of those trials on behalf of the start-up. In most people, stimulation reduced the pain of an attack, made attacks less frequent, or both1. Side effects were rare. In February 2012, while US trials continued, the European Medicines Agency granted the company approval to market the device across Europe.
Möllmann-Bohle contacted May, and travelled from his home near Düsseldorf, Germany, to meet him. Filled with hope that this might alleviate his suffering, Möllmann-Bohle underwent surgery to have the device fitted in 2013.
“Once the stimulator was working well, it felt like a rebirth” — Markus Möllmann-Bohle
The implant was a revelation. After the pattern and strength of the stimulation had been tailored to Möllmann-Bohle’s needs, around an hour’s use five or six times a day was enough to prevent attacks from becoming debilitating. “I was reborn,” he says.
But, by the end of 2019, ATI had collapsed. The company’s closure left Möllmann-Bohle and more than 700 other people alone with a complex implanted medical device. People using the stimulator and their physicians could no longer access the proprietary software needed to recalibrate the device and maintain its effectiveness. Möllmann-Bohle and his fellow users now faced the prospect of the battery in the hand-held remote wearing out, robbing them of the relief that they had found. “I was left standing in the rain,” Möllmann-Bohle says.
A systemic problem


Hundreds of thousands of people benefit from implanted neurotechnology every day. Among the most common devices are spinal-cord stimulators, first commercialized in 1968, that help to ease chronic pain. Cochlear implants that provide a sense of hearing, and deep-brain stimulation (DBS) systems that quell the debilitating tremor of Parkinson’s disease, are also established therapies.
Encouraged by these successes, and buoyed by advances in computing and engineering, researchers are trying to develop evermore sophisticated devices for numerous other neurological and psychiatric conditions. Rather than simply stimulating the brain, spinal cord or peripheral nerves, some devices now monitor and respond to neural activity.
For example, in 2013, the US Food and Drug Administration approved a closed-loop system for people with epilepsy. The device detects signs of neural activity that could indicate a seizure and stimulates the brain to suppress it. Some researchers are aiming to treat depression by creating analogous devices that can track signals related to mood. And systems that allow people who have quadriplegia to control computers and prosthetic limbs using only their thoughts are also in development and attracting substantial funding.
The market for neurotechnology is predicted to expand by around 75% by 2026, to US$17.1 billion. But as commercial investment grows, so too do the instances of neurotechnology companies giving up on products or going out of business, abandoning the people who have come to depend on their devices.


Electrodes implanted in the brain can help to control the tremors associated with Parkinson’s disease. Credit: Zephyr/Science Photo Library
Electrodes implanted in the brain can help to control the tremors associated with Parkinson’s disease. Credit: Zephyr/Science Photo Library


Retinal implants by the company Second Sight were fitted in hundreds of people before the firm ended support for the product. Credit: Philippe Psaila / Science Photo Library
Retinal implants by the company Second Sight were fitted in hundreds of people before the firm ended support for the product. Credit: Philippe Psaila / Science Photo Library
Shortly after the demise of ATI, a company called Nuvectra, which was based in Plano, Texas, filed for bankruptcy in 2019. Its device — a new kind of spinal-cord stimulator for chronic pain — had been implanted in at least 3,000 people. In 2020, artificial-vision company Second Sight, in Sylmar, California, laid off most of its workforce, ending support for the 350 or so people who were using its much heralded retinal implant to see. And in June, another manufacturer of spinal-cord stimulators — Stimwave in Pompano Beach, Florida — filed for bankruptcy. The firm has been bought by a credit-management company and is now embroiled in a legal battle with its former chief executive. Thousands of people with the stimulator, and their physicians, are watching on in the hope that the company will continue to operate.
When the makers of implanted devices go under, the implants themselves are typically left in place — surgery to remove them is often too expensive or risky, or simply deemed unnecessary. But without ongoing technical support from the manufacturer, it is only a matter of time before the programming needs to be adjusted or a snagged wire or depleted battery renders the implant unusable.
People are then left searching for another way to manage their condition, but with the added difficulty of a non-functional implant that can be an obstacle both to medical imaging and future implants. For some people, including Möllmann-Bohle, no clear alternative exists.
“It’s a systemic problem,” says Jennifer French, executive director of Neurotech Network, a patient advocacy and support organization in St. Petersburg, Florida. “It goes all the way back to clinical trials, and I don’t think it’s received enough attention.”
As money pours into the neurotechnology sector, implant recipients, physicians, biomedical engineers and medical ethicists are all calling for action to protect people with neural implants. “Unfortunately, with that kind of investment, come failures,” says Gabriel Lázaro-Muñoz, an ethicist specializing in neurotechnology at Harvard Medical School in Boston, Massachusetts. “We need to figure out a way to minimize the harms that patients will endure because of these failures.”
Hundreds of thousands of people benefit from implanted neurotechnology every day. Among the most common devices are spinal-cord stimulators, first commercialized in 1968, that help to ease chronic pain. Cochlear implants that provide a sense of hearing, and deep-brain stimulation (DBS) systems that quell the debilitating tremor of Parkinson’s disease, are also established therapies.
Encouraged by these successes, and buoyed by advances in computing and engineering, researchers are trying to develop evermore sophisticated devices for numerous other neurological and psychiatric conditions. Rather than simply stimulating the brain, spinal cord or peripheral nerves, some devices now monitor and respond to neural activity.
For example, in 2013, the US Food and Drug Administration approved a closed-loop system for people with epilepsy. The device detects signs of neural activity that could indicate a seizure and stimulates the brain to suppress it. Some researchers are aiming to treat depression by creating analogous devices that can track signals related to mood. And systems that allow people who have quadriplegia to control computers and prosthetic limbs using only their thoughts are also in development and attracting substantial funding.
The market for neurotechnology is predicted to expand by around 75% by 2026, to US$17.1 billion. But as commercial investment grows, so too do the instances of neurotechnology companies giving up on products or going out of business, abandoning the people who have come to depend on their devices.

Electrodes implanted in the brain can help to control the tremors associated with Parkinson’s disease. Credit: Zephyr/Science Photo Library
Electrodes implanted in the brain can help to control the tremors associated with Parkinson’s disease. Credit: Zephyr/Science Photo Library
Shortly after the demise of ATI, a company called Nuvectra, which was based in Plano, Texas, filed for bankruptcy in 2019. Its device — a new kind of spinal-cord stimulator for chronic pain — had been implanted in at least 3,000 people. In 2020, artificial-vision company Second Sight, in Sylmar, California, laid off most of its workforce, ending support for the 350 or so people who were using its much heralded retinal implant to see. And in June, another manufacturer of spinal-cord stimulators — Stimwave in Pompano Beach, Florida — filed for bankruptcy. The firm has been bought by a credit-management company and is now embroiled in a legal battle with its former chief executive. Thousands of people with the stimulator, and their physicians, are watching on in the hope that the company will continue to operate.
When the makers of implanted devices go under, the implants themselves are typically left in place — surgery to remove them is often too expensive or risky, or simply deemed unnecessary. But without ongoing technical support from the manufacturer, it is only a matter of time before the programming needs to be adjusted or a snagged wire or depleted battery renders the implant unusable.
People are then left searching for another way to manage their condition, but with the added difficulty of a non-functional implant that can be an obstacle both to medical imaging and future implants. For some people, including Möllmann-Bohle, no clear alternative exists.

Retinal implants by the company Second Sight were fitted in hundreds of people before the firm ended support for the product. Credit: Philippe Psaila / Science Photo Library
Retinal implants by the company Second Sight were fitted in hundreds of people before the firm ended support for the product. Credit: Philippe Psaila / Science Photo Library
“It’s a systemic problem,” says Jennifer French, executive director of Neurotech Network, a patient advocacy and support organization in St. Petersburg, Florida. “It goes all the way back to clinical trials, and I don’t think it’s received enough attention.”
As money pours into the neurotechnology sector, implant recipients, physicians, biomedical engineers and medical ethicists are all calling for action to protect people with neural implants. “Unfortunately, with that kind of investment, come failures,” says Gabriel Lázaro-Muñoz, an ethicist specializing in neurotechnology at Harvard Medical School in Boston, Massachusetts. “We need to figure out a way to minimize the harms that patients will endure because of these failures.”
Left to their own devices


When Möllmann-Bohle had the ATI-made neurostimulator implanted to help with his cluster headaches, he agreed to participate in a five-year post-approval trial aimed at refining the device. He diligently provided ATI with data from his device and answered questionnaires about his progress. Every few months he made an 800-kilometre round trip to Hamburg to be assessed.
But four years in, the company running the trial on behalf of ATI called Möllmann-Bohle to tell him it was over. Rumours spread that the firm was in trouble, before a letter from May confirmed his fears — ATI had gone out of business.
Timothy White, another recipient of the company’s stimulator who took part in the post-approval trial, also heard of ATI’s closure second-hand.
Now head of clinical affairs for a medical-device company based near Frankfurt, White credits the device with allowing him to complete his medical training. Indeed, ATI had seized on this eloquent medical student’s enthusiasm for its technology and asked him to speak at conferences and to investors.
Yet even White heard about the company’s collapse only when he contacted May with concerns that his remote control might be under-performing.
“That was really rough for me,” says White. “I was asking myself, what’s going to happen if I lose my remote control, if it breaks down, or the battery dies. But no one really had answers.”
LISTEN: Timothy White shares his experience using ATI’s implant to suppress his cluster headaches.
LISTEN: Timothy White shares his experience using ATI’s implant to suppress his cluster headaches.
LISTEN: Pain specialist Anjum Bux on caring for patients following Nuvectra’s demise.
LISTEN: Pain specialist Anjum Bux on caring for patients following Nuvectra’s demise.
When an implant manufacturer disappears, what happens to the people using its devices varies hugely.
In some cases, there will be alternatives available. When Nuvectra folded, for example, users of its spinal-cord stimulator who feared a resurgence of their chronic pain could turn to similar devices offered by more established companies.
Even this best-case scenario puts considerable strain on the people using the implants, many of whom are already vulnerable, says anaesthesiologist Anjum Bux. He estimates that around 70 people received the Nuvectra device at his pain-management clinics in Kentucky.
Replacing obsolete implants of this kind requires surgery that would otherwise have been unnecessary and takes weeks to recover from. And at around US$40,000 for the surgery and replacement device, it’s also costly — although Bux says that in his experience, insurance providers have picked up the tab.
A greater challenge arises when no ready replacement is available. The stimulator made by ATI that Möllmann-Bohle and White have was the first of its kind. When the manufacturer closed its doors, there was no other implant on the market that they could use to manage their cluster headaches.
Left to fend for themselves, White and Möllmann-Bohle each leant on their own professional expertise. White drew on his medical training and found a drug, developed for treating migraines, that suppresses his headaches. But he must take triple the recommended dose, and worries about potential long-term side effects.
Möllmann-Bohle, meanwhile, turned to skills he developed as an electrical engineer. In the past three years, he has repaired a faulty charging port on the hand-held portion of his device and replaced its inbuilt battery several times. This battery was never intended to be accessible to the user, and it turned out to be unusual. Möllmann-Bohle scoured the Internet and eventually found suitable replacements made by a firm in the United States. When he returned for more, however, he learnt that the company had stopped making them. His most recent replacement came from a Chinese company that custom made what he needed.
His tinkering brought him into conflict with his insurers, who initially advised him not to tamper with the device, but eventually agreed to foot the bill for the replacement parts, after he convinced them he was suitably qualified. “They put really big obstacles in my way, or at least they tried to,” Möllmann-Bohle says. But although his repairs have been successful so far, he knows that he does not have the tools or skills to fix everything that could go wrong.


Markus Möllmann-Bohle has relied on his engineering expertise to keep his device functioning. Credit: Nyani Quarmyne/Panos Pictures for Nature
Markus Möllmann-Bohle has relied on his engineering expertise to keep his device functioning. Credit: Nyani Quarmyne/Panos Pictures for Nature
“How would I be able to manage in the future without the company?” — Markus Möllmann-Bohle
Although maintaining the device has been tough, Möllmann-Bohle cannot see an alternative. “There is still no medication reliable enough to help me live a pain-free life without the device,” he says.
He and White are now placing much of their hope in the potential revival of ATI’s stimulator technology. In late 2020, a company now called Realeve, based in Effingham, Illinois, announced that it had acquired the patents for the device. The new company intends to market an essentially identical successor device in both the United States and Europe. In April 2021, Realeve attained FDA breakthrough status, which is intended to speed up access to medical devices in the United States.
Möllmann-Bohle and White both approached Realeve earlier this year, and corresponded with then-chief executive Jon Snyder directly, asking for assistance with their implants. So far, they have received none. In an e-mail to Nature in July, Snyder said: “Since we do not have FDA or CE mark approval yet, we are unable to market the therapy and provide support. However, we have investigated the options of providing support via compassionate use approvals in various markets.”
Möllmann-Bohle desperately wants this support to materialize. “He [Snyder] assured me that he and his staff are working on providing replacement parts,” he says. There have been changes at Realeve in recent months, with Snyder departing and a consulting firm taking temporary control of the business. But interim chief executive Peter Donato says that the company has now gained approval in Denmark to distribute replacement devices and software to existing users. He hopes that it can begin deliveries in the latter half of 2023, and says that it is also in talks with three other European countries. For Möllmann-Bohle and others in Germany, the wait goes on. “This new start has been in the making for years now,” he says.
“This new start has been in the making for years now. I'm hopeful, but I'm also a realist.”
When Möllmann-Bohle had the ATI-made neurostimulator implanted to help with his cluster headaches, he agreed to participate in a five-year post-approval trial aimed at refining the device. He diligently provided ATI with data from his device and answered questionnaires about his progress. Every few months he made an 800-kilometre round trip to Hamburg to be assessed.
But four years in, the company running the trial on behalf of ATI called Möllmann-Bohle to tell him it was over. Rumours spread that the firm was in trouble, before a letter from May confirmed his fears — ATI had gone out of business.
Timothy White, another recipient of the company’s stimulator who took part in the post-approval trial, also heard of ATI’s closure second-hand.
Now head of clinical affairs for a medical-device company based near Frankfurt, White credits the device with allowing him to complete his medical training. Indeed, ATI had seized on this eloquent medical student’s enthusiasm for its technology and asked him to speak at conferences and to investors.
Yet even White heard about the company’s collapse only when he contacted May with concerns that his remote control might be under-performing.
LISTEN: Timothy White shares his experience using ATI’s implant to suppress his cluster headaches.
LISTEN: Timothy White shares his experience using ATI’s implant to suppress his cluster headaches.
“That was really rough for me,” says White. “I was asking myself, what’s going to happen if I lose my remote control, if it breaks down, or the battery dies. But no one really had answers.”
When an implant manufacturer disappears, what happens to the people using its devices varies hugely.
In some cases, there will be alternatives available. When Nuvectra folded, for example, users of its spinal-cord stimulator who feared a resurgence of their chronic pain could turn to similar devices offered by more established companies.
Even this best-case scenario puts considerable strain on the people using the implants, many of whom are already vulnerable, says anaesthesiologist Anjum Bux. He estimates that around 70 people received the Nuvectra device at his pain-management clinics in Kentucky.
Replacing obsolete implants of this kind requires surgery that would otherwise have been unnecessary and takes weeks to recover from. And at around US$40,000 for the surgery and replacement device, it’s also costly — although Bux says that in his experience, insurance providers have picked up the tab.
LISTEN: Pain specialist Anjum Bux on caring for patients following Nuvectra’s demise.
LISTEN: Pain specialist Anjum Bux on caring for patients following Nuvectra’s demise.
A greater challenge arises when no ready replacement is available. The stimulator made by ATI that Möllmann-Bohle and White have was the first of its kind. When the manufacturer closed its doors, there was no other implant on the market that they could use to manage their cluster headaches.
Left to fend for themselves, White and Möllmann-Bohle each leant on their own professional expertise. White drew on his medical training and found a drug, developed for treating migraines, that suppresses his headaches. But he must take triple the recommended dose, and worries about potential long-term side effects.

Markus Möllmann-Bohle has relied on his engineering expertise to keep his device functioning. Credit: Nyani Quarmyne/Panos Pictures for Nature
Markus Möllmann-Bohle has relied on his engineering expertise to keep his device functioning. Credit: Nyani Quarmyne/Panos Pictures for Nature
Möllmann-Bohle, meanwhile, turned to skills he developed as an electrical engineer. In the past three years, he has repaired a faulty charging port on the hand-held portion of his device and replaced its inbuilt battery several times. This battery was never intended to be accessible to the user, and it turned out to be unusual. Möllmann-Bohle scoured the Internet and eventually found suitable replacements made by a firm in the United States. When he returned for more, however, he learnt that the company had stopped making them. His most recent replacement came from a Chinese company that custom made what he needed.
His tinkering brought him into conflict with his insurers, who initially advised him not to tamper with the device, but eventually agreed to foot the bill for the replacement parts, after he convinced them he was suitably qualified. “They put really big obstacles in my way, or at least they tried to,” Möllmann-Bohle says. But although his repairs have been successful so far, he knows that he does not have the tools or skills to fix everything that could go wrong.
“How would I be able to manage in the future without the company?” — Markus Möllmann-Bohle
Although maintaining the device has been tough, Möllmann-Bohle cannot see an alternative. “There is still no medication reliable enough to help me live a pain-free life without the device,” he says.
He and White are now placing much of their hope in the potential revival of ATI’s stimulator technology. In late 2020, a company now called Realeve, based in Effingham, Illinois, announced that it had acquired the patents for the device. The new company intends to market an essentially identical successor device in both the United States and Europe. In April 2021, Realeve attained FDA breakthrough status, which is intended to speed up access to medical devices in the United States.
“This new start has been in the making for years now. I'm hopeful, but I'm also a realist.”
Möllmann-Bohle and White both approached Realeve earlier this year, and corresponded with then-chief executive Jon Snyder directly, asking for assistance with their implants. So far, they have received none. In an e-mail to Nature in July, Snyder said: “Since we do not have FDA or CE mark approval yet, we are unable to market the therapy and provide support. However, we have investigated the options of providing support via compassionate use approvals in various markets.”
Möllmann-Bohle desperately wants this support to materialize. “He [Snyder] assured me that he and his staff are working on providing replacement parts,” he says. There have been changes at Realeve in recent months, with Snyder departing and a consulting firm taking temporary control of the business. But interim chief executive Peter Donato says that the company has now gained approval in Denmark to distribute replacement devices and software to existing users. He hopes that it can begin deliveries in the latter half of 2023, and says that it is also in talks with three other European countries. For Möllmann-Bohle and others in Germany, the wait goes on. “This new start has been in the making for years now,” he says.
A commitment to care


Examples of makers supporting implanted neurotechnology when profits fail to materialize are few and far between. French can therefore consider herself one of the lucky ones.
As well as being a prominent advocate for neurotechnology, she has been using an implanted device to help her move for more than 20 years — even though the life-changing technology never became the foundation of a viable business.
In 1999, two years after a snowboarding accident left her unable to move her legs, French enrolled in a clinical trial of an electrical implant system designed by Ronald Triolo, a biomedical engineer at Case Western Reserve University in Cleveland, Ohio.
Over seven and a half hours, surgeons placed 16 electrodes in her body, each of which could stimulate a nerve that runs to her leg muscles. These electrodes were connected to an implanted pulse generator, which is wirelessly powered and controlled by an external unit.
Initially, the implant allowed French to stand and move herself between her wheelchair and a bed or a car. Over time, more electrodes and controllers have been added. Now she can stand and step, and pedal a stationary bike. “I use it on a daily basis for exercise, for standing, for function,” she says.


Jennifer French was given an implanted device that helps her to stand as part of a clinical trial. Credit: Advanced Platform Technology Center
Jennifer French was given an implanted device that helps her to stand as part of a clinical trial. Credit: Advanced Platform Technology Center
”Within that instant, what you knew before then has completely changed” — Jennifer French

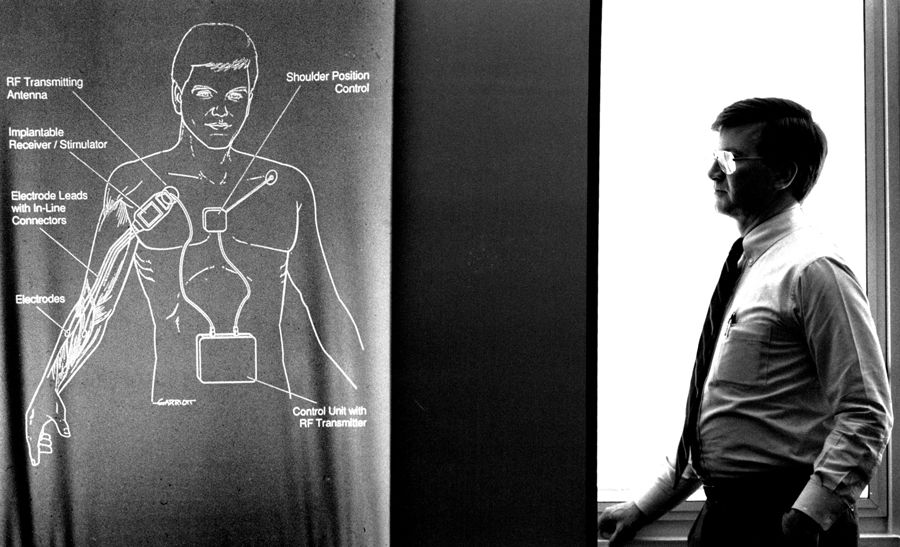
Hunter Peckham designed a device to restore hand and arm movement. Credit: Robert Pearce/Fairfax Media/Getty
Hunter Peckham designed a device to restore hand and arm movement. Credit: Robert Pearce/Fairfax Media/Getty
Although the device was not commercially available at the time French joined the trial, Triolo expected it wouldn’t be long before it was — a similar system developed at Case Western for restoring functional hand and arm movement, known as Freehand, had been brought to market by a local start-up in 1997.
But this did not come to pass. Despite the difference it has made to French’s life, the device she uses has never been commercialized. The company that had acquired the rights to the Freehand system shuttered in 2001, and no other company picked up the device. Freehand’s developer, biomedical engineer Hunter Peckham also at Case Western, attributes the start-up’s failure to impatient investors. “The uptake was not as fast as they would have liked,” he says.
Around 350 people with Freehand devices, as well as French and her fellow participants in Triolo’s lower-body implant trial, could have lost access to the technology that had become an integral part of their lives. But Peckham and Triolo refused to let this happen.
“We understood that if there was something that they were benefiting from, if you took that away that would be another loss for them — when they had had such a devastating loss before,” Peckham says.
Using old and dwindling stocks of components — including items that the university had acquired after the demise of the Freehand manufacturer — and tapping into money from academic grants, the researchers continue to support as many people with these devices as they can.
Over two decades, the Freehand devices have been repaired as they gradually failed, and funding for a succession of further fixed-term clinical trials has allowed Triolo to continue to support French and her fellow research participants. He has even been able to offer them upgrades over time. French’s system has failed four times, leaving her unable to stand and acutely aware of her reliance on the technology. Every time, the Case Western team has provided the surgery and parts required to restore her movement.
“Someone is dedicating their body to our research. We have an obligation to maintain their systems for as long as they want to use them.”
“We've invested in her, and she continues to invest her time and effort in advancing our science” — Ronald Triolo
French knows her situation is precarious and that it rests on Triolo continuing to attract funding. “I live every day with the fact that this technology might go away,” she says. But she takes heart in what she sees as the researchers’ unwavering commitment to her.
“Our world view,” Triolo says, “is someone is dedicating their body to help advance our research, and we have an obligation to them to maintain their systems for as long as they want to use them.”
Examples of makers supporting implanted neurotechnology when profits fail to materialize are few and far between. French can therefore consider herself one of the lucky ones.
As well as being a prominent advocate for neurotechnology, she has been using an implanted device to help her move for more than 20 years — even though the life-changing technology never became the foundation of a viable business.
In 1999, two years after a snowboarding accident left her unable to move her legs, French enrolled in a clinical trial of an electrical implant system designed by Ronald Triolo, a biomedical engineer at Case Western Reserve University in Cleveland, Ohio.

Jennifer French was given an implanted device that helps her to stand as part of a clinical trial. Credit: Advanced Platform Technology Center
Jennifer French was given an implanted device that helps her to stand as part of a clinical trial. Credit: Advanced Platform Technology Center
Over seven and a half hours, surgeons placed 16 electrodes in her body, each of which could stimulate a nerve that runs to her leg muscles. These electrodes were connected to an implanted pulse generator, which is wirelessly powered and controlled by an external unit.
Initially, the implant allowed French to stand and move herself between her wheelchair and a bed or a car. Over time, more electrodes and controllers have been added. Now she can stand and step, and pedal a stationary bike. “I use it on a daily basis for exercise, for standing, for function,” she says.
“Within that instant, what you knew before then has completely changed” — Jennifer French
Although the device was not commercially available at the time French joined the trial, Triolo expected it wouldn’t be long before it was — a similar system developed at Case Western for restoring functional hand and arm movement, known as Freehand, had been brought to market by a local start-up in 1997.
But this did not come to pass. Despite the difference it has made to French’s life, the device she uses has never been commercialized. The company that had acquired the rights to the Freehand system shuttered in 2001, and no other company picked up the device. Freehand’s developer, biomedical engineer Hunter Peckham also at Case Western, attributes the start-up’s failure to impatient investors. “The uptake was not as fast as they would have liked,” he says.

Hunter Peckham designed a device to restore hand and arm movement. Credit: Robert Pearce/Fairfax Media/Getty
Hunter Peckham designed a device to restore hand and arm movement. Credit: Robert Pearce/Fairfax Media/Getty
Around 350 people with Freehand devices, as well as French and her fellow participants in Triolo’s lower-body implant trial, could have lost access to the technology that had become an integral part of their lives. But Peckham and Triolo refused to let this happen.
“We understood that if there was something that they were benefiting from, if you took that away that would be another loss for them — when they had had such a devastating loss before,” Peckham says.
“Someone is dedicating their body to our research. We have an obligation to maintain their systems for as long as they want to use them.”
Using old and dwindling stocks of components — including items that the university had acquired after the demise of the Freehand manufacturer — and tapping into money from academic grants, the researchers continue to support as many people with these devices as they can.
Over two decades, the Freehand devices have been repaired as they gradually failed, and funding for a succession of further fixed-term clinical trials has allowed Triolo to continue to support French and her fellow research participants. He has even been able to offer them upgrades over time. French’s system has failed four times, leaving her unable to stand and acutely aware of her reliance on the technology. Every time, the Case Western team has provided the surgery and parts required to restore her movement.
”We've invested in her, and she continues to invest her time and effort in advancing our science” — Ronald Triolo
French knows her situation is precarious and that it rests on Triolo continuing to attract funding. “I live every day with the fact that this technology might go away,” she says. But she takes heart in what she sees as the researchers’ unwavering commitment to her.
“Our world view,” Triolo says, “is someone is dedicating their body to help advance our research, and we have an obligation to them to maintain their systems for as long as they want to use them.”
Protection from failure


Konstantin Slavin is a neurosurgeon at the University of Illinois College of Medicine in Chicago, who contributed to clinical trials of ATI’s cluster-headache device and implanted the spinal-cord stimulator made by Nuvectra. He thinks that anyone given an implanted device as a part of routine clinical care should be able to count on ongoing support. “You expect them to receive essentially lifelong care from the device manufacturer,” he says.
He is not alone in this view — every device user, physician and engineer Nature interviewed thinks that people need to be better protected from the failure of device makers.
“You expect them to receive essentially lifelong care from the device manufacturer.”
“Long-term support on the commercial side would be a competitive advantage” — Ronald Triolo
One proposal is that neurotechnology companies should ensure that there is money available to support the people using their devices in the event of the company’s closure. How this would best be achieved is uncertain. Suggestions include the company setting up a partner non-profit organization to manage funds to cover this eventuality; putting aside money in an escrow account; being obliged to take out an insurance policy that would support users; paying into a government-supported safety network; or ensuring the people using the devices are high-priority creditors during bankruptcy proceedings.
Currently, there is little sign that device makers are taking this kind of action. Asked in July if Realeve had plans in place to protect people should its business go the same way as ATI, Snyder, then chief executive, replied: “There is always the risk that a company may stop operating, but our focus is to be successful in our effort to deliver the Realeve Pulsante therapy to patients”.
Realeve’s interim chief executive Donato thinks that it will take legislation to convince investors or shareholders in companies to take on the expense of a safety net. “Unless, and until, the governments force it on us,” he says, “I’m not sure companies will do it on their own.” But Triolo is optimistic that manufacturers might think differently if the jeopardy faced by device users becomes more widely known, and physicians and prospective patients start to favour companies that do have a safety net in place. “If that is what it takes to have a competitive advantage, maybe that’ll be enlightening for our friends on the commercial side of things,” Triolo says.
Indeed, the failures of various neurotechnology start-ups over the past few years are already causing the surgeons responsible for implanting the devices to be cautious.
Robert Levy, a neurosurgeon in Boca Raton, Florida, and a former president of the International Neuromodulation Society, was particularly burnt by the demise of Nuvectra. He had been sufficiently impressed with its technology to become chairman of the company’s medical advisory board in August 2016. But in 2019, around five months before Nuvectra filed for bankruptcy, he cut ties after what he and others formerly associated with the firm saw as the company side-lining the needs of people using the implant in its attempt to stay afloat. “All of us who had any association with the company at that time expressed our severe dissatisfaction with such a move, which we felt was unethical,” Levy says.
“Making patients the victims of bad business practices or a bankruptcy is horrible for them, horrible for the field, and grossly unethical.”
“I learned that they completely abandoned the patients, and frankly I was horrified” — Robert Levy
From now on, Levy requires any new company that asks him to implant its product to send him a letter guaranteeing support for the people who have the surgery should something happen to the business. “If they should not supply such a letter, they’re not going to be included in my practice,” he says.
He plans to write an editorial arguing for this approach in the journal Neuromodulation, of which he is editor-in-chief, to further raise awareness and put pressure on neurotechnology companies. “Patients are suffering terribly,” he says. “Making them the victims of bad business practices or a bankruptcy is horrible for patients, horrible for the field and grossly unethical.”
Momentum is also building behind another way to protect people with implants: technical standardization. The electrodes, connectors, programmable circuits and power supplies used in implanted neurotechnology are often proprietary or otherwise difficult to source, as Möllmann-Bohle discovered when looking for replacement parts for his stimulator. If components were common across devices, one manufacturer might be able to step in and offer spares when another goes under.
A 2021 survey of surgeons who implant neurostimulators showed that 86% backed standardization of the connectors used by these devices2. Such a move would not be without precedent, says retired neurosurgeon and medical-device engineer Richard North, formerly at Johns Hopkins Medical School in Baltimore, and president of the Institute of Neuromodulation in Chicago, who led the survey. Cardiac pacemakers have included standardized elements since the early 1990s, when manufacturers voluntarily agreed to ensure that any company’s power supply could fuel a pacemaker from any other company. Many of those same companies are now the biggest names in spinal-cord stimulators and DBS systems.

Parts from cardiac pacemakers have been standardized since the 1990s. Credit: Louise Oligny/BSIP/Alamy
Parts from cardiac pacemakers have been standardized since the 1990s. Credit: Louise Oligny/BSIP/Alamy
“It’s inevitable that there will be standardization, and I think the companies involved recognize that too.”
North now co-chairs a Connector Standards Committee for the North American Neuromodulation Society, of which the Institute of Neuromodulation is a part, that is promoting the idea. Although the industry has not raced to embrace further standardization, he thinks it is only a matter of time. “It’s inevitable that there will be standardization, and I think the companies involved recognize that too,” he says. As well as making replacement components easier to come by, North thinks that standardization would boost innovation by encouraging companies to develop components that can be used with a wide range of existing systems.
Peckham hopes that the neurotechnology field can go even further — he wants devices to be made open source. Under the auspices of the Institute for Functional Restoration, a non-profit organization that he and his colleagues at Case Western established in 2013, Peckham plans to make the design specifications and supporting documentation of new implantable technologies developed by his team freely available. “Then people can just cut and paste,” he says.
This marks a major departure from the proprietary nature of most current devices. Peckham hopes that other people will build on the technology, and potentially even adapt it for new indications. The benefits for the people using these devices are at the centre of his thinking. “It starts with a commitment to the patients, to the people who can benefit from this,” he says.
It is exactly that sort of commitment that people such as Möllmann-Bohle, White and French want to see — and which they think they are entitled to. A raft of new companies are developing evermore sophisticated neurological implants with the power to transform people’s lives. Should any fail, it is the people using the devices, and their physicians, who will be most affected, says Triolo.
The recent run of commercial casualties demonstrates the human cost of abandoning neurotechnology. “It’s impossible,” Triolo says, “for people not to know that this is becoming a bigger and bigger issue.”
References
- J. Schoenen et al. Cephalalgia 33, 816–830 (2013). Article
- R. B. North et al. Neuromodulation 24, 1299–1306 (2021). Article
Author: Liam Drew
Design: Chris Ryan
Video: Josh Birt, Colin Kelly, Adam Levy
Original photography: Nyani Quarmyne
Audio: Adam Levy
Multimedia editors: Adam Levy, Dan Fox
Photo editors: Jessica Hallett, Madeline Hutchinson
Translation: Shaya Zarrin
Subeditor: Jenny McCarthy
Project manager: Rebecca Jones
Editor: Richard Hodson
Nature is pleased to acknowledge financial support from FII Institute in producing the above story. Nature retains sole responsibility for all editorial content. About this content.
The supporting organization retains sole responsibility for the following message:

FII Institute is a global non-profit foundation with an investment arm and one agenda: Impact on Humanity. Committed to ESG principles, we foster the brightest minds and transform ideas into real-world solutions in five focus areas: AI and Robotics, Education, Healthcare, and Sustainability.
We are in the right place at the right time – when decision makers, investors, and an engaged generation of youth come together in aspiration, energized and ready for change. We harness that energy into three pillars – THINK, XCHANGE, ACT – and invest in the innovations that make a difference globally.
Join us to own, co-create and actualize a brighter, more sustainable future for humanity.
Visit the FII Institute website.
Konstantin Slavin is a neurosurgeon at the University of Illinois College of Medicine in Chicago, who contributed to clinical trials of ATI’s cluster-headache device and implanted the spinal-cord stimulator made by Nuvectra. He thinks that anyone given an implanted device as a part of routine clinical care should be able to count on ongoing support. “You expect them to receive essentially lifelong care from the device manufacturer,” he says.
He is not alone in this view — every device user, physician and engineer Nature interviewed thinks that people need to be better protected from the failure of device makers.
“You expect them to receive essentially lifelong care from the device manufacturer.”
One proposal is that neurotechnology companies should ensure that there is money available to support the people using their devices in the event of the company’s closure. How this would best be achieved is uncertain. Suggestions include the company setting up a partner non-profit organization to manage funds to cover this eventuality; putting aside money in an escrow account; being obliged to take out an insurance policy that would support users; paying into a government-supported safety network; or ensuring the people using the devices are high-priority creditors during bankruptcy proceedings.
“Long-term support on the commercial side would be a competitive advantage” — Ronald Triolo
Currently, there is little sign that device makers are taking this kind of action. Asked in July if Realeve had plans in place to protect people should its business go the same way as ATI, Snyder, then chief executive, replied: “There is always the risk that a company may stop operating, but our focus is to be successful in our effort to deliver the Realeve Pulsante therapy to patients”.
Realeve’s interim chief executive Donato thinks that it will take legislation to convince investors or shareholders in companies to take on the expense of a safety net. “Unless, and until, the governments force it on us,” he says, “I’m not sure companies will do it on their own.” But Triolo is optimistic that manufacturers might think differently if the jeopardy faced by device users becomes more widely known, and physicians and prospective patients start to favour companies that do have a safety net in place. “If that is what it takes to have a competitive advantage, maybe that’ll be enlightening for our friends on the commercial side of things,” Triolo says.
Indeed, the failures of various neurotechnology start-ups over the past few years are already causing the surgeons responsible for implanting the devices to be cautious.
“Making patients the victims of bad business practices or a bankruptcy is horrible for them, horrible for the field, and grossly unethical.”
Robert Levy, a neurosurgeon in Boca Raton, Florida, and a former president of the International Neuromodulation Society, was particularly burnt by the demise of Nuvectra. He had been sufficiently impressed with its technology to become chairman of the company’s medical advisory board in August 2016. But in 2019, around five months before Nuvectra filed for bankruptcy, he cut ties after what he and others formerly associated with the firm saw as the company side-lining the needs of people using the implant in its attempt to stay afloat. “All of us who had any association with the company at that time expressed our severe dissatisfaction with such a move, which we felt was unethical,” Levy says.
From now on, Levy requires any new company that asks him to implant its product to send him a letter guaranteeing support for the people who have the surgery should something happen to the business. “If they should not supply such a letter, they’re not going to be included in my practice,” he says.
He plans to write an editorial arguing for this approach in the journal Neuromodulation, of which he is editor-in-chief, to further raise awareness and put pressure on neurotechnology companies. “Patients are suffering terribly,” he says. “Making them the victims of bad business practices or a bankruptcy is horrible for patients, horrible for the field and grossly unethical.”

Parts from cardiac pacemakers have been standardized since the 1990s. Credit: Louise Oligny/BSIP/Alamy
Parts from cardiac pacemakers have been standardized since the 1990s. Credit: Louise Oligny/BSIP/Alamy
Momentum is also building behind another way to protect people with implants: technical standardization. The electrodes, connectors, programmable circuits and power supplies used in implanted neurotechnology are often proprietary or otherwise difficult to source, as Möllmann-Bohle discovered when looking for replacement parts for his stimulator. If components were common across devices, one manufacturer might be able to step in and offer spares when another goes under.
A 2021 survey of surgeons who implant neurostimulators showed that 86% backed standardization of the connectors used by these devices2. Such a move would not be without precedent, says retired neurosurgeon and medical-device engineer Richard North, formerly at Johns Hopkins Medical School in Baltimore, and president of the Institute of Neuromodulation in Chicago, who led the survey. Cardiac pacemakers have included standardized elements since the early 1990s, when manufacturers voluntarily agreed to ensure that any company’s power supply could fuel a pacemaker from any other company. Many of those same companies are now the biggest names in spinal-cord stimulators and DBS systems.
“It’s inevitable that there will be standardization, and I think the companies involved recognize that too.”
North now co-chairs a Connector Standards Committee for the North American Neuromodulation Society, of which the Institute of Neuromodulation is a part, that is promoting the idea. Although the industry has not raced to embrace further standardization, he thinks it is only a matter of time. “It’s inevitable that there will be standardization, and I think the companies involved recognize that too,” he says. As well as making replacement components easier to come by, North thinks that standardization would boost innovation by encouraging companies to develop components that can be used with a wide range of existing systems.
Peckham hopes that the neurotechnology field can go even further — he wants devices to be made open source. Under the auspices of the Institute for Functional Restoration, a non-profit organization that he and his colleagues at Case Western established in 2013, Peckham plans to make the design specifications and supporting documentation of new implantable technologies developed by his team freely available. “Then people can just cut and paste,” he says.
This marks a major departure from the proprietary nature of most current devices. Peckham hopes that other people will build on the technology, and potentially even adapt it for new indications. The benefits for the people using these devices are at the centre of his thinking. “It starts with a commitment to the patients, to the people who can benefit from this,” he says.
It is exactly that sort of commitment that people such as Möllmann-Bohle, White and French want to see — and which they think they are entitled to. A raft of new companies are developing evermore sophisticated neurological implants with the power to transform people’s lives. Should any fail, it is the people using the devices, and their physicians, who will be most affected, says Triolo.
The recent run of commercial casualties demonstrates the human cost of abandoning neurotechnology. “It’s impossible,” Triolo says, “for people not to know that this is becoming a bigger and bigger issue.”
References
- J. Schoenen et al. Cephalalgia 33, 816–830 (2013). Article
- R. B. North et al. Neuromodulation 24, 1299–1306 (2021). Article
Author: Liam Drew
Design: Chris Ryan
Video: Josh Birt, Colin Kelly, Adam Levy
Original photography: Nyani Quarmyne
Audio: Adam Levy
Multimedia editors: Adam Levy, Dan Fox
Photo editors: Jessica Hallett, Madeline Hutchinson
Translation: Shaya Zarrin
Subeditor: Jenny McCarthy
Project manager: Rebecca Jones
Editor: Richard Hodson
Nature is pleased to acknowledge financial support from FII Institute in producing the above story. Nature retains sole responsibility for all editorial content. About this content.
The supporting organization retains sole responsibility for the following message:
FII Institute is a global non-profit foundation with an investment arm and one agenda: Impact on Humanity. Committed to ESG principles, we foster the brightest minds and transform ideas into real-world solutions in five focus areas: AI and Robotics, Education, Healthcare, and Sustainability.
We are in the right place at the right time – when decision makers, investors, and an engaged generation of youth come together in aspiration, energized and ready for change. We harness that energy into three pillars – THINK, XCHANGE, ACT – and invest in the innovations that make a difference globally.
Join us to own, co-create and actualize a brighter, more sustainable future for humanity.
Visit the FII Institute website.