
Abstract
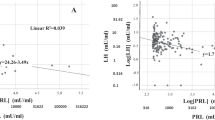
We have recently documented significantly reduced serum testosterone (T) levels in patients with erectile dysfunction (ED). To understand the mechanism of this hypotestosteronemia, which was independent of the etiology of ED, and its reversibility only in patients in whom a variety of nonhormonal therapies restored sexual activity, we measured serum luteinizing hormone (LH) in the same cohort of ED patients (n=83; 70% organic, 30% nonorganic). Both immunoreactive LH (I-LH) and bioactive LH (B-LH) were measured at entry and 3 months after therapy. Based on outcome (ie number of successful attempts of intercourse per month), patients were categorized as full responders (namely, at least eight attempts; n=51), partial responders (at least one attempt; n=20) and non-responders (n=16). Compared to 30 healthy men with no ED, baseline B-LH (mean±s.d.) in the 83 patients was decreased (13.6±5.5 vs 31.7±6.9 IU/L, P<0.001), in the face of a slightly increased, but in the normal range, I-LH (5.3±1.8 vs 3.4±0.9 IU/L, P<0.001); consequently, the B/I LH ratio was decreased (3.6±3.9 vs 9.7±3.3, P<0.001). Similar to our previous observation for serum T, the three outcome groups did not differ significantly for any of these three parameters at baseline. However, outcome groups differed after therapy. Bioactivity of LH increased markedly in full responders (pre-therapy=13.7±5.3, post-therapy=22.6±5.4, P<0.001), modestly in partial responders (14.8±6.9 vs 17.2±7.0, P<0.05) but remained unchanged in non-responders (11.2±2.2 vs 12.2±5.1). The corresponding changes went in the opposite direction for I-LH (5.2±1.7 vs 2.6±5.4, P<0.001; 5.4±2.2 vs 4.0±1.7, P<0.05; 5.6±1.2 vs 5.0±1.2, respectively), and in the same direction as B-LH for the B/I ratio (3.7±4.1 vs 11.8±7.8, P<0.001; 4.2±4.3 vs 5.8±4.2, P<0.05; 2.1±0.7 vs 2.6±1.3, respectively). We hypothesize that the hypotestosteronemia of ED patients is due to impaired bioactivity of LH. This reduced bioactivity is reversible, provided that resumption of sexual activity is achieved regardless of the therapeutic modality. Because biopotency of pituitary hormones is controlled by the hypothalamus, LH hypoactivity should be due to the hypothalamic functional damage associated to the psychological disturbances which unavoidably follow sexual inactivity.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 8 print issues and online access
$259.00 per year
only $32.38 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
NIH Consensus Development Panel on Impotence. JAMA 1993 270: 83–90.
Feldman HA et al . Impotence and its medical and psychological correlates: results of the Massachusetts Male Aging Study. J Urol 1994 151: 54–61.
Krane RJ, Goldstein I, Sanz de Tejada I. . Impotence. New Engl J Med 1989 321: 1648–1659.
Utiger RD. . A pill for impotence. Editorial. New Engl J Med 1998 338: 1458–1459.
Govier FE, Dale McClure R, Kramer-Levien D. . Endocrine screening for sexual dysfunction using free testosterone determinations. J Urol 1996 156: 405–408.
Johnson AR, Jarow JP. . Is routine endocrine testing of impotent men necessary? J Urol 1992 147: 1542–1543.
Jannini EA et al . Lack of sexual activity from erectile dysfunction is associated with a reversible reduction in serum testosterone. Int J Androl 1999 22: 385–392.
Dufau ML, Beitins IZ, McArthur JW, Catt KJ. . Effects of luteinizing hormone-releasing hormone (LHRH) upon bioactive and immunoreactive serum LH levels in normal subjects. J Clin Endocrinol Metab 1976 43: 658–667.
Rich BH, Rosenfield RL, Moll GW, Lucky AW. . Bioactive luteinizing hormone pituitary reserves during normal and abnormal male puberty. J Clin Endocrinol Metab 1982 1: 140–146.
Nagamani N, Osuampke C, Kelver ME. . Increased bioactive luteinizing hormone levels and Bio/Immuno ratio in women with hyperthecosis of the ovaries: possible role of hyperinsulinemia. J Clin Endocrinol Metab 1999 84: 1685–1689.
Katt KJ, Dufau ML. . Gonadotropic hormones: biosynthesis, secretion, receptors, and action. In: Yen SSC, Jaffe RB (eds). Reproductive Endocrinology. Saunders Co: Philadelphia 1991 105–155.
Fabbri A et al . Endorphins in male impotence: evidence for naltrexone stimulation of erectile activity in patient therapy. Psychoneuroendocrinology 1989 14: 103–111.
Heiman JR, Rowland DL. . Affective and psychological response patterns: the effect of instructions on sexually functional and dysfunctional men. J Psychosom Res 1983 27: 105–116.
Korenman SG. . Advances in the understanding and management of erectile dysfunction. J Clin Endocrinol Metab 1995 80: 1985–1988.
Dufau ML, Pock R, Neubauer A, Catt KJ. . In vitro bioassay of LH in human serum: the rat interstitial cell testosterone (RICT) assay. J Clin Endocrinol Metab 1977 42: 958–969.
Spratt D et al . WF. Bio- and immunoreactive luteinizing hormone responses to low doses of gonadotropin-releasing hormone (GnRH): dose–response curves in GnRH-deficient men. J Clin Endocrinol Metab 1986 63: 143–150.
Fabbri A et al . Low bioactive luteinizing hormone in nonorganic male impotence: possible relationship with altered gonadotropin-releasing hormone. J Clin Endocrinol Metab 1988 67: 867–875.
Linet OI, Ogrinc FG. . Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. New Engl J Med 1996 334: 873–877.
Padma-Nathan H et al . The Medical Urethral System for Erection (MUSE) Study Group Treatment of men with erectile dysfunction with transurethral alprostadil. New Engl J Med 1997 336: 1–7.
Anonymous. . Yohimbine for male sexual dysfunction. Med Lett Drug Ther 1994 36: 115–116.
Kaplan HS. . The New Sex Therapy Brunner/Mazel: New York 1974
Levine FJ, Goldstein I. . Vascular reconstructive surgery in the management of erectile dysfunction. Int J Impot Res 1990 2: 59–78.
Glibert P et al . Venous surgery in erectile dysfunction. Urol Int 1992 49: 40–47.
Petrou SP, Barret DM. . The use of penile prostheses in erectile dysfunction. Sem Urol 1990 8: 138–152.
Meinhardt W et al . The negative pressure device for erectile disorders: when does it fail? J Urol 1993 149: 1285–1287.
Segre GV, Brown EN. . Measurement of hormones. In: Williams Textbook of Endocrinology, IX edition. Saunders Co: Philadelphia 1998 43–54.
Veldhuis JD, Johnson ML, Dufau ML. . Preferential release of bioactive luteinizing hormone in response to endogenous and low dose exogenous gonadotropin-releasing hormone pulses in man. J Clin Endocrinol Metab 1987 64: 1275–1282.
Sherwood N. . The GnRH family of peptides. Trends in Neurosci 1987 10: 129–132.
Goldstein JA. . Erectile function and naltrexone. Ann Intern Med 1986 105: 799.
Brannemann W et al . Treatment of idiopathic erectile dysfunction in men with the opiate antagonist naltrexone—a double-blind study. J Androl 1993 14: 407–410.
Veldhuis JD, Rogol AD, Samojlik E, Ertel NH. . Role of endogenous opiates in the expression of negative feedback actions of androgen and estrogen on pulsatile properties of luteinizing hormone secretion in man. J Clin Invest 1984 74: 47–55.
Lightman SL et al . Constancy of opioid control of luteinizing hormone in different pathophysiological states. J Clin Endocrinol Metab 1981 52: 1260–1263.
Plourde PV, Dufau ML, Plourde N, Santen RJ. . Impotence associated with low biological to immunological ratio of luteinizing hormone in a man with a pituitary stone. J Clin Endocrinol Metab 1985 60: 797–802.
Warner BA, Dufau ML, Santen RJ. . Effects of aging and illness on the pituitary–testicular axis in men: qualitative as well as quantitative changes in luteinizing hormone. J Clin Endocrinol Metab 1985 60: 263–268.
Carani C et al . Changes in the bioactivity to immunoreactivity ratio of circulating luteinizing hormone in impotent men treated with testosterone undecanoate. Acta Endocrinol 1989 120: 284–288.
Acknowledgements
The authors wish to thank Drs Massimino D'Armiento and Susanna Dolci for the critical reading of the manuscript. Our compliments and gratitude to Paola Minelli for her secretarial work and to Dr Rosaria Caruso for adapting her English expertise to our needs. This paper has been partially supported by the Italian Ministry of University and Scientific Research grants.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carosa, E., Benvenga, S., Trimarchi, F. et al. Sexual inactivity results in reversible reduction of LH bioavailability. Int J Impot Res 14, 93–99 (2002). https://doi.org/10.1038/sj.ijir.3900832
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijir.3900832
