

Key Points
- Esophageal pain manifests as symptoms of heartburn and or chest pain.
- Esophageal pain is a type of visceral pain that is poorly localized owing to divergence of visceral afferents.
- The esophagus is innervated by vagal afferents and visceral spinal afferents, which transmit noxious stimuli to specific centers within the central nervous system.
- Mechanical distention, acid exposure, temperature, and osmolality-related stimuli can all induce esophageal pain.
- Esophageal dysmotility may also induce symptoms of heartburn and chest pain.
- Acid-induced esophageal pain is likely to be mediated by vanilloid receptor 1 (VR1) and by anion-sensing ion channels (ASICs).
- Visceral hypersensitivity has been implicated in the pathogenesis of esophageal pain.
- Psychiatric disease plays a role in heartburn and chest pain.
- Diagnostic evaluation and medical management are important in heartburn and chest pain.
- New therapies are being developed for esophageal pain.
Heartburn
Historical Background
The first description of heartburn dates back to Galen in 200 A.D., who coined the term based upon the observation that diseases of the esophagus often mimicked diseases of the heart.1 Over 1800 years later, Asher Winklestein provided the first clinical definition of acid reflux. At the 85th session of the American Medical Association, he presented five cases of "peptic esophagitis, i.e., an esophagitis resulting from the irritant action on the mucosa of hydrochloric acid and pepsin." In 1958, Baker and Bernstein implicated acid as the inciting agent when they instilled 0.1 N HCl into the esophagus, reproducing patients symptoms of chest pain and heartburn.1 Medical remedies have evolved over the centuries from the use of coral powder in the 16th century, to histamine receptor-2 blockers (H2 blockers) in the 1970s and to proton pump inhibitors (PPI) in the 1990s. Despite these advances, several aspects of heartburn remain elusive. New insights into the concepts of distention-induced heartburn, visceral hypersensitivity, and sustained esophageal muscle contraction suggest that several other noxious stimuli, besides acid, may cause heartburn.
Definition
Esophageal pain is a noxious sensation emanating from the esophagus. Common manifestations of esophageal pain include heartburn and chest pain. Stedman's Medical Dictionary defines heartburn as a "burning sensation, usually centered in the middle of chest, near the sternum and caused by the reflux of acid stomach fluid that enters the lower end of the esophagus, i.e., acid reflux."2 Consequently, the symptom of heartburn has been historically associated with esophageal acid exposure. Chest pain is a symptom that is often described as tightness or a squeeze-like pain centered in the mid-sternal region. When a cardiac cause has been ruled out, this symptom is termed as noncardiac chest pain (NCCP), which has been traditionally associated with esophageal dysmotility disorders (e.g., diffuse esophageal spasm, nutcracker esophagus).
However, the presence of heartburn or chest pain is not 100% predictive of acid- or motility-related disorders, respectively. In fact, clinical data suggest that only 5% to 10% of episodes of acid reflux produce heartburn.3 Recent observations suggest that heartburn and chest pain can be caused by distention of the esophagus and possibly several other noxious stimuli. Similarly chest pain in some patients is related to acid in the esophagus.
Epidemiology of Heartburn
Population-based studies on the prevalence of heartburn are often influenced by the definitions used to describe the disease entity. Using symptom-based descriptions, in a study of Olmstead County, Minnesota, Locke et al.4 described a 19.8% prevalence of heartburn or regurgitation over a 1-year period. In a more racially diverse cross-sectional study of employees at a Veterans' Administration Hospital, El Serag et al.5 found a 27% prevalence of weekly heartburn among African-Americans and 23% among Caucasians. In one of the rare longitudinal studies of gastroesophageal reflux disease (GERD) with the cardinal symptom of heartburn, Kotzan et al.6 described an incidence of 5.4 per 1000 person. The prevalence of GERD in which the cardinal symptom is heartburn appears to increase with advancing age; 20% of patients older than age 65 years complain of heartburn symptoms once a week and 59% at least once a month.4
Nonerosive Reflux Disease (NERD)
Nearly 70% of patients with heartburn do not have evidence of erosive changes on endoscopy and thus are classified as having NERD.7 Furthermore, only 37% to 57% of these patients report symptom relief with PPI therapy.8, 9 Martinez et al.10 reported that patients with NERD were significantly less likely to have abnormal findings on 24-hour pH testing as compared to patients with erosive esophagitis and Barrett's esophagus (Figure 1). Among the NERD population, those patients with a positive pH test were more likely than those with a negative pH test to demonstrate a greater than 75% correlation of acid reflux events with symptoms.9, 10
Figure 1: Distribution of acid reflux times in patients with nonerosive esophageal reflux disease (NERD), erosive esophagitis (EE), and Barrett's esophagus (BE).

*p =.0012. (Source: Martinez et al.,10 with permission from Blackwell Publishing.)
These findings have spurred an effort to further categorize NERD (Figure 2). Clouse et al.11 have delineated a separate entity known as functional heartburn. The Rome II definition of functional heartburn is "an episodic burning in the absence of pathologic gastroesophageal reflux, motility disorders and any structural explanations."11 It is likely that acid exposure is not the major cause of symptoms in patients with functional heartburn.
Figure 2: Proposed algorithm for defining gastroesophageal reflux disease based on endoscopic findings and the results of pH studies.

(Source: Chey,12 with permission from Excerpta Medica, Inc.)
Noncardiac Chest Pain
Historical Background
The entity of noncardiac chest pain (NCCP) was first described during the American Civil War when a Philadelphia physician, Jacob Mendez Da Costa, first encountered soldiers who complained of chest pain, shortness of breath, and palpitations. Given the patients' young age, cardiac disease was not thought to be the underlying etiology of symptoms and the syndrome was described as the "irritable heart."13 In 1892, Sir William Osler14 coined the term "oesophagismus" in reference to esophageal spasm that was associated with emotional disturbances and substernal chest pain. In 1911, Hertz15 was the first to reproduce symptoms of chest pain with balloon distention of the esophagus. With the advent of esophageal manometry in the 1950s, motility disorders were found to be associated with NCCP. In the 1970s, nutcracker esophagus was thought to be the most common motility disorder found in patients with NCCP.16
Definitions
Noncardiac chest pain is defined as "angina like" chest pain that is not due to ischemic heart disease or other cardiac pathology.17 One can only assume the esophagus to be the source of pain after excluding etiologies related to musculoskeletal structures and other viscera in the chest. Patients with esophageal pain experience symptoms that are nearly indistinguishable from cardiac pain. Patients with esophageal pain may exhibit diaphoresis, pallor, and dizziness that is frequently seen in cardiac angina.18 Noncardiac chest pain, like cardiac chest pain, at times can be related to exertion and can often be relieved with nitrates and calcium channel blockers.19 Characteristics that may differentiate esophageal pain from cardiac angina include the provocation of pain with meals and certain postures, relief with antacids, periods of prolonged remission, nocturnal symptoms, delayed relief from nitroglycerine (10 minutes or longer), and the association with specific esophageal symptoms.20 In particular, symptoms of heartburn, regurgitation, and dysphagia are found in nearly 83% of NCCP patients referred for esophageal manometry/24-hour pH monitoring.21
The situation of NCCP is complicated by the fact that both esophageal and coronary artery disease may be present in the same patient and at the same time. Furthermore, there are no perfect tests to exclude pain originating from either the heart or the esophagus. Symptoms of chest pain may be present in patients with esophageal motility disorders and GERD. However, the majority of patients may not have any identifiable abnormality. Rome II delineated a functional variant of NCCP in the form of functional chest pain of presumed esophageal origin, described as "at least 12 weeks of midline chest pain or discomfort that is not of burning quality, occurring in the absence of pathologic gastrointestinal reflux, achalasia of the esophagus or other motility disorder with a recognized pathologic basis."11
Epidemiology
Nearly 30% of coronary angiograms performed to evaluate chest pain result in normal or insignificant findings.18 Fifty percent of patients with chest pain in whom a cardiac cause has been eliminated are ultimately found to have esophageal abnormalities as the cause of their symptoms.22 Noncardiac chest pain has been estimated to constitute 2% to 5% of all emergency room visits.23 Population studies estimate the prevalence of NCCP as ranging between 19.5% and 33%.4, 24, 25 Unlike heartburn, the overall prevalence of NCCP appears to decrease with advancing age.25
Mechanisms of Heartburn and Esophageal Pain
Heartburn and chest pain are manifestations of visceral pain. Visceral pain by definition means that it originates from the organs of the thorax, abdomen, and pelvis. Visceral pain is distinguished from somatic pain in that it is often diffuse and poorly localized.27 Visceral pain is typically accompanied by motor and autonomic reflexes such as nausea and vomiting, but somatic pain is not. Visceral pain may occur in the absence of actual injury or trauma. In addition, visceral pain is often referred to areas other than the location of viscera from which it originates; for example, biliary pain may be referred to the right shoulder and renal colic to the groin area. Visceral pain tends to be poorly localized because unlike somatic afferents, visceral afferents exhibit extensive divergence within the central nervous system (Figure 3).27 Visceral afferents often travel with somatic afferents from the body wall, which explains why esophageal pain may be referred to the chest wall. The phenomenon of referred visceral pain is the basis for secondary allodynia or hyperalgesia.
Figure 3: Schematic of visceral pain. Visceral pain is mediated by visceral afferents that are processed in the dorsal root ganglion.

(Source: Cervero and Laird,27 with permission from Elsevier Science.)
Sensory Innervation of the Esophagus
The esophagus receives innervation from vagal and spinal nerves. Even though the majority of the esophageal pain pathways are probably located in the spinal nerve, some actually may be in the vagus nerve.
Vagal Afferents
Vagal afferent nerve endings are found in both the mucosa and the muscular layer of the esophagus.28 They are also present in the intraganglionic laminar nerve endings (IGLEs), which appear as specialized leafy structures covering the myenteric ganglia in the tunica muscularis layer of the esophagus.29 Intraganglionic laminar nerve endings have been postulated to sense mechanical shearing forces between muscle layers.30 They also have been demonstrated in the animal model to serve as transduction sites for mechanosensitive vagal afferent neurons.31
Seventy percent to 90% of the nerve fibers in the vagus nerve are unmyelinated fibers, and the majority of these are afferents.32 The ratio of afferent to efferent fibers in the vagus is approximately 9:1.32, 33 Vagal neurons that receive afferents nerve endings from the esophagus have cell bodies in the nodose ganglia. The latter are located below the jugular foramina.34 Vagal afferents project to the brainstem in the medial division of the nucleus solitary tract.35 From there, second-order neurons extend to the hypothalamus, ventrolateral medulla, and parabrachial nuclei. There are also projections that extend from the brainstem to the anterior cingulate gyrus, insular cortex, and lateral primary somatosensory cortex.34, 36
Spinal Visceral Afferents
Spinal visceral afferents are found in the mucosal and submucosal layers as free nerve endings without any specialized structure at their terminals. The majority of these afferents are unmyelinated C fibers with cell bodies in the dorsal root ganglia.28 Paired dorsal root ganglia located in the cardiac and splanchnic nerves provide craniocaudal innervation to the esophagus with the primary areas of innervation in the C2–C6, T2–T4, and T8–T12 regions.37, 38, 39 Afferent fibers then ascend centrally via spinothalamic tracts and dorsal columns, projecting to the thalamus and to the primary somatosensory cortex, insula, and anterior cingulate gyrus.28
Central Nervous System Processing of Esophageal Afferents
Cortical evoked potentials (CEPs), functional MRI (fMRI), positron electron tomography (PET), and most recently magnetoencephalography (MEG) have shed new light on the cortical processing of esophageal sensory signals. Aziz et al.,40 using PET scanning and fMRI, demonstrated that nonpainful esophageal sensation resulted in an increased regional blood flow bilaterally in the central sulcus of the primary somatosensory cortex, insular cortex, and frontal/parietal operculum. Painful sensations elicited by balloon distention produced increased activity in the same areas but of greater magnitude than nonpainful stimuli. In addition, the anterior cingulate gyrus and the superior frontal gyrus appear to be activated in response to noxious stimuli.40
The timing of cortical activity in relation to the noxious stimulus delivered to the esophagus has been further elucidated by studies utilizing MEP and CEP. Hobson et al.41 found that electrical stimulation of the esophagus resulted in cortical activity that occurred in parallel within the primary (S1) and secondary (S2) somatosensory cortex and posterior region of the insular cortex (Figure 4). This activity was directly related to the intensity of the esophageal stimuli. Neural activity appeared to occur later in the anterior insular and cingulate areas in a manner that was not stimulus-dependent.
Figure 4: Latency of cortical responses to painful esophageal stimuli based on neuroanatomy and gender.

This demonstrates early activation in the somatosensory cortex (S1, S2) and posterior insula and delayed activation in the anterior insula and cingulate. *p =.0001. There was a significant decrease in P1 latency from the mid-cingulate when compared to the two other cingulate regions when male and female data were pooled. #p =.04. (Source: Hobson et al.,41 with permission from American Gastroenterological Association.)
This dichotomy in cortical activity suggests a two-step mechanism in the central nervous system (CNS) processing of noxious esophageal stimuli: (1) early cortical activity centered in the primary somatosensory cortex and the posterior insular cortex, which is responsible for the expression of visceral pain; and (2) late activity in the anterior insular and anterior cingulate gyrus, which is primarily earmarked for the affective response to esophageal pain.41
Stimuli that Cause Heartburn and Esophageal Pain
Both experimental animal models and clinical research in humans have demonstrated that a number of noxious stimuli may cause heartburn and esophageal pain. Exposure to acid, mechanical distention, esophageal muscle spasm, high osmolality contents, and extreme temperatures are some of the noxious stimuli that may illicit heartburn as well as chest pain.
Distention as the Stimulus for Heartburn and Esophageal Pain
Distention of the esophagus results in secondary peristalsis at lower levels of distention and pain at higher levels of distention.42, 43 These responses are mediated by mechanosensitive fibers in the vagal and spinal nerves.28 Studies in the opossum esophagus demonstrate two types of low-threshold vagal afferent fibers. The first type of fibers exhibit short-duration activity in response to swallows, which relates to contractions of the circular muscle layer.44 The second type of mechanosensitive fibers show a long duration of response during swallows, which correlate with longitudinal muscle contractions. Vagal afferent fibers exhibit a steep increase in the activity within a narrow range of distending pressure, which implies that these afferents are responsible for the physiologic reflexes involved in the secretomotor function of the esophagus.45
In contrast to vagal afferents, the spinal afferents contain both low threshold (<5 mmHg, 63%) and high-threshold (>40 mmHg, 37%) mechanosensitive fibers.46 Both types of mechanonociceptors appear to be present in series within the longitudinal muscle layer.45 Unlike vagal afferents, the spinal afferents have a linear increase in response to increasing levels of distention.45 It is likely that the pain associated with esophageal distention is mediated by the spinal afferents through the recruitment of high-threshold mechanonociceptors.46
Distention of the esophagus is generally thought to cause esophageal pain, but several studies show that the majority of subjects actually experience heartburn with esophageal distention. Distention causes two fundamental changes in the esophageal wall. First, it increases wall tension and wall stress. According to Laplace's law, Tension = Pressure  Radius, and Wall Stress = Pressure Radius/Wall Thickness. Second, distention increases the cross-sectional area (CSA) of the esophagus, which implies circumferential wall stretch.47 Considerable attention has been paid to the possible roles of tension/wall stress, and wall stretch in the mediation of distention-induced sensation. Using impedance planimetry, Barlow et al.47 found that hyoscine-N-butyl bromide (HBB), a cholinergic muscarinic blocker, which decreased wall tension, did not influence distention-induced esophageal sensation. Takeda et al.,48 who used ultrasound imaging of the esophagus to determine biomechanical properties of the esophageal wall during esophageal distention, reported similar findings. They concluded that stretch receptors were important in the mediation of distention-induced esophageal sensation.
Radius, and Wall Stress = Pressure Radius/Wall Thickness. Second, distention increases the cross-sectional area (CSA) of the esophagus, which implies circumferential wall stretch.47 Considerable attention has been paid to the possible roles of tension/wall stress, and wall stretch in the mediation of distention-induced sensation. Using impedance planimetry, Barlow et al.47 found that hyoscine-N-butyl bromide (HBB), a cholinergic muscarinic blocker, which decreased wall tension, did not influence distention-induced esophageal sensation. Takeda et al.,48 who used ultrasound imaging of the esophagus to determine biomechanical properties of the esophageal wall during esophageal distention, reported similar findings. They concluded that stretch receptors were important in the mediation of distention-induced esophageal sensation.
Wall stretch during esophageal distention is dependent on the compliance characteristics of the esophagus, which is not uniform in all regions of the esophagus. Patel and Rao49 found that the lower esophageal sphincter (LES) and proximal esophagus exhibit greater wall tension, lower CSA, and lower compliance as compared to the middle or distal esophagus. In their studies, balloon distentions in the proximal esophagus produced pain at lower thresholds than in the distal esophagus, which indicates that stretch alone cannot explain the entire distention-induced sensation.
Distention of the esophagus by food and gastroesophageal reflux (GER) is a possible cause of heartburn and NCCP. Distention-induced belching has also been postulated as a factor in causing symptoms of chest pain. Gignoux et al.50 conducted graded balloon distentions in NCCP patients. They graded these patients as high- and low-threshold belchers based on responses to intraesophageal air injection. High-threshold belchers belched during two of three 40-cc distentions and low threshold belchers did not. These investigators found that the balloon distention test was positive in 64% of high-threshold belchers versus 14% in low-threshold belchers, thereby suggesting that belching may be a cause of increased sensitivity to mechanical distention seen in patients with NCCP.
Muscle Spasm as the Stimulus for Heartburn and Esophageal Pain
Esophageal spasm as the cause of angina-like pain has been discussed for a long time. The observation that patients may get relief of their esophageal pain with smooth muscle relaxants (nitroglycerine) suggests that smooth muscle contraction may indeed elicit pain. Esophageal motility disorders are identified manometrically in 30% of patients with NCCP.21, 51, 52 Pope and colleagues were the first to identify high amplitude contractions in patients with angina like pain.53 In 1979, Castell's team16 described a group of patients with angina-like pain who had peristaltic contractions of greater than 225 mmHg. They coined the term nutcracker esophagus for this entity. However, nutcracker esophagus is only one of the motility disorders found during the diagnostic workup of NCCP. In a review of a large multicenter clinical database of manometry studies, Dekel et al.54 identified hypotensive LES as the most common motility disorder in this group of patients (61%).
Nutcracker esophagus as the cause of esophageal pain has not been borne out by prolonged ambulatory pressure recordings. Several studies, conducted during the 1980s and early 1990s, failed to find a temporal correlation between pain events and abnormal esophageal contractions. All of these prolonged ambulatory motility studies were done using intraluminal pressure monitoring techniques, which record contraction of the circular muscles of the esophagus. Recent studies using high-frequency intraluminal ultrasound (HFIUS) imaging technique, which records longitudinal muscle contraction, reveal that the latter may be important in the genesis of heartburn and esophageal pain. Balaban et al.55 found a sustained increase in esophageal muscle thickness (which represent longitudinal muscle contraction of the esophagus) prior to 18 of the 24 chest pain events (Figures 5 and 6). The mean duration of these contractions was 71 seconds and these contractions preceded pain by at least 30 seconds. Similarly, chest pain induced by edrophonium, which is believed to be esophageal in origin, was associated with a sustained esophageal contraction (SEC).55 Pehlivanov et al.56 conducted a similar study in patients with heartburn and found a close temporal correlation between longitudinal muscle contraction and heartburn symptoms. Interestingly, longitudinal muscle contraction was found in connection with heartburn associated with acid reflux and heartburn not associated with acid reflux with similar frequency (Figure 7). Mean duration of longitudinal muscle contraction associated with heartburn was approximately 35 seconds, significantly less than that associated with chest pain in the Balaban study. Acid (0.1 N HCl) infusion into the esophagus (Bernstein test) also induces esophageal longitudinal muscle contraction, and subjects responding to acid infusion with heartburn revealed a strong longitudinal muscle contraction prior to the onset of heartburn, indicating that the two events may be related. More evidence for the longitudinal muscle contraction in the genesis of heartburn is revealed by the study of Bhalla et al.,57 who performed two acid infusions into the esophagus, one after the other. The second acid infusion elicited heartburn with a shorter latency and stronger intensity than the first acid infusion. Interestingly, longitudinal muscle contraction elicited by the second acid infusion was also stronger than during the first acid infusion, providing further evidence of the temporal relationship between longitudinal muscle contraction and heartburn. Temporal correlation, however, does not prove causality, and further studies are needed to prove the cause-and-effect relationship between chest pain, heartburn, and longitudinal muscle contraction of the esophagus.
Figure 5: Esophageal wall thickness in patients with chest pain and controls.

Peak (black bar) and mean (striped bar) percentage increases in total esophageal muscle thickness during sustained esophageal contractions (SECs) associated with chest pain periods, control periods, and swallows. SEC was defined by the following criteria: (1) initiation by two or more consecutive images (2 seconds apart) with muscle thickening greater than the baseline thickness + 2 standard deviations (SD), and (2) total duration of muscle thickening above baseline greater than the mean + 3 SD duration of a swallow-associated contraction. (Source: Balaban et al.,55 with permission from American Gastroenterological Association.)
Figure 6: Esophageal pH (a), manometric pressure (b), and esophageal wall thickness (c) as measured by high-frequency intraluminal ultrasound.
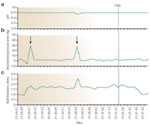
The vertical line (pain) represents the onset of chest pain. Sustained esophageal contraction (SEC) measured as an increase in wall thickness precedes the episode of chest pain and is accompanied by an increase in intraluminal pressure (arrows). (Source: Balaban et al.,55 with permission from American Gastroenterological Association.)
Figure 7: Simultaneous readings of esophageal pH, muscle layer thickness, and manometric pressure in patients with heartburn.

Sustained esophageal contractions (SECs) detected by an increase in esophageal muscle thickness on high-frequency intraluminal ultrasound precede symptoms of heartburn in the absence of pathologic acid reflux detected on pH recording. (Source: Pehlivanov et al.,56 with permission from American Physiological Society.)
Chemical Stimulants: Acid as the Stimulus for Heartburn and Chest Pain
A number of chemical agents may cause esophageal pain, the most accepted of which is acid. Even though the precise mechanism by which acid causes heartburn and pain is not known, the current understanding is as follows: acid and pepsin induce injury to the squamous epithelium and as a result the epithelium becomes porous and leaky. Electron microscopic studies show evidence of dilated intracellular spaces in the squamous epithelium of esophagus that allows diffusion of acid into the mucosa and lamina propria. Acid-sensitive nerve endings, located in the mucosa and lamina propria, carry the sensation of heartburn and chest pain to the CNS. Not much is known about these acid sensitive nerves; however, it appears that two types of receptors, vanilloid and anion-sensing ion channel (ASIC) receptors may be present on the acid-sensitive nerve endings that are important in transducing acid-induced sensation.
Vanilloid Receptors
Vanilloid receptor 1 (VR1) is a polymodal, nonselective calcium-permeable cation channel with six transmembrane domains (Figure 8). The VR1 receptor belongs to a transient receptor potential (TRP) channel family of receptors.58VR1 activation occurs with exposure to heat (>48°C), hydrogen ions,59 and capsaicin. A drop in tissue pH of 5 to 6 leads to VR1 activation.60 Capsaicin, an active ingredient in chili peppers, is a key activator of VR1 and works by lowering the heat threshold required to open the VR1 ion pore.59 Consequently, VR1 activation can occur even at normal temperatures. Once activated, VR1 allows the passage of Ca and Na ions through the ion channel, resulting in depolarization of the nerve fibers and propagation of an action potential. Activation of the afferent nerve terminal may also lead to release of neuropeptides (substance P, calcitonin gene-related peptide, neurokinin A), which can induce local neurogenic inflammation (Figure 9).61
Figure 8: Schematic of vanilloid receptor 1 (VR1).

It consists of six transmembrane domains (blue cylinders) along with a calcium-permeable pore-loop (green). Outer (o) and inner (i) plasma membrane leaflets are present. The hydrophilic amino-terminal segment contains three ankyrin repeat domains (A) followed by an N-terminus (N). One of the transmembrane domains also contains a carboxy terminus (C), which does not have any recognizable motifs. (Source: Caterina et al.,58 with permission from Macmillan Publishers Ltd.)
Figure 9: VR1 activation in nerve endings triggers the release of substance P (SP), calcitonin gene-related-peptide (CGRP), and neurokinin A.

This leads to local vasodilation and edema owing to mast cell histamine release and lymphocyte-mediated hypersensitivity reactions. (Source: Szallasi and Blumberg,58 with permission from American Society for Pharmacology and Experimental Therapeutics.)
Matthews et al.62 demonstrated an increase in VR1 receptors in the lamina propria of patients with erosive esophagitis, implying that VR1 receptor may be upregulated under the most common condition associated with heartburn, that is reflux disease. Evidence also suggests that a number of agents (e.g., ethanol, prostaglandins, and others) may sensitize the VR1 receptor and induce esophageal symptoms.63 Capsaicin ingested in the meal also lowers the time to postprandial heartburn in patients with GERD.64
Acid-Sensing Ion Channels
Acid-sensing ion channels (ASICs) are H+ cation channels that belong to the degenerin-sodium (DEG/ENaC) family of receptors. Thus far, four types of ASIC (1 to 4) receptors have been cloned. Consisting of two large transmembrane domains with a large extracellular protein component, ASIC is expressed in the dorsal root ganglia, nodose ganglia, and nerve ending in the mucosa and submucosa of the esophagus.58, 65, 66 A drop in extracellular pH to 6.9 or less causes the ion channel to open, allowing for the passage of cations and propagation of action potentials (Figure 10),67 which is in sharp contrast to the VR1 receptor that requires a steeper drop in pH (<5 to 6) for activation. All subtypes of ASIC are permeable to Na and Li, but ASIC1 is unique in that it is also permeable to Ca. ASIC receptors activation is blocked by amiloride and its derivatives benzamil and ethyl isopropylamiloride (Figure 11).67
Figure 10: Acid-sensing ion channels (ASIC) function as proton-gated channels.

Left: A rapid change in pH from 7.4 to 6 results in inward currents measured at -70 mV in the xenopus oocyte. Right: A drop in pH results in proton transfer and action potential. The mean inward current (I) is measured over six experiments as compared to the maximum inward current (Imax). A significant change in inward current is seen at a mean pH (pHm) of 6.4. Beyond a pH of 6, there is little change in inward current. (Source: Waldmann et al.,65 with permission from Macmillan Publishers Ltd.)
Figure 11: Anion-sensing ion channel 1 (ASIC1) is inhibited by amiloride and its derivatives.

Inhibition of ASIC1 action potential propagation is a function of the logarithmic concentration of the drug in the oocyte. The inward current is blocked by the administration of amiloride, benzamil, and ethylisopropyl-amiloride. (Source: Waldmann et al.,65 with permission from Macmillan Publishers Ltd.)
Recent research has also focused on the interaction of ASIC and esophageal mechanoreceptors. Animal models suggest that the effect of ASIC on tension receptors depends on the type of ASIC. Page et al.68 demonstrated that a gene knockout of ASIC1 results in an increase in the sensitivity of esophageal tension and mucosal receptors to distention. This would suggest that ASIC1 activation result in an inhibitory effect upon the nociceptive response to distention. The ASIC1 knockout also resulted in delayed gastric emptying, which could potentially contribute to reflux.66 Disruption of ASIC2 resulted in an increase in mucosal sensitivity and a decrease in sensitivity to tension.68 The ASIC3 knockout had no effect on mucosal receptors, but it did decrease sensitivity to tension.68
Other Stimuli that Activate Esophageal Nociceptors
Noxious stimuli including temperatures (hot/cold), bile, and hypertonic solutions have been associated with esophageal pain. In addition, electrical stimulation of the esophagus induces symptoms of heartburn and chest pain.69
Duodenogastroesophageal Reflux
Along with potentially augmenting the noxious effects of trypsin, acid, and pepsin, bile may also produce symptoms of esophageal pain through direct interaction with vagal afferents. Page et al.70 performed experiments in the ferret involving stimulation of mucosal and tension receptors with bile infusion into the esophagus. Their investigation was significant in that 100% of the mucosal receptors and 50% of the tension receptors responded to bile. In addition, a separate nerve fiber class that was insensitive to mechanical stimulation was also recruited by bile.
Thermal Stimulus
Both experimental studies and clinical observation suggest a role for the thermal activation of esophageal nociceptive pathways. Patients often identify coffee, tea, and other hot drinks as potential triggers of heartburn. In addition, prior investigations have demonstrated that temperatures of greater than 48°C activate the VR1 receptor.59 Using a thermal electrode attached to an esophageal probe, Pedersen et al.71 reported inducing esophageal pain at both cold temperatures (14°C) and hot temperatures (48.5°C). After acid administration, the threshold to induce heat-related pain was decreased and the referred pain area increased by 49%. A related experiment in patients with esophagitis demonstrated a similar process of hyperalgesia to heat (but not cold) stimulus.72
Hypertonic Solution
Unlike the small intestine, the stomach does not alter the osmolality of food contents, and as a result the esophagus is exposed to high osmolality when gastric contents reflux into the esophagus.73 Lloyd and Borda74 reported inducing pain through the infusion of a moderately hypertonic solution (630 mOsm/kg) into the esophagus in 82% of patients who had a positive Bernstein test. In addition, patients with Barrett's esophagus exhibit a greater sensitivity to hypertonic solutions and increased symptoms of nausea associated with acid exposure.73 Feldman and Barnett,75 however, did not find an association between symptoms of heartburn and osmolality of consumed food products.
Visceral Sensitivity as the Cause of Heartburn and Chest Pain
It is believed that hypersensitivity of the esophagus (a form of visceral hypersensitivity) may play a role in the genesis of heartburn and chest pain because GERD and motor abnormalities of the esophagus are not detected in association with heartburn and chest pain during a significant number of these events. Esophageal sensitivity implies an abnormal sensory or pain response, upon activation with stimuli that are usually not noxious. These stimuli could be distention, contraction, acid, other chemical agents, and electrical. The condition is also referred to as an "irritable esophagus." Visceral hypersensitivity has also been implicated in functional gastrointestinal (GI) disorders other than that of the esophagus, for example, functional dyspepsia and irritable bowel syndrome (IBS). Visceral hypersensitivity manifests as either allodynia (a painful response to normally nonpainful stimuli) or hyperalgesia (increased pain response to stimuli that are normally painful).
Several studies show that patients with NCCP experience sensation at lower levels of esophageal distention than normal subjects. Rao et al.76 observed that these patients have a poorly compliant and hyperreactive esophagus. Recent observation that patients with nutcracker esophagus and other spastic motor disorders of the esophagus have hypertrophy of muscularis propria may explain low compliance and hyperreactive esophagus in these patients.
The current concept also theorizes that acid induces local inflammation leading to sensitization of esophageal nociceptors. Beedassy et al.77 performed a retrospective analysis of patients with NCCP. In this study, episodes of chest pain correlating with acid reflux were strongly associated with prior episodes of acid reflux occurring in a preceding 25-minute time period. Similarly, a study in Bernstein-positive subjects observed a decreased time interval to the onset of symptoms between the first acid infusion and the second acid infusion.78
Along with examining the relationship between acid–acid chemosensitivity, several studies have focused on the effect of acid on distention-mediated esophageal pain. In 1999, Rodriguez-Stanley et al.79 reported that 52% of heartburn patients with normal esophageal acid contact time (ACT) exhibited sensitivity to intraesophageal balloon distention. Their finding was in sharp contrast to Fass et al.,80 who found no difference in mechanosensitivity between the GERD patients and normal controls.
Acute acid exposure also appears to enhance sensitivity to mechanical distention. Several experiments demonstrate this observation by comparing responses to balloon distention before and after infusion of acid. Drewes et al.81 reported that acid infusion resulted in a hyperreactive esophagus with an increase in the number of contractions with amplitudes of greater than 2.5 kPa with distention. Sensitization with acid resulted in a 50% increase in the evoked pain area, thus providing evidence of secondary allodynia. The degree of sensitization was also directly associated with the volume of acid infused.
Studies using HFIUS also help clarify the picture of the hypersensitive esophagus. Bhalla's group82 recorded esophageal contractile activity in response to two separate acid infusions, one immediately following the other. The latency of symptoms was smaller and intensity stronger during the second acid infusion as compared to the first. In addition, esophageal contraction amplitudes, contraction durations, and longitudinal muscle activity were greater during the second acid infusion as compared to the first acid infusion. Visceral hypersensitivity is postulated to occur through central (spinal cord or brain) or peripheral (within the esophageal wall) processes.
Central Sensitization
Central sensitization implies a process in the dorsal horn neurons or the cortical regions of the brain. The strongest evidence for central sensitization is provided by the studies of Aziz's group.83 In their experiments, infusion of acid into the distal esophagus increases sensitivity to electrical stimulus in the proximal esophagus. Studies using CEPs to assess visceral afferent nerve activity demonstrate decreased N1 and P2 latencies after acid infusion, suggesting that sensitization occurs at the level of the dorsal horn neurons.84 Hobson et al.85 also report decreased pain thresholds to esophageal electrical stimulation after the infusion of acid into the duodenum. The fact that sensitization can occur in locations distant from the sensitizing stimulus (duodenum) suggests a central site of sensitization.
A study by Hollerbach et al.86 also raises the possibility that central sensitization can occur in the cortical regions of the brain. Using CEP, the investigators examined the response to esophageal electrical stimulation in patients with NCCP and normal controls. Their study was significant in that patients with NCCP had lower thresholds to electrical-induced chest pain. In addition, NCCP patients exhibited lower evoked potential (EP) amplitudes (6  1
1  V vs. 13 2 V, p <.05) and shorter latency periods (219 6 ms vs. 191 7 ms, p <.001) as compared to normal subjects. The cardiovagal reflex, as measured by power spectrum analysis of heart rate variability (PS-HRV), appears to be greater in subjects with NCCP.86 The fact that visceral afferent activity as measured by CEPs was low and cortical output, as measured by PS-HRV, was high suggests that the cerebral processing of visceral sensory input may play an important role in modulating esophageal pain responses.
V vs. 13 2 V, p <.05) and shorter latency periods (219 6 ms vs. 191 7 ms, p <.001) as compared to normal subjects. The cardiovagal reflex, as measured by power spectrum analysis of heart rate variability (PS-HRV), appears to be greater in subjects with NCCP.86 The fact that visceral afferent activity as measured by CEPs was low and cortical output, as measured by PS-HRV, was high suggests that the cerebral processing of visceral sensory input may play an important role in modulating esophageal pain responses.
Peripheral Sensitization
The process of nociceptor sensitization may also occur at the level of peripheral nerves. Studies demonstrate a decrease in the threshold of action potential discharge in the myenteric neurons when exposed to a repetitive inflammatory stimulus.87 Bradykinin, tachykinin, neural growth factors, prostaglandins, adenosine triphosphate (ATP), vanilloid compounds, and serine proteases released from injured tissues may mediate sensitization of afferent nerves.88 Increased expression of VR1 receptor activity found in patients with esophagitis is also an example of sensitization at the peripheral level.
A group of afferent silent nociceptors also exist in the esophagus. These nociceptors are inactive under normal conditions. However, in response to repetitive localized stimulation, tissue injury, and inflammation, they become active, leading to increased excitability of the dorsal horn neurons.89 Activation of silent nociceptors is another peripheral sensitization mechanism that could explain allodynia or hyperalgesia of visceral hypersensitivity.
Altered Autonomic Function
Autonomic nerves play a central role in the modulation of visceral noxious stimuli. The esophagus and the heart share common spinal and vagal innervations. The latter give rise to number of esophagocardiac reflexes. One of these is a vagally mediated inhibitory reflex in which esophageal distention results in a decreased heart rate.90
Clinical studies illustrate the presence of an altered esophagocardiac reflex in NCCP. Balloon distention of the esophagus resulted in an attenuated inhibitory esophagocardiac reflex in patients with NCCP.90 In contrast, using PS-HRV as a measure of the vagal outflow of the heart, Tougas et al.91 demonstrated an increase in vagal activity in acid-sensitive patients with NCCP.
The link between esophageal and cardiac innervation and its implications for NCCP is also exemplified by studies that examined the effect of esophageal acid stimulation on coronary blood flow. Chauhan et al.92 demonstrated that acid infusion resulted in reduction of coronary blood flow in patients with syndrome X. Blood flow in patients with cardiac deinnervation owing to heart transplant did not exhibit acid-mediated decrease in coronary blood flow.
Psychiatric Disease and Noncardiac Chest Pain
The prevalence of psychiatric disease in patients with NCCP has been estimated to be as high as 70%.93 In one of the largest cross-sectional studies of NCCP, Hotopf et al.94 assessed the relationship between psychiatric diseases and chest pain using questionnaires in 5362 British patients in their 30s; 17% of these patients complained of chest pain. Of this group, only 0.4% met the diagnostic criteria for probable cardiac angina. Psychiatric disease was a significant risk factor for both generalized chest pain [odds ratio (OR) 3.55, 95% confidence interval (CI) 2.34–5.37] and exertional chest pain (OR 29.08, 95% CI 6.65–127.15).
Other studies have sought to find an association between psychiatric disease and motility disorders. Clouse and Lustman95 found a comorbid psychiatric diagnosis in 84% of patients with abnormal manometry findings. Song et al.96 reported higher anxiety, depression, and somatization scores in symptomatic patients with nutcracker esophagus, hypertensive LES, and hypotensive contractions.
Ho et al.97 attempted to differentiate between functional chest pain and NCCP in trying to assess the psychological factors in symptomatic patients. Among patients with chest pain and normal manometry, endoscopy, and 24-hour pH monitoring (i.e., functional chest pain), there was a higher proportion of panic disorder (15%), obsessive-compulsive disorder (21%), and major depressive episodes (28%) as compared to a control group of patients with gallstone disease. Interestingly, the prevalence of psychiatric disease in patients with NCCP and a clear-cut esophageal cause was not increased. This suggests that psychiatric disease may be more important in functional chest pain than in patients with motility disorders and acid-reflux–induced NCCP.
Qualitative research methods have also raised interesting observations regarding how depression, anxiety and panic disorders contribute to symptoms of NCCP. Fear of specific cardiopulmonary symptoms (chest pain, dyspnea, palpitations) clearly appears to be heightened.98 Patients with NCCP exhibit difficulty coping with stress-related emotions and also receive less emotional support in dealing with stressors.99 Higher rates of parental divorce, difficulties with anger control, and negative attitudes toward the health care system have also been described.100
Psychiatric Disease and Heartburn
Psychotropic agents like tricyclic antidepressants and benzodiazepines can cause alterations in GI motility and decrease salivary production of bicarbonate, both of which can impair esophageal acid clearance.101 In addition, patients with depression and anxiety have higher rates of alcohol consumption and smoking, both risk factors for GERD.104 Avidan et al.101 estimated the association of GERD in patients with known psychiatric disorders. In this study, the presence of any psychiatric diagnosis increased the risk for heartburn (OR 2.71, 95% CI 1.01–7.30) and exercise-induced heartburn (OR 3.34, 95% CI 1.12–9.96)102. A potential confounder, however, was the possibility of increased rates of alcohol and tobacco use in patients with psychiatric disease.103 A separate study by Lieberman's group103 demonstrated a higher rate of psychiatric symptoms in patients with GERD versus normal controls that was accounted for by a subset of patients (30%) who exhibited a higher degree of psychosomatic distress.
Evidence also suggests that the prevalence of psychiatric comorbidities may be different in patients with NERD versus erosive esophagitis (EE). Ang et al.104 conducted a demographic and psychometric profile of patients with EE and NERD in an Asian population. The study was significant in that patients with NERD were more likely to have a psychiatric illness than patients with EE (46.7% vs. 26.4%, p =.002).
Psychiatric disease also may affect responses to antireflux treatment. Surgical data examining symptom response to antireflux surgery indicate higher rates of recurrent chest pain, bloating, and dysphagia in patients with major depression at 1 year.105 Retrospective analysis of patients who fail to respond symptomatically to laparoscopic Nissen fundoplication also identifies preexisting psychiatric disease as a predictive factor.106
Diagnostic Tests for Evaluation of Heartburn and Chest Pain
The Proton Pump Inhibitor Test
Heartburn in the absence of alarm or "red flag" symptoms is generally a benign disease and the PPI test remains an appropriate and widely utilized diagnostic strategy. The PPI test has a variable positive predictive value, ranging from 22% to 81%.107, 108, 109, 110, 111 Meta-analyses of the PPI test in diagnosing GERD by Numans et al.112 reported a sensitivity of 78% (95% CI 0.66–0.86) and a specificity of 54% (95% CI 0.44–0.65). However, the study was seriously hampered in that there were insufficient data to determine if the variations in PPI dosages and durations of therapy affected the sensitivity of the test. A similar strategy can also be applied to patients with symptoms of NCCP. Wang et al.,113 in a meta-analysis, reported that the PPI test had a 80% sensitivity (95% CI 71–87%) and 74% specificity (95% CI 64–83%) for acid-induced NCCP.
pH Monitoring
Ambulatory 24-hour pH testing has now assumed a more defined role in the diagnostic workup of esophageal symptoms. It is helpful to document abnormal esophageal acid exposure in endoscopy-negative patients who are candidates for antireflux surgery. In the post–antireflux surgery patient, ambulatory testing may also be helpful to evaluate recurrent symptoms of heartburn.114 Esophageal pH testing also can be applied to situations in which patients with heartburn fail to respond to PPI therapy. A distinction to be made is whether the lack of response is because of a lack of acid suppression or an incorrect diagnosis. It is important that pH testing in these patients be done while patients are taking maximal PPI therapy.
pH monitoring facilitates correlation between acid reflux and esophageal symptoms. A recent review article summarizes various indices and their pro and cons.115 Briefly, symptom index (SI), symptom sensitivity index (SSI), and symptom-associated probability (SAP) have been used to determine the correlation between acid reflux and symptoms. The SI, originally described by Wiener et al.,116 is defined as the number of times a symptom occurs in association with an acid reflux event (pH <4) divided by the total number of symptoms. In general, most observers consider an SI of greater than 50% to be indicative of positive association.117 The SSI is defined as the ratio of symptoms associated with reflux episodes to the total number of reflux episodes.3 The SAP analysis divides and compares total number of 2-minute intervals during a 24-hour pH recording period into symptom periods with reflux and symptom free periods with reflux.3 The Fisher's exact test is then applied to calculate the probability (p value) that the reflux and symptom episodes are unrelated. The SAP is calculated as (1.0 – p) 100.3
Clinical studies demonstrate a bimodal distribution of SI ranging from high (greater than 75%) to low (less than 25%). Singh et al.118 reported a higher SI for heartburn in patients with abnormal pH studies versus patients with normal pH testing. Overall, they estimated that an SI of greater than 50% had a sensitivity of 93% and a specificity of 71% for acid reflux disease. Wiener et al.116 also demonstrated that SI correctly identified 97.5% of patients with GERD. In contrast, the SI for chest pain has not been proven to be diagnostically accurate in predicting the presence of GERD related chest pain.119 The problem with SI is that it does not take into account the large number of reflux episodes that do not correlate with symptoms.
The SSI reveals that only a fraction of reflux events are associated with esophageal symptoms (5–10%). Symptom-associated probability analysis is a better test to determine the statistical association between acid reflux and heartburn. However, one of the limitations of SAP analysis is that if the percentage of periods with reflux exceeds a limit, it is impossible to reach the 5% significance level. For one pain episode this number is 5%. Steinbach et al.120 used receiver operative characteristic (ROC) curves to determine the sensitivity and specificity of correlation between acid reflux and heartburn in a group of patient referred to tertiary care center for evaluation of heartburn. The area under the curve for the association ranged from 0.6 to 0.7, which suggests a weak correlation between acid reflux and heartburn.
Irrespective of the index used for the symptom association, it is evident that a large number of heartburn symptoms do not correlate with acid reflux and a large number of acid reflux episodes do not induce heartburn. One can safely conclude that the relationship between acid reflux and heartburn is not straightforward and that there must be more than one stimulus responsible for the genesis of heartburn.
Esophageal Manometry
Esophageal manometry is a useful test for the evaluation of motility disorders in patients with heartburn and chest pain. However, its role in determining the etiology of heartburn and NCCP remains unproven. Manometry is usually required to determine the location of the LES for the purposes of determination of location of the pH probe placement.
Treatment of Heartburn and Chest Pain
Management of patients with esophageal symptoms begins with a good history and physical examination. Symptoms suggestive of cardiac disease (e.g., exertional chest pain, dyspnea, palpitations) necessitate appropriate cardiac workup. "Red-flag" or alarm symptoms (e.g., weight loss, dysphagia, GI bleeding, iron-deficiency anemia) should prompt appropriate endoscopic evaluation.121
Lifestyle Modification
In patients with mild symptoms of heartburn or regurgitation, simple lifestyle modifications may be effective in producing symptom relief. Elevating the head of the bed facilitates nocturnal acid clearance and decreases the duration of supine esophageal acid exposure.122 Patients should also be advised to avoid eating at least 3 hours prior to bedtime because evidence suggests that such activities lead to increased reflux events.126 Avoidance of food products known to cause transient lower esophageal sphincter relaxation (TLESR) and smoking cessation should also be advised.
Efficacy of Proton Pump Inhibitor Therapy
The PPIs cause inhibition of the H+, K+–adenosine triphosphatase (ATPase) pump, thereby leading to potent acid suppression. Proton pump inhibitors effectively heal erosive esophagitis at 8 weeks with an efficacy of 80% or greater.124, 125, 126, 127 Treatment with PPIs is more effective than histamine receptor-2 antagonists (HR2As) in inducing mucosal healing and in bringing about symptom relief.128, 129
In general, all of the PPIs appear to have similar efficacy when used in equivalent dosages.130 The one study that indicates a difference in PPI therapies was one in which esomeprazole healed erosive esophagitis and relieved heartburn more quickly than lansoprazole during the 4-week treatment period.131
In patients with NERD, PPIs are less effective in relieving symptoms as compared to patients with erosive esophagitis. Dean et al.132 described a 56% response at 4 weeks in patients with erosive esophagitis versus 37% in patients with NERD. These results should not be surprising, given the fact that heartburn may not be acid induced in these patients.
The linkage between acid reflux and NCCP is also supported by the efficacy of treatment with PPIs in relieving symptoms of chest pain. In a randomized placebo controlled cross-over trial, Pandak et al.133 reported a 71% response rate of chest pain following 14 days of therapy with high-dose omeprazole (40 mg twice a day); 95% of patients with pH-testing indicative of acid reflux responded to therapy, as did 39% who did not have evidence of pathologic acid reflux. Response rates in other randomized controls run between 71% and 83%.134, 135, 136
Antireflux Surgery
Antireflux surgery is aimed at preventing acid reflux through several mechanisms. These include increasing basal LES pressure and decreasing the occurrences of TLESRs. At the present time, the two most commonly performed procedures are Nissen fundoplication and Toupet partial fundoplication. Indications for antireflux surgery include situations in which patients responding to PPI therapy do not wish to remain on long-term medication. Surgery is a reasonable option in patients with atypical GERD symptoms, such as bronchial asthma, who do respond to PPI therapy. Patients with regurgitation who are nonresponsive to acid suppression may also be surgical candidates.137
Smooth Muscle Relaxants
Sublingual nitroglycerine and other longer acting oral nitrates (nitric oxide donors) have been used in the treatment of esophageal pain; however, their efficacy is not confirmed in controlled clinical trials. Sildenafil, a phosphodiesterase-5 inhibitor, the enzyme responsible for degrading nitric oxide, is a potent smooth muscle relaxant. It relaxes the LES and reduces esophageal contraction amplitude in normal subjects and in patients with achalasia of the esophagus.138, 139 There are no studies on the efficacy of sildenafil in achalasia of the esophagus. A double-blind study in patients with spastic motor disorders found that sildenafil decreased contraction amplitude by more than 70% in normal subject and patients, and the effects lasted for more than 8 hours.140 However, improvement in symptoms was noticed in only four of the 11 subjects, and two of these four subjects experienced significant side effects. Similarly, calcium channel blockers can reduce contraction amplitude in normal subjects and patients with high-amplitude contractions, but these agents are not efficacious in relieving symptoms and produced significant side effects in the controlled clinical trials.141, 142 Therefore, it is clear that therapies other than smooth muscle relaxants are required in the treatment of esophageal pain.
Botulinum toxin Therapy
Botulinum toxin, 100 units, injected into the LES of patients with various types of primary motor disorders has been found to be useful in 72% of patients, with a 50% reduction in the symptoms in an uncontrolled study.143 Achalasia patients were not included in this study. The average duration of follow up was 7.3 months, and a repeat injection was successful in some of the patients. Storr et al.,144 in their uncontrolled study of nine patients with diffuse esophagus spasm, also observed significant improvement in symptoms. They injected botulinum toxin along the distal 10 to 15 cm length of the esophagus. Placebo-controlled studies are needed to determine the true efficacy of botulinum toxin in these disorders.
Other Medical Therapies
Trazodone, in the dose of 100 to 150 mg once a day, is the only antianxiety therapy that shows benefit in the controlled clinical trial.145 In the absence of a clear understanding of the mechanism of esophageal pain, blockade of sensory receptors of pain could be used as treatment. Adenosine, one of the candidates in myocardial ischemic pain, may also be involved in the esophageal pain. Theophylline, an adenosine antagonist inhibits adenosine-induced pain in patients with stable angina.146 Theophylline increases the sensory threshold of distention-induced esophageal pain.76 Furthermore, a 3-month uncontrolled study found significant relief of symptoms in the majority of patients with esophageal pain.76 It is possible that in the near future VR1 and ASIC antagonists may find a place in the treatment of esophageal pain and heartburn.
Managing Visceral Hypersensitivity
Insight into the process of central sensitization has galvanized new perspectives on the therapeutic approach to esophageal pain. In a study by Sarkar et al.,147 the role of PPIs in treating NCCP and functional heartburn was examined by comparing thresholds to electrically induced esophageal pain before and after 6 weeks of high-dose PPI therapy. Following PPI therapy, the pain thresholds increased (34.65 13.4 to 40.5 12.5 mA, p =.03), suggesting that esophageal hypersensitivity was at least partially responsive to acid suppression.
Prostaglandin E2 (PGE2) also plays a key role in mediating esophageal hypersensitivity. Prostaglandins are metabolites of arachidonic acid and play key roles in tissue inflammation and smooth muscle activity. Localized inflammation leads to an increase in PGE2 production due to the activity of cyclooxygenase-2 (COX2). The peripheral administration of PGE2 causes a reduction in nociceptor response to mechanical stimuli through the activation of protein kinase A in the nerve ending.148 In addition, central administration of PGE2 also enhances visceral sensitivity through its effects on the dorsal horn neurons.149 Applying this understanding of PGE2, Sarkar et al.150 conducted a randomized, placebo-controlled study using ZD6416 (Astra-Zeneca, Alderly Park, UK), a known antagonist of the PGE2EP-1 receptor in normal controls. After acid infusion in the distal esophagus, a decreased threshold to electrical stimulation was observed in the proximal esophagus. In the ZD6416 group, there was a significant attenuation of this phenomena [area under the curve (AUC) -11.9 2.5 for placebo and 6.4 6.7 for ZD6416 p <.01], thus confirming that PGE2 plays a central role in peripheral and central sensitization, which opens the door for possible new therapies for esophageal hypersensitivity.
Along with PGE2, N-methyl-D-aspartate (NMDA) receptors have also been found to be important actors in the process of central sensitization associated with esophageal hypersensitivity. The NMDA receptors contain a voltage-dependent channel that is blocked by magnesium and is located in the dorsal horn neurons.151, 152 At resting membrane potentials, the channel is blocked and as a result it does not contribute to nociceptive signaling.153 However, with tissue injury or inflammation, glutamate is released from the nociceptor afferents. Glutamate then binds to the NMDA receptor, which removes the magnesium block and thus allows for action potential propagation.154
Willert et al.154 examined the role played by NMDA receptors in mediating the process of central sensitization in esophageal hypersensitivity. Using intravenous ketamine, a known antagonist to the phencyclidine site of NMDA receptor, the investigators performed electrical stimulation experiments before and after acid infusion. After acid infusion, ketamine markedly decreased esophageal sensitivity [AUC, p <.0001, analysis of variance (ANOVA)] (Figure 12). In addition, ketamine that was given prior to acid infusion prevented the development of acid-induced hypersensitivity as well (AUC, p <.0001, ANOVA). The study supported the theory of central sensitization and again suggested yet another new approach to treating esophageal hypersensitivity.
Figure 12: The effect of ketamine on acid-induced pain thresholds in the proximal esophagus and the foot.

a: The effect of intravenous ketamine infusion on esophageal pain thresholds in the proximal esophagus after acid exposure. Ketamine (–) attenuates the reduction in pain threshold caused by acid compared to saline (—). b: Intravenous ketamine has no effect on pain thresholds in the foot. (Source: Willert et al.,154 with permission from American Gastroenterological Association.)
Future Directions
Since the first description of heartburn nearly 1800 years ago, our understanding of the pathophysiology of heartburn and esophageal pain has grown beyond the simple concept of acid-induced mucosal injury. As the intricate neuroanatomy of esophageal innervation has become better defined, it is apparent that the mechanisms of nociceptive signaling are extremely complex. From a pathophysiologic standpoint, how the esophagus responds to various noxious stimuli remains an important research focus. Further elaboration of how VR1 and ASIC receptors translate nociceptive signals will likely prove to be of great importance, and antagonists of these receptors may find a place in the therapeutic armamentarium. The use of NMDA and PGE2 antagonists will need to be further investigated as viable treatment options. In addition, recent studies on the effect of baclofen, a known  -aminobutyric acid (GABA) agonist, in inhibiting TLESRs should prompt randomized control trials in patients with esophageal symptoms.154, 155
-aminobutyric acid (GABA) agonist, in inhibiting TLESRs should prompt randomized control trials in patients with esophageal symptoms.154, 155
Acknowledgments
Dr. Mittal's research is supported by National Institutes of Health (NIH) grant RO1 DK 60733. Dr. Lee's research is supported by NIH grant DK 07202.
