

Key Points
- Hiatal hernia generally denotes upward displacement of the stomach through the diaphragmatic esophageal hiatus into the thoracic cavity.
- There are two main types of hiatal hernias: sliding (type I) and paraesophageal. Types II, III, and IV are variations of paraesophageal hiatal hernia.
- Sliding hiatal hernia contributes significantly to gastroesophageal reflux disease (GERD) in up to 50% of such cases.
- Enlarging sliding hiatal hernias cause progressive disruption of gastroesophageal reflux barrier, and large hernias cause greater gastroesophageal reflux.
- Sliding hiatal hernias contribute to gastroesophageal reflux through several different mechanisms and they also impair esophageal emptying.
- Isolated sliding hiatal hernias do not usually require surgical repair.
- Paraesophageal hiatal hernias may be associated with a number of serious complications and should be surgically repaired.
Introduction
Although hiatus hernia had been occasionally noted as a congenital anomaly or a consequence of abdominal trauma in the preradiographic literature, the prevalence of this condition was not appreciated until the evolution of imaging technology. With the maturation of imaging technology, especially barium contrast radiography, it became reasonably easy to detect hiatus hernia antemortem. In 1926, Akerlund1 reported that hiatal hernia was found in 2.3% of all upper gastrointestinal x-ray studies. With the improvement of radiographic techniques and a more systematic approach to their detection, more hernias were identified, such that by 1955 the reported incidence was 15%.2 When provocative maneuvers were employed to accentuate herniation during fluoroscopy, the frequency increased more dramatically; of 955 patients subject to abdominal compression during an upper gastrointestinal x-ray series, hiatus hernia was diagnosed in 55%.3
Coincident with this evolution in imaging, the clinical understanding of reflux disease also evolved. The term reflux esophagitis was introduced in 1946 by Allison,4 thereby acknowledging that irritant gastric juices were refluxed from the stomach to the esophagus. Since then, there has been considerable controversy regarding the relationship between esophagitis, heartburn, hiatal hernia, and the physiology of the lower esophagus. Recognizing this controversy and the fact that the main significance of hiatus hernia is in its relationship to reflux disease, it is impossible to discuss hiatus hernia without some discussion of reflux disease. Thus, this review first focuses on the relevant anatomy and classification of hiatus hernia and then examines our current understanding of the relationship between these anatomic variables and the pathophysiology of gastroesophageal reflux disease.
Anatomy and Physiology of the Esophagogastric Junction
The hiatal orifice is an elliptically shaped opening through the diaphragm with its long axis in the sagittal plane through which the esophagus and vagus nerves gain access to the abdomen. Although there is some anatomic variability with partial contribution from the left crus, the most common anatomy is for the hiatus to be formed by elements of the right diaphragmatic crus.5 The crura arise from tendinous fibers emerging from the anterior longitudinal ligament over the upper lumbar vertebrae; the left crus is usually attached to two lumbar vertebrae and the right to three. Additionally, accessory tendons may arise from the fascia over the psoas muscles and from the medial arcuate ligaments. The crura pass upward in close contact with the vertebral bodies for most of their course and only incline forward as they arch around the esophagus.5
Once muscle fibers emerge from the tendinous origin of the right crus, they form two overlying ribbon-like bundles separated from each other by connective tissue. The dorsal bundle forms the left limb of the right crus (thoracic aspect) and the ventral bundle becomes the right limb (abdominal aspect) of the right crus. As they approach the hiatus, the muscle bands diverge and cross each other in a scissor-like fashion with the ventral bundle passing upward and to the right and the dorsal bundle passing upward and to the left. The lateral fibers of each hiatal limb insert directly into the central tendon of the diaphragm but the medial fibers, which form the hiatal margins, incline toward the midline and decussate with each other in a trellis-like fashion in front of the esophagus.5 Although there are variations of this pattern, the basic organization of two flattened muscle bundles first diverging like a scissor and then merging anterior to the esophagus is common to all arrangements (Figure 1). Normally there is about a centimeter of muscle separating the anterior rim of the hiatus from the central tendon of the diaphragm.
Figure 1: Anatomy of the diaphragmatic hiatus.
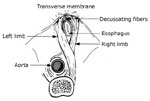
In the most common anatomy, the muscular elements of the crural diaphragm derive from the right diaphragmatic crus. The right crus arises from the anterior longitudinal ligament overlying the lumbar vertebrae. Once muscular elements emerge from the tendon, two flat muscular bands form, which cross each other in scissor-like fashion, form the walls of the hiatus, and decussate with each other anterior to the esophagus. (Source: Modified from Marchand 5 with permission from Society of Thoracic Surgeons.)
Under normal circumstances, the esophagus is anchored to the diaphragm and the stomach cannot be displaced through the hiatus into the mediastinum. The main restraining structure is the phrenoesophageal ligaments, alternatively referred to as the phrenoesophageal membrane, along with an aggregate of posterior elements including the vagus nerve and radicles of the left gastric vein and artery.6, 7 The phrenoesophageal membrane is formed from the fascia transversalis on the undersurface of the diaphragm and, to a lesser degree, fused elements of the endothoracic fascia. This elastic membrane inserts circumferentially into the esophageal musculature, close to the squamocolumnar junction, and extends for about a centimeter above the esophagogastric junction (EGJ), at which point it thins and merges with the perivisceral fascia of the esophagus.8 Thus, the axial position of the squamocolumnar junction is normally within or slightly distal to the diaphragmatic hiatus.9
The anatomic relationship of the distal esophagus, hiatus, and stomach is transiently altered during swallow-initiated peristalsis. Physiologically, peristalsis is a sequenced contraction of both the longitudinal and circular muscularis propria of the esophagus.10 In particular, with contraction of the longitudinal muscle, the esophagus shortens and the phrenoesophageal membrane is stretched; at the termination of the peristaltic sequence, relaxation of the longitudinal muscle along with the elastic recoil of the phrenoesophageal membrane is then responsible for pulling the squamocolumnar junction back to its native position. In effect, this is "physiologic herniation," because the gastric cardia tents through the diaphragmatic hiatus with each swallow (Figure 2).9 This paradox has led to a confusing array of terminology summarized in Figure 3. The globular structure seen radiographically that forms above the diaphragm, beneath the tubular esophagus, during deglutition is termed the phrenic ampulla, bounded from above by the distal esophagus and from below by the crural diaphragm. Emptying of swallowed material from the ampulla occurs between inspirations in conjunction with relengthening of the esophagus.11 As will become apparent in the discussion of sliding hiatus hernia, a type I hiatus hernia is an exaggeration of the normal phrenic ampulla. Not all of the structures illustrated in Figure 3 are always evident radiographically. Commonly, only an A ring is evident (Figure 4) in which case the measurement defining hiatus hernia becomes inexact. In such cases, the demonstration of rugal folds traversing the diaphragm is often used as a defining criterion. Alternatively, a B ring but not an A ring may be evident radiographically, as in Figure 5, in which case the B ring is of such prominence (luminal diameter <13 mm) as to be termed a Schatzki ring. In such case it is easy to apply the  2 cm between the B ring and the hiatus criterion for defining a sliding hiatus hernia.12
2 cm between the B ring and the hiatus criterion for defining a sliding hiatus hernia.12
Figure 2: Demonstration of "physiologic herniation" during swallow using endoscopically placed mucosal clips.
![Figure 2 : Demonstration of |[ldquo]|physiologic herniation|[rdquo]| during swallow using endoscopically placed mucosal clips. Unfortunately we are unable to provide accessible alternative text for this. If you require assistance to access this image, or to obtain a text description, please contact npg@nature.com](/gimo/contents/pt1/thumbs/gimo48-f2.jpg)
a: Before swallow. Clip B marks the position of the squamocolumnar junction 0.4 cm distal to the hiatus and 3.5 cm distal to the anchor point on the vertebral body (V). Clip A is affixed to the esophageal mucosa 3.1 cm proximally. Clip movements are referenced to point V on the vertebral column. b: At the time of maximal esophageal shortening, clip B is 1.8 cm proximal to the hiatus and 2.0 cm distal to point V. The distance between clips A and B is reduced to 2.2 cm, indicative of 29% shortening. c: As elongation proceeds, first both clips descend, after which clip B descends, stretching the A-B segment back to its initial length. d: After swallow, clip B is again at the level of the hiatus. (Source: Kahrilas et al.,9 with permission from American Gastroenterological Association.)
Figure 3: Anatomic features of a sliding hiatus hernia viewed radiographically during swallowing.

The A ring is a muscular ring visible during swallowing that demarcates the superior margin of the LES. The B ring at the squamocolumnar junction is present in only about 15% of individuals and allows for accurate division of the phrenic ampulla into the esophageal vestibule (A ring to B ring) and the sliding hiatus hernia (B ring to the subdiaphragmatic stomach). By convention the distinction between normal and hiatus hernia is a 2-cm separation between the B ring and the hiatus. Rugal folds traversing the hiatus support the conviction that a portion of the stomach is supradiaphragmatic. (Source: Kahrilas,24 with permission from Blackwell Publishing.)
Figure 4: Radiograph of a patient with a small axial hiatal hernia (case 1).
A well-developed A ring is evident, but no B ring. In such cases the criterion for defining hiatus hernia is the appearance of rugal folds traversing the diaphragmatic hiatus. The A ring has no anatomic correlate but physiologically corresponds to the superior aspect of the LES. (Source: Kahrilas and Pandolfino,75 with permission.)
Figure 5: Radiograph of a patient with a small axial hiatal hernia (case 2).
A prominent B ring is evident, but no A ring. The B ring occurs at the squamocolumnar junction and, when subtle, is referred to as the transverse mucosal fold. In instances such as this where there is marked compromise of the esophageal lumen, the B ring is referred to as a Schatzki ring and is a frequent cause of episodic solid food dysphagia. When a B ring is evident, the criterion for defining the hiatus hernia is a separation of 2 cm between the B ring and the diaphragmatic hiatus. (Source: Kahrilas and Pandolfino,75 with permission.)
A key function of the EGJ is to minimize gastroesophageal reflux. This is accomplished by a complex valvular mechanism, the function of which is partly attributable to the esophagus, partly to the stomach, and partly to the crural diaphragm. The esophageal element has been extensively analyzed and consists of the lower esophageal sphincter (LES)—a 2-cm segment of tonically contracted smooth muscle. The proximal margin of the LES extends up to and 1 to 1.5 cm proximal to the squamocolumnar junction.13 The distal margin of the LES is more difficult to define, but careful anatomic studies suggest that it is composed of elements of the gastric musculature—the opposing clasp and sling fibers of the gastric cardia.14 Finally, surrounding the LES at the level of the squamocolumnar junction is the crural diaphragm, composed mainly of the right diaphragmatic crus.15 Alternatively, with variant anatomy, the left crus is dominant, both crura can provide equal contributions, or a band from the left crus crosses to the right (band of Low).8 Elegant physiologic studies have clearly demonstrated that diaphragmatic contraction augments EGJ pressure, in essence serving as an external sphincter.16 Furthermore, if the EGJ is defined as either the end of the LES or the point at which the tubular esophagus joins the saccular stomach, there are normally about 2 cm of tubular esophagus distal to the squamocolumnar junction within the abdomen.9
Types of Hiatal Hernia
In general terms, hiatus hernia refers to herniation of elements of the abdominal cavity through the esophageal hiatus of the diaphragm. The most comprehensive classification scheme recognizes four types of hiatal hernia.
With type I (sliding) hiatal hernia, there is a widening of the hiatal opening and circumferential laxity of the phrenoesophageal membrane, allowing a portion of the proximal stomach to herniate upward. Largely because of the inherent subjectivity in defining type I hiatal hernia, estimates of prevalence vary widely, from 10% to 80% of the adult population in North America.15 In all probability, most type I hiatal hernias, even large ones, are asymptomatic. The main clinical implication of type I hiatal hernias is of the propensity to develop reflux disease, the likelihood of which increases with increasing hernia size. With larger type I hernias, the crural muscles are absent or reduced to a few atrophic strands, and margins of the hiatus abut directly on the transverse membrane of the central tendon of the diaphragm.5 As this dilatation progresses, the hiatus itself is no longer a sagittal slit but becomes a rounded opening, and its transverse diameter approximates the sagittal diameter in size (Figure 6). This change in caliber of the hiatus is most apparent during distention.17 Associated with the widening of the hiatal orifice, the phrenoesophageal membrane becomes thinned and inconspicuous in comparison to its normal prominence. Nonetheless, the phrenoesophageal membrane remains intact and the associated herniated stomach is contained within the posterior mediastinum (Figure 7).15 In marginal instances, type I hiatal hernia is simply an exaggeration of the normal phrenic ampulla, making its identification dependent on measurement technique. However, when a sliding hiatal hernia enlarges further, such that >3 cm of gastric pouch is herniated upward, its presence is obvious, regardless of technique, because gastric folds are evident traversing the diaphragm both during swallow-induced shortening and at rest (Figure 8). The progression from normal anatomy to obvious type I hernia is well illustrated in a recent analysis of the endoscopic appearance of the cardia, viewed in retroflexion (Figure 9).18
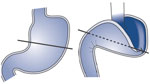
Figure 6: Alteration of the hiatal anatomy associated with sliding hiatal hernia.

Note that the main change is a widening of the hiatal canal. Associated with this, there can be substantial atrophy of the abutting muscular elements, thinning and elongation of the phrenoesophageal membrane, and axial displacement of the gastric cardia. (Source: Modified from Marchand5 with permission from Society of Thoracic Surgeons.)
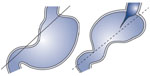
Figure 7: Sliding versus paraesophageal hiatal hernia.

With sliding or axial hiatal hernia there is thinning and elongation of the phrenoesophageal membrane leading to herniation of the stomach into the posterior mediastinum. As such, there is no potential for incarceration or strangulation. With paraesophageal herniation, visceral elements herniate through a focal weakness in the phrenoesophageal membrane with the potential to lead to the usual array of complications associated with visceral herniation through a constricted aperture. (Source: Modified from Skinner.15 with permission from American Gastroenterological Association.)
Figure 8: Type I hiatal hernia. In this example, the herniated gastric cardia is evident at rest, after completion of esophageal emptying.

Note the rugal folds traversing the diaphragmatic hiatus. (Source: Kahrilas and Pandolfino,75 with permission.)
Figure 9: Three-dimensional representation of the progressive anatomic disruption of the EGJ as occurs with development of a type I hiatus hernia.

In the grade I configuration, a ridge of muscular tissue is closely approximated to the shaft of the retroflexed endoscope. With a grade II configuration, the ridge of tissue is slightly less well defined and there has been slight orad displacement of the squamocolumnar junction along with widening of the angle of His. In the grade III appearance, the ridge of tissue at the gastric entryway is barely present and there is often incomplete luminal closure around the endoscope. Grade III deformity is nearly always accompanied by an obvious hiatal hernia. With grade IV deformity, no muscular ridge is present at the gastric entry. The gastroesophageal area stays open all the time, and squamous epithelium of the distal esophagus can be seen from the retroflexed endoscopic view. A hiatus hernia is always present. (Source: Modified from Hill LD, Kraemer SJM, Aye RW, et al. Laparoscopic Hill repair. Contemp Surg 1994;44:1.)
Although there are clear examples in which trauma, congenital malformation, and iatrogeny are implicated, type I hiatus hernia is usually an acquired condition. Allison19 observed that the typical age of onset was in the fifth decade of life. Pregnancy has long been suspected to be an inciting factor.20 Conceptually, Marchand21 argues that the compounded stresses of age-related degeneration, pregnancy, and obesity take their toll on a relative weak point of the anatomy. The positive peritoneopleural pressure gradient acts to extrude the abdominal contents into the chest opposed by the entire surface of the diaphragm. However, of the openings through the diaphragm, only the esophageal hiatus is vulnerable to visceral herniation because it faces directly into the abdominal cavity. Furthermore, because the esophagus does not tightly fill the hiatus, the integrity of this opening depends on its intrinsic structures, especially the phrenoesophageal membrane, which are designed to achieve a fine balance of mobility and stability.21 Add to this vulnerability the repetitive stresses of deep inspiration, the Valsalva maneuver, vomiting, and the physiologic herniation accompanying swallowing, and then compound the stress by packing the abdominal cavity with adipose tissue or a gravid uterus, and eventually the integrity of the hiatus is compromised. Another potential source of stress on the phrenoesophageal membrane is tonic contraction of the esophageal longitudinal muscle induced by gastroesophageal reflux and mucosal acidification.22, 23
The type I, or "sliding," hiatal hernias described above accounts for the great majority of hiatal hernias. The less common types, II, III, and IV, are varieties of paraesophageal hernias. Taken together, these account for 5% to 15% of all hiatal hernias.24, 25, 26 Although individuals with these hernias may also have gastroesophageal reflux, the main clinical significance of paraesophageal hernias lies in their potential for obstructive or ischemic complications. A type II hernia results from a localized defect in the phrenoesophageal membrane while the gastroesophageal junction remains in its native position, fixed to the preaortic fascia and the median arcuate ligament (Figure 7).15 The gastric fundus then serves as the leading point of herniation. The natural history of a type II hernia is progressive enlargement so that the entire stomach eventually herniates, with the pylorus juxtaposed to the gastric cardia, forming an upside-down, intrathoracic stomach (Figure 10). Either as cause or effect, paraesophageal hernias are associated with laxity of structures normally preventing displacement of the stomach—the gastrosplenic and gastrocolic ligaments. As the hernia enlarges, the greater curvature of the stomach rolls up into the thorax. Because the stomach is anchored at the EGJ, the herniated stomach tends to rotate around its longitudinal axis resulting in an organoaxial volvulus (Figure 11).27 Infrequently, rotation may alternatively occur around the transverse axis resulting in a mesenteroaxial volvulus (Figure 12).27
Figure 10: Type II paraesophageal hiatal hernia.
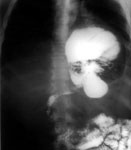
In this example, the entire stomach has herniated into the chest leading to an "upside-down stomach." Because the EGJ remains within the hiatus, there is no element of type I herniation in this example. (See also Figure 23 to understand the resultant gastric configuration.) (Source: Kahrilas and Pandolfino,75 with permission.)
Figure 11: Organoaxial volvulus.
The axis of rotation is the long axis of the stomach. (Source: Modified from Peridikis G, Hinder RA. Paraesophageal hiatal hernia. In: Nyhus LM, Condon RE, eds. Hernia. Philadelphia: JB Lippincott, 1995:544.)
Figure 12: Mesenteroaxial volvulus.
The axis of rotation is along the mesenteric attachment, much the same as is seen with sigmoid colon volvulus. (Source: Modified from Peridikis G, Hinder RA. Paraesophageal hiatal hernia. In: Nyhus LM, Condon RE, eds. Hernia. Philadelphia: JB Lippincott, 1995:544.)
Types III and IV hiatal hernias are variants of the type II (purely paraesophageal) hernia described above. Type III hernias have elements of both types I and II hernias and can evolve from either type. The EGJ is displaced through the hiatus, indicative of a stretched phrenoesophageal membrane, but there is also a focal area of weakening in the phrenoesophageal membrane leading to a portion of the stomach becoming inverted as with a type II hernia (Figure 13). Type IV hiatus hernia is associated with a large defect in the phrenoesophageal membrane, allowing other organs, such as colon, spleen, pancreas, and small intestine to enter the hernia sac (Figure 14).
Figure 13: Type III paraesophageal hiatal hernia.

In this example, much of the stomach has herniated into the chest, but the leading edge of the herniating stomach has additionally herniated through a weakening of the phrenoesophageal membrane, contributing a paraesophageal component to the hernia. Because the EGJ is well above the diaphragmatic hiatus, this is a mixed, or type III, paraesophageal hernia. (Source: Kahrilas and Pandolfino,75 with permission.)
Figure 14: Computed tomography image through the chest showing a type IV paraesophageal hiatal hernia.
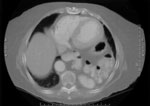
In this example, the sigmoid colon (containing contrast) is clearly evident adjacent to the heart (also contrast enhanced). Lower cuts show the patient to be postsplenectomy, consistent with the observation that paraesophageal herniation occurs most commonly after surgical dissection in the area of the hiatus. (Source: Kahrilas and Pandolfino,75 with permission.)
Although paraesophageal hernias often occur as an idiopathic process, they are also a recognized complication of surgical dissection of the hiatus as is done during antireflux procedures, Heller myotomy, or partial gastrectomy. Many patients with a type II hernia have only vague, intermittent symptoms, or no symptoms at all. When present, symptoms are generally related to ischemia or obstruction. The most common symptoms are epigastric or substernal pain, postprandial fullness, substernal fullness, nausea, and retching. An upright chest x-ray may be diagnostic, revealing a retrocardiac air-fluid level within a paraesophageal hernia or intrathoracic stomach. Barium contrast studies are almost always diagnostic, and attention should focus on the position of the EGJ in order to differentiate type II and III hernias. Upper endoscopy is also useful in the diagnosis and evaluation of patients with paraesophageal hernias. A type II paraesophageal hernia is noted on retroflexion by observing a distinct opening adjacent to the EGJ with gastric folds extending into the opening. With an upside-down stomach it is often not possible to traverse the pylorus, as continued insertion of the endoscope only leads to enlargement of the loop within the gastric body and paradoxical motion away from the pylorus, visible in the distance. Type III paraesophageal hernias can be difficult to identify with certainty endoscopically, often mistaken for large type I hernias. Gastric volvulus and partial prolapse of the intrathoracic stomach through the hiatus are associated with difficulty passing the scope through the EGJ and may lead to triple obstruction at the esophageal, mid-gastric, and duodenal levels.
Most complications of a type II hernia are reflective of the mechanical problem caused by the hernia. Dysphagia may occur as a result of compression of the esophagus within the hiatus by the herniated portion of the stomach or by gastric volvulus. Vomiting is usually intermittent and often associated with continued retching after emesis ends. Postprandial bloating and early satiety are related to compression of the proximal stomach, whereas postcibal pain is usually related to gastric torsion. Bleeding, although infrequent, occurs from gastric ulceration or gastritis within the incarcerated hernia pouch.15 Respiratory complications such as dyspnea and recurrent pneumonia result from compression of the lung by the stomach or other organs herniating through the hiatus. Paraesophageal hernias may present with life-threatening complications, warranting emergent intervention, and should be considered in symptomatic patients with a history of surgical manipulation of the diaphragmatic hiatus. Gastric volvulus may lead to acute gastric obstruction, incarceration, and perforation. The triad of epigastric pain, inability to vomit, and inability to pass a nasogastric tube should prompt immediate evaluation.28
The Association of Type I Hiatus Hernia with Reflux Disease
Endoscopic and radiographic studies suggest that 50% to 94% of patients with gastroesophageal reflux disease (GERD) have a type I hiatal hernia whereas the corresponding prevalence in control subjects ranges from 13% to 59%.12, 27, 29, 30 Most patients with severe esophagitis have a hiatal hernia,31, 32 and 96% of patients with Barrett's esophagus have a sliding hernia greater than 2 cm in length.33 However, the validity of these prevalence estimates is compromised by considering type I hiatus hernia an all-or-none phenomenon. It is more useful to view type I hiatal hernia as a continuum of progressive disruption of the EGJ, as illustrated in Figure 9. Type I hiatus hernia impacts on reflux by affecting the competence of the EGJ both in preventing reflux and in compromising the process of esophageal acid clearance once reflux has occurred.
Pathogenesis of Gastroesophageal Reflux Disease
Although GERD is multifactorial in etiology with potentially important modifying roles played by mucosal defensive factors and differences in reflux constituents, the key abnormalities in the pathogenesis of GERD are reflux of acid and pepsin from the stomach into the esophagus and a reduction in the effectiveness of esophageal acid clearance.
Mechanistic studies of reflux disease have revealed three dominant patterns of EGJ incompetence: (1) transient LES relaxations, (2) hypotensive LES, and (3) anatomic disruption of the EGJ associated with a hiatal hernia. Which reflux mechanism dominates in a given patient depends on a number of factors including the anatomy of the EGJ. Transient LES relaxations account for the overwhelming majority of reflux events in normal individuals and GERD patients without hiatus hernia. Transient LES relaxations appear without fixed temporal relation to an antecedent pharyngeal contraction, are unaccompanied by esophageal peristalsis, and persist for longer periods (>10 seconds) than do swallow-induced LES relaxations.34 The likelihood of reflux occurring during a transient lower esophageal sphincter relaxation (TLESR) is influenced by both the circumstances of the recording and the temporal proximity to a meal, with reflux during as many as 93% or as few as 9%.35, 36
Although TLESRs typically account for up to 90% of reflux events in normal subjects or in GERD patients without hiatus hernia, patients with hiatus hernia have a more heterogeneous mechanistic profile with reflux episodes frequently occurring in the context of low LES pressure, straining, and swallow-associated LES relaxation.37 These observations support the concept that the functional integrity of the EGJ is dependent on both the intrinsic LES and extrinsic sphincteric function of the diaphragmatic hiatus. In essence, gastroesophageal reflux requires "two hits" to the EGJ. Patients with a normal EGJ require inhibition of both the intrinsic LES and extrinsic crural diaphragm for reflux to occur; physiologically this occurs only in the setting of a TLESR. Swallowing does not inhibit the crural diaphragm. In contrast, patients with hiatal hernia may exhibit preexisting compromise of the hiatal sphincter. In that setting reflux can occur with only relaxation of the intrinsic LES, as may occur during periods of LES hypotension or even swallowing.
Once the esophageal mucosa has been acidified by reflux of gastric juice across the EGJ, the normal process of esophageal acid clearance (defined as restoration of esophageal pH to a value of 4) requires both effective esophageal emptying and normal salivation.38 Esophageal emptying is defined as elimination of fluid from the esophagus. Thus, the two major potential causes of prolonged esophageal acid clearance are impaired esophageal emptying and reduced salivation resulting in diminished neutralizing capacity. Diminished salivation during sleep explains why reflux events during sleep or immediately before sleep are associated with markedly prolonged acid clearance times.39 However, in the only large-scale analysis of salivary function in GERD, no difference was found between the resting salivary function of the patients with esophagitis, young controls, or age-matched controls.40
Impaired esophageal emptying in reflux disease was inferred by the observation that patients with abnormal acid clearance times were improved by an upright posture or by head of bed elevation, suggesting that gravity could improve abnormal clearing.41 Two mechanisms of impaired volume clearance have been identified: (1) peristaltic dysfunction, and (2) "rereflux" secondary to hiatal hernia. Significant findings of peristaltic dysfunction include the occurrence of failed peristaltic contractions and hypotensive (<30 mmHg) peristaltic contractions that incompletely empty the esophagus.42 Hiatal hernia and esophageal emptying are discussed in a later section.
Hiatus Hernia and the Diaphragmatic Sphincter
Theories of the mechanism of EGJ competence have seesawed between strictly anatomic explanations, focusing on type I hiatus hernia, and physiologic explanations focusing on the vigor of LES contraction while ignoring the significance of hiatus hernia. Current thinking recognizes contributions from both sphincteric components. However, before discussing recent experiments, it is instructive to reflect on the work of Allison,19 who exhibited masterful understanding of EGJ anatomy. He stated, "The position of the stomach in relationship to the diaphragm is only important in so far as the diaphragm acts as a sphincter.... When the right crus of the diaphragm contracts, its action on the cardia is twofold: first, it compresses the walls of the esophagus from side to side, and second, it pulls down and increases the angulation of the esophagus."
Since the time of Allison's writings, the intrinsic sphincter of the EGJ (the LES) was described and much of his elegant conjecture forgotten. However, recent physiologic investigations have advanced the two-sphincter hypothesis of EGJ competence, suggesting that both the intrinsic LES sphincter and the crural diaphragm encircling the LES serve a sphincteric function.43, 44, 45, 46
Evidence supporting a specialized sphincteric role of the crural diaphragm comes from the observation that the actions of the costal and crural parts of the diaphragm function independently during certain gastrointestinal functions. During esophageal distention, vomiting, and eructation, electrical activity of the crural fibers was reportedly silent at the same time as the dome of the diaphragm was entirely active, suggesting that the crural diaphragm participates in LES relaxation.47, 48 In addition, swallow-induced LES relaxation is associated with minimal crural inhibition, whereas TLESRs are accompanied by significant inhibition of the crural diaphragm.49
Crural diaphragmatic dysfunction may promote gastroesophageal reflux by three mechanisms: (1) disrupting the "pinchcock effect" of crural contraction, (2) altering the morphology and pressure of the LES, and (3) increasing compliance at the EGJ creating wider opening diameters during LES relaxation. The diaphragm augments the LES by a "pinchcock effect" of crural contraction as illustrated in Figure 15. Thus, crural contraction augments the antireflux barrier during transient periods of increased intraabdominal pressure such as occur during inspiration, coughing, or abdominal straining. As evident by the data in Figure 16, the susceptibility to reflux under these circumstances of abrupt increases of intraabdominal pressure depends on both the instantaneous LES pressure and the integrity of the diaphragmatic sphincter.50 Statistical modeling of the data in Figure 16 suggests that the susceptibility to this mode of reflux is proportional to the size of a type I hernia (Figure 17).50 The implication is that patients with hiatal hernia exhibit progressive disruption of the diaphragmatic sphincter proportional to the extent of axial herniation. Therefore, although neither hiatus hernia nor a hypotensive LES alone results in severe EGJ incompetence, the two conditions interact with each other as evidenced by the statistical modeling in Figure 17. This conclusion is consistent with the clinical experience that exercise, tight-fitting garments, and activities involving bending at the waist exacerbate heartburn in GERD patients (most of whom have hiatal hernias), especially after having consumed meals that reduce LES pressure.
![Figure 15 : The |[ldquo]|pinchcock|[rdquo]| action of the pelvic and crural diaphragms on the alimentary canal as it enters and exits the abdominal cavity. Unfortunately we are unable to provide accessible alternative text for this. If you require assistance to access this image, or to obtain a text description, please contact npg@nature.com](/gimo/contents/pt1/thumbs/gimo48-f15.jpg)
Figure 16: Success or failure of individual provocative maneuvers (coughing, leg lifting, abdominal compression, Valsalva) at eliciting gastroesophageal reflux as a function of lower esophageal sphincter (LES) pressure among groups of normal controls, patients without hiatus hernia and patients with radiographically defined hiatus hernia.
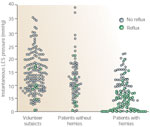
Lower esophageal sphincter pressure values were determined immediately prior to the onset of the maneuver. Open circles indicate individual trials of provocative maneuvers associated with gastroesophageal reflux, whereas solid circles indicate trials in which reflux did not occur. Reflux by the stress mechanism was much more easily elicited among the hiatus hernia patients. (Source: Sloan et al.,50 with permission from American College of Physicians.)
Figure 17: Model of the relationship among lower esophageal sphincter pressure (x axis), size of hernia (y axis), and the susceptibility to gastroesophageal reflux induced by provocative maneuvers that increase abdominal pressure as reflected by the reflux score (z axis).
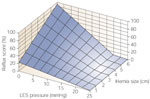
The statistical model was created by stepwise regression analysis of the data in Figure 16. The overall equation for the model is as follows: reflux score = 22.64 + 12.05 (hernia size) – 0.83 (LES pressure) – 0.65 (LES pressure hernia size). The multiple correlation coefficient of this equation for the 50 subject data set was 0.86 (R2 = .75), indicating that 75% of the observed variance in susceptibility to stress reflux among individuals was accounted for by the size of hiatus hernia and the instantaneous value of LES pressure. (Source: Sloan et al.,50 with permission from American College of Physicians.)
Another hypothesis regarding the interrelationship between hiatal hernia and the LES is that type I hiatus hernia in and of itself may diminish LES pressure, an hypothesis consistent with observations made both in both humans and animals. Klein et al.51 studied the thoracoabdominal junction of 10 patients after oncologically motivated resection of the EGJ, removing the entire intrinsic lower esophageal sphincter.51 Subsequent manometric analysis revealed an end-expiratory intraluminal pressure of 6  1 mmHg within the "sphincterless" EGJ, a value similar to the 3 0.2 mmHg observed within the hiatal canal of hernia subjects.52 Relevant animal data come from experimentally severing the phrenoesophageal ligament in dogs, analogous to the effect of axial hiatus hernia in which the ligament is stretched and its diaphragmatic attachments loosened.9, 53 Severing the ligament substantially reduced peak EGJ pressure, which was then restored with reanastomosis.54 In the case of the hiatus hernia patients, reducing the hernia is the equivalent of reanastomosing the phrenoesophageal ligament, and doing so will in effect increase the LES pressure by causing the hiatal canal pressure to be superimposed on the intrinsic LES pressure.13 Perhaps, the only contradictory data are from diaphragmatic electromyography recordings, which strongly support the notion of a phasic, but not tonic, diaphragmatic contribution to EGJ pressure.43, 44, 45, 46 However, relying on electromyography recordings to completely represent the diaphragmatic contribution to EGJ pressure ignores the possible contribution of passive forces such as diaphragmatic and arcuate ligament elasticity to intraluminal pressure. Certainly, in the case of the upper esophageal sphincter, such passive forces contribute an intraluminal pressure of similar magnitude after experimental abolition of the myogenic tone.55
1 mmHg within the "sphincterless" EGJ, a value similar to the 3 0.2 mmHg observed within the hiatal canal of hernia subjects.52 Relevant animal data come from experimentally severing the phrenoesophageal ligament in dogs, analogous to the effect of axial hiatus hernia in which the ligament is stretched and its diaphragmatic attachments loosened.9, 53 Severing the ligament substantially reduced peak EGJ pressure, which was then restored with reanastomosis.54 In the case of the hiatus hernia patients, reducing the hernia is the equivalent of reanastomosing the phrenoesophageal ligament, and doing so will in effect increase the LES pressure by causing the hiatal canal pressure to be superimposed on the intrinsic LES pressure.13 Perhaps, the only contradictory data are from diaphragmatic electromyography recordings, which strongly support the notion of a phasic, but not tonic, diaphragmatic contribution to EGJ pressure.43, 44, 45, 46 However, relying on electromyography recordings to completely represent the diaphragmatic contribution to EGJ pressure ignores the possible contribution of passive forces such as diaphragmatic and arcuate ligament elasticity to intraluminal pressure. Certainly, in the case of the upper esophageal sphincter, such passive forces contribute an intraluminal pressure of similar magnitude after experimental abolition of the myogenic tone.55
Another interesting observation pertains to the effect of hiatus hernia on the morphology of the LES high-pressure zone. Not only does the peak pressure within the LES high-pressure zone negatively correlate with the presence of hiatal hernia, but the overall length of the high-pressure zone can be significantly reduced in patients with large hiatal hernias, principally because of loss of the segment distal to the squamocolumnar junction (Figure 18).9 This distal segment of the LES may be attributable to the sling fibers and clasp fibers of the gastric cardia, also referred to as the intraabdominal segment of the esophagus.14, 56 This is probably the most confusing segment of esophageal anatomy, referred to by Ingelfinger57 as an anatomic and functional "no-man's-land." Highlighting this confusion, Wolf58 remarked that "it is indeed strange that, when normally located below the hiatus, the 'submerged segment' resembles the esophagus while, when displaced above the hiatus, it resembles stomach. In fact, when a large hiatal hernia is present, the original submerged segment is incorporated into the hernia sac." Liebermann-Meffert et al.14 described a "fold transition line," evident in postmortem specimens, which appears analogous to the intragastric margin of the EGJ as imaged endoscopically and related to the angle of His as identified externally.14 The squamocolumnar junction was 10.5 4.4 mm proximal to the fold transition line when measured along the greater curvature. Although the relevance of this distal sphincter segment is controversial, Hill et al.18 found the integrity of this "flap valve" (Figure 9) to correlate with EGJ competence against an antegrade pressure gradient in postmortem experiments.18 With progressive proximal displacement of the squamocolumnar junction above the hiatus, this distal segment eventually becomes disrupted and splays open, creating a radiographically evident saccular structure identifiable as a nonreducing hiatal hernia.53 These observations suggest that the observed shortening of the LES high pressure zone commented on by surgeons as indicative of a mechanically defective sphincter is probably largely a manometric correlate of a large nonreducing hiatal hernia.56, 59
Figure 18: Esophagogastric junction high pressure zone relative to the diaphragmatic hiatus.

Length and position of EGJ high pressure zone relative to the diaphragmatic hiatus among groups of normal subjects (group 1), subjects in whom the squamocolumnar junction (SCJ) was 0 to 2 cm above the diaphragm at rest (group 2), and subjects in whom the SCJ was >2 cm above the diaphragm at rest (group 3). Subject groups were defined by radiographically imaging an endoscopically placed metal mucosal clip. The horizontal bars depict the average limits of the high-pressure zone within each subject group (mean standard error in centimeters). The position of the respiratory inversion point (RIP) is constant among subject groups, whereas the position of the SCJ is progressively more cephalic in groups 2 and 3. Similar to the type IV patients in Figure 9, the group 3 subjects in this investigation had a patulous hiatus and no detectable high-pressure zone at the diaphragmatic hiatus. Thus, the net effect was of shortening the high-pressure zone and positioning the SCJ relatively distally within the high-pressure zone such that it likely would be visible endoscopically from a retroflexed view. (Source: Kahrilas et al.,9 with permission from American Gastroenterological Association.)
A study evaluating the mechanistic profile for reflux in GERD patients with and without hiatus hernia provided some additional insight into the role of EGJ competence in GERD.37 In these ambulatory manometry experiments 90% of reflux events in normal subjects and GERD patients without hiatus hernia were attributable to TLESRs. In contrast, patients with hiatus hernia had a more heterogeneous mechanistic profile with reflux episodes frequently occurring in the context of low LES pressure, straining, and swallow associated LES relaxation. In contemplating this difference in mechanistic profile it is necessary to explore mechanical variables of the system that may account for a relaxed EGJ remaining closed in one case and open in another; one such mechanical variable is sphincter compliance or distensibility.
Acquired anatomic changes attributable to hiatus hernia may alter the compliance at the relaxed EGJ, thereby decreasing the resistance to gastroesophageal flow. Recent physiologic studies exploring the role of compliance in GERD reported that GERD patients with hiatus hernia had increased compliance at the EGJ compared to normal subjects17 or to patients having undergone fundoplication.60 These experiments utilized a combination of barostat-controlled distention, manometry, and fluoroscopy to quantify EGJ compliance. Several parameters of EGJ compliance were shown to be increased in hiatus hernia patients with GERD: (1) the EGJ opened at lower distention pressure; (2) when relaxed, the EGJ opened at distention pressures that were at or near resting intragastric pressure; and (3) for a given distention pressure the EGJ opened about 0.5 cm wider (Figure 19).17 These alterations of EGJ mechanics are likely secondary to a disrupted, distensible crural aperture and likely contribute to the physiologic aberrations associated with hiatus hernia and GERD. Other potential anatomic manifestations of dilatation of the diaphragmatic hiatus include hiatus hernia and disruption of the gastroesophageal flap valve, both of which are strongly associated with reflux disease. Once the hiatus is physiologically disrupted, it is no longer protective in preventing gastroesophageal reflux. In that setting, reflux no longer requires "two hits" because the extrinsic sphincteric mechanism is already disrupted and the only prerequisite for reflux becomes LES relaxation, be that in the setting of swallow-induced relaxation, TLESR, or a period of prolonged LES hypotension.
Figure 19: Esophagogastric junction (EGJ) opening diameter during deglutitive relaxation.

The EGJ cross-sectional area was 0.5 cm wider among the hernia patients and gastroesophageal reflux disease (GERD) patients without hiatus hernia compared to the controls at every distention pressure above 0 mmHg. (Source: Pandolfino et al.,17 with permission from American Gastroenterological Association.)
Increased compliance may also help explain why GERD patients are more likely to sustain acid reflux in association with TLESRs compared to asymptomatic subjects. In an experiment that sought to quantify this difference, normal subjects exhibited acid reflux with 40% to 50% of TLESRs compared to 60% to 70% in patients with GERD.61 This difference may be attributable to increased EGJ compliance and its effect on trans-EGJ flow. This hypothesis is based on an equation modeling flow across the EGJ:
flow =  P
P  R4/C L
R4/C L 
where P is the pressure difference, R is the radius, C is a constant, L is the length of the opening and is viscosity. In the flow equation, flow is directly proportional to EGJ diameter to the 4th power and inversely proportional to the length of the narrowed segment and the viscosity of the gas or liquid traversing the segment. Should TLESRs occur in the context of an EGJ with increased compliance, wider opening diameters will occur under a given set of circumstances, and therefore trans-EGJ flow will increase. Note that patients without obvious hiatus hernia may still have increased compliance secondary to more subtle defects at the EGJ not readily evident using current radiographic or endoscopic methods of evaluation. These defects may be more akin to minor anatomic variants of the EGJ such as a grade II gastroesophageal flap valve illustrated in Figure 9.
In addition to affecting the opening diameter of the EGJ during TLESRs, hiatus hernia may also increase the frequency of TLESRs. A study examining the effects of gastric distention on TLESR frequency in normal subjects and GERD patients with and without hiatus hernia revealed that continuous air infusion was a potent stimulus for TLESRs and acid reflux in all subject groups.62 An interesting finding was that the degree of augmentation of TLESR frequency was directly proportional to axial separation between the squamocolumnar junction and hiatal canal. Thus, increased sensitivity to distention-induced TLESR is yet another mechanism by which altered EGJ anatomy may predispose to GERD.
Compromise of Esophageal Emptying Related to Hiatus Hernia
The defining abnormality with esophagitis is excessive mucosal acid exposure, which, in turn, is dependent on both the frequency of reflux events and the time required to achieve acid clearance for each event. Prolongation of acid clearance among patients with reflux disease has long been recognized, especially with type I hiatus hernia while recumbent.63 A study evaluating the characteristics of esophageal acid exposure in asymptomatic controls and GERD patients with and without esophagitis provided further support of the importance of hiatus hernia in the development of esophagitis.64 This study reported that the esophagitis patients have significantly greater esophageal acid exposure compared to normal controls and nonerosive GERD patients, and that the increased acid exposure was attributable to impaired acid clearance. The variable associated with the greatest impairment of esophageal acid clearance was hiatus hernia. In fact, there was a direct correlation between axial hiatus hernia size and total esophageal acid exposure.
The mechanisms by which hiatus hernia compromises fluid emptying from the distal esophagus have been explored.65, 66 Sloan and Kahrilas66 analyzed the impact of hiatal hernia on esophageal emptying using simultaneous videofluoroscopy and manometry in patients with axial hiatal hernias compared to normal subjects. Subjects were divided into three groups: (1) volunteers with a phrenic ampulla of <2 cm in length, (2) patients or volunteers with maximal ampullary or hiatal hernia length >2 cm that reduced between swallows (reducing hernia group), and (3) patients with hernias that did not reduce between swallows (nonreducing hiatus hernia). Each subject performed 10 barium swallows, and the outcome of each in terms of esophageal emptying was noted. Possible outcomes were complete clearance, minimal clearance because of failed peristalsis, late retrograde flow of barium from the ampulla back up the tubular esophagus (Figure 20), or early retrograde flow from the ampulla occurring coincident with LES relaxation (Figure 21). As shown in Figure 22, the overall efficacy of esophageal emptying was significantly impaired in both hiatus hernia groups, but it was especially poor in the group with nonreducing hernias. The group with nonreducing hernias had complete emptying in only one third of test swallows and exhibited early retrograde flow, a phenomenon unique to this group, in almost half.
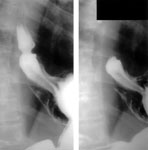
Figure 20: Concurrent manometric and videofluorographic recording of a 10-mL barium swallow in a subject with a reducing hiatal hernia characterized by late retrograde flow.

The tracings from the video images on the right correspond to the four selected times from the swallowing sequence indicated by the numbers at the top of the vertical lines intersecting the manometric record. The schematic diagram to the left indicates the relative spacing of the pressure sensing ports (side holes located proximal to the markers in the fluoroscopic images). The lines at the bottom of the tracing indicate the timing and direction of barium flow. Image 1 depicts the instant of swallowing when barium was visible only in the stomach. Image 2 depicts the instant the stripping wave was at the level of the most proximal sensor; the hiatal hernia had formed and sensors 2, 3, and 4 were in a common cavity within the hernia. Image 3 depicts when retrograde flow began, at which point sensors 2 and 3 were above the hernia, sensor 4 was measuring intrahernial pressure, sensors 5 and 6 were at the level of the diaphragm, and sensor 7 remained within the stomach. Image 4 shows residual barium in the distal esophagus and no hiatal hernia with sensors 3, 4, 5, and 6 now straddling the high pressure zone comprised of the LES and diaphragm. (Source: Sloan and Kahrilas,66 with permission from American Gastroenterological Association.)
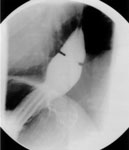
Figure 21: Concurrent manometric and video recording of a 10-mL barium swallow characterized by early retrograde flow in a subject with a nonreducing hiatal hernia.

Tracings from the video images are below the manometric record and correspond to the times on the manometric tracings intersected by the vertical lines. The schematic diagram to the left depicts the relative spacing of the pressure sensors whose tracings are depicted. The arrows next to the video image indicate the direction of barium flow. The first video image to the far left shows a barium filled hiatal hernia at the time the swallow is initiated with sensor 1 in the distal esophagus, sensor 2 in the LES, sensor 3 within the hernia, sensor 4 measuring crural contractile activity, and sensor 5 within the abdominal stomach. The second image was about 1 second after the swallow and depicts the onset of retrograde flow; intrahernial pressure was 2 mmHg and LES pressure was 0 mmHg. Retrograde flow continued for 5 seconds until the peristaltic contraction reached the distal esophagus. The third image depicts antegrade flow with the stripping wave progressing down the esophagus and LES pressure increasing to equal intrahernia pressure ( 4 mmHg). The final image to the far right shows barium cleared from the esophagus with the LES pressure now exceeding intrahernial pressure. (Source: Sloan and Kahrilas,66 with permission from American Gastroenterological Association.)
4 mmHg). The final image to the far right shows barium cleared from the esophagus with the LES pressure now exceeding intrahernial pressure. (Source: Sloan and Kahrilas,66 with permission from American Gastroenterological Association.)
Figure 22: Esophageal emptying results among subject groups based on 10 test swallows.

Control subjects had complete esophageal emptying without retrograde flow in 86% 6% of test swallows compared to 61% 9% in the reducing hernia group and 31% 8% in the nonreducing hernia group (p <.05 vs. controls). The distinction between reducing hernia and nonreducing hernia was the radiographic observation of persistent rugal folds traversing the diaphragmatic hiatus in the nonreducing hernia group. The reducing hernia group exhibited significantly more instances of late retrograde flow (Figure 19) (p <.05 vs. controls) and the nonreducing hernia group had the only individuals to exhibit early retrograde flow (Figure 20) (p <.001 vs. other groups). (Source: Sloan and Kahrilas,66 with permission from American Gastroenterological Association.)
This work corroborated findings by Mittal and coworkers,65 who used concurrent pH recording and scintiscanning to examine the efficacy of fluid emptying and acid clearance in patients with hiatal hernia and compared them to a group of esophagitis patients without hernias. Regardless of the presence of esophagitis, the hernia groups had impaired acid clearance because there was re-reflux from the hernia sac during swallowing (Figure 23). Re-reflux occurs predominantly during inspiration and can be attributed to loss of the normal one-way valve function of the crural diaphragm. By pinching off the distal esophagus, the crural diaphragm prevents backward flow from the stomach during each inspiration when it would be favored by a positive abdominal-thoracic pressure gradient. This one-way valve function of the crural diaphragm is grossly impaired with large type I hernias because a gastric pouch persists above the diaphragm as seen in Sloan's patients with nonreducing hernias.66
Figure 23: Graphic depiction of a radionuclide acid clearance study in a subject with a hiatus hernia.

Fifteen seconds after the injection of a 15-mL bolus of 0.1 N HCl labeled with 200  Ci of technetium-99m (99mTc)-sulfur colloid, subjects swallowed every 30 seconds. The vertical axis represents the region from the sternal notch to the stomach. The horizontal axis is the time scale. The radioactivity is represented by the darker area and no radioactivity is represented by the absence of color. Soon after injection, the radioactivity appears in the stomach. However, note the biphasic response, i.e., an initial reflux of isotope into the esophagus followed by clearance of the isotope during the first three swallows. (Source: Mittal et al.,65 with permission from American Gastroenterological Association.)
Ci of technetium-99m (99mTc)-sulfur colloid, subjects swallowed every 30 seconds. The vertical axis represents the region from the sternal notch to the stomach. The horizontal axis is the time scale. The radioactivity is represented by the darker area and no radioactivity is represented by the absence of color. Soon after injection, the radioactivity appears in the stomach. However, note the biphasic response, i.e., an initial reflux of isotope into the esophagus followed by clearance of the isotope during the first three swallows. (Source: Mittal et al.,65 with permission from American Gastroenterological Association.)
Treatment
Repair of an isolated, asymptomatic type I hiatal hernia is rarely indicated. If symptoms of GERD occur in association with a large hiatus hernia, either medical or surgical treatment is indicated to control the reflux as discussed extensively elsewhere in this volume. Conversely, enlarging types II, III, and IV hernias pose a risk of serious complications similar to complications of viscera herniated through an aperture elsewhere in the body.67 Skinner and Belsey67 reported that six of 21 patients with paraesophageal hernia treated medically died from complications of incarceration, perforation, and bleeding. However, more recent studies suggest that these catastrophic complications are less common than initially reported. Allen et al.68 followed 23 patients for a median of 78 months and found that only four patients had progression of symptoms with only three cases of gastric strangulation in 735 patient-years. In addition, there was only one mortality in that series, resulting from aspiration during an esophagram. Despite these more recent data, most experts still recommend that elective repair should be pursued in patients able to tolerate surgery. These hernias never regress and progressively enlarge. Left untreated, the paraesophageal hernia may eventually reach the stage of the giant intrathoracic stomach, at which point the patient may have substernal pain and pressure, or a gastric ulcer may develop in the poorly draining stomach.69 More problematic, when the fundus becomes distended and prolapses out of the posterior mediastinum, obstruction occurs at the esophageal, mid-gastric, and duodenal levels (Figure 24). If this is not relieved promptly, incarceration may become irreducible. Among a group of 10 such patients with strangulated and incarcerated hiatal hernias, Hill69 reported a 50% mortality. Conversely, among 19 patients in whom preoperative preparation and decompression was possible there was no mortality.69 Thus, once a paraesophageal hernia is identified, current thinking is that it should be treated surgically regardless of symptoms.
Figure 24: Obstruction and entrapment as a complication of type II paraesophageal hernia with an upside-down stomach.

The drawing on the left shows the hernia prior to obstruction with the EGJ still fixed at the hiatus. This drawing is analogous to the radiograph in Figure 10. With distention and filling of the fundus, it has the potential to form an organoaxial volvulus (Figure 11) and reherniate through the hiatus. Obstruction then develops at the duodenum and at the midportion of the stomach. Mortality of this condition is substantial. (Source: Hill,69 with permission from Excerpta Medica, Inc.)
Surgical approaches to type II hiatal hernias can be divided into five components, not all of which are required in every case70: (1) reduction of the herniated stomach into the abdomen, (2) herniotomy (excision of the hernia sac), (3) herniorrhaphy (closure of the hiatal defect), (4) antireflux procedure, and (5) gastropexy (attachment of the stomach subdiaphragmatically to prevent reherniation). The operation can be approached via a transthoracic or transabdominal route. Thoracotomy provides excellent exposure of the esophagus and hernia sac facilitating dissection of sufficient esophageal length and possible creation of a gastroplasty to lengthen the esophagus if needed to ensure a tension-free repair. The transabdominal approach better facilitates reduction of gastric volvulus, and occasionally a thoracotomy will be converted to a thoracolaparotomy for giant hernias with herniation of abdominal contents into the chest.71 Opinion varies as to whether or not an antireflux procedure is necessary if pathologic reflux has not been demonstrated. The most common procedure done is a Nissen fundoplication. Gastropexy is employed if the stomach is unusually mobile after reduction. Although the prognosis following surgical repair of a type II hiatal hernia is excellent, recurrence is more likely than that for type I hernias, presumably because the hiatus is more compromised.15
Laparoscopic repair of paraesophageal hernias is also possible, albeit more challenging than laparoscopic antireflux surgery. Initial experience has reported shorter hospital stays and reduced complications.72 However, mortality is still significant, reported to be as high as 5%.71, 73 Laparoscopic repair is also associated with higher recurrence rates compared to open procedures.28 Thus, the decision of whether to pursue laparoscopic or open repair remains controversial.
Given that paraesophageal hernias are more common with advancing age, many patients who present with paraesophageal hernias have significant comorbidities. In this patient population the risks of surgery may be substantial, and therefore less invasive techniques may be more appropriate. Kercher et al.74 described a technique combining endoscopic reduction of the hernia with percutaneous endoscopic gastrostomy (PEG). This technique was performed in 11 American Society of Anesthesiology class III patients that presented with symptomatic paraesophageal hernia. Laparoscopic assistance was required in nine patients for reduction and gastropexy, with a mean operative time of 61 minutes and hospital stay of 2.8 days. Three major complications (atrial fibrillation, transient ischemic event, and reoperation for an internal hernia) occurred, as did one minor complication (PEG site infection). This technique may represent a valuable alternative management for symptomatic patients with severe comorbidity.
Conclusion
The EGJ is anatomically and physiologically complex, making it vulnerable to dysfunction by several mechanisms. Gastroesophageal reflux disease has several potential causes, the unifying theme being increased esophageal acid exposure. A variety of lines of evidence suggest that hiatal hernia is a significant pathophysiologic factor in approximately 50% of instances. The importance of hiatal hernia is obscured by imprecise usage of the term and the misconception that hiatal hernia is an all-or-none phenomenon. It is more accurate to view hiatal hernia as a continuum of progressive disruption of the EGJ, with larger hernias being of greater significance. The dynamic anatomy of the EGJ outlined herein highlights the difficulty of defining hiatal hernia and elucidating the relationship among hiatal hernia, the diaphragmatic hiatus, the LES, and GERD. Hence, although it is clear that hiatal hernia is a contributing factor in the pathogenesis of GERD, it is equally clear that GERD is a multifactorial process that defies overly reductionist explanation.
Paraesophageal hernia represents a potentially catastrophic condition that warrants immediate attention in all affected patients and urgent intervention in symptomatic individuals. Patients deemed to be good surgical risks should be offered surgical correction before complications occur because emergent surgery in the setting of incarceration has a high mortality. However, the choice of operative approach is controversial. Patients with severe comorbidity may benefit from a less invasive technique that focuses on reduction of the hernia and prevention of gastric volvulus.
