

The process of swallowing (Figure 1) includes the conscious effort to ingest food and the largely subconscious (reflex) efforts of preparing the bolus to be swallowed (preparatory phase), transferring or transporting of the bolus from oral and pharyngeal passages to the esophagus (oropharyngeal transfer or transport phase), and transporting of the bolus through the esophagus to the stomach (esophageal transport phase).
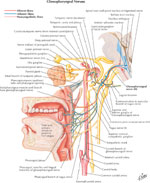
Figure 1: Diagrammatic illustration of motor events of swallowing reflex.

a. Illustrates the onset of the swallowing reflex. It shows tip of tongue in contact with anterior part of palate. Bolus is pushed backward in groove between tongue and palate. Soft palate is being drawn upward. b. Bolus has reached the vallecula. Hyoid bone and larynx move upward and forward. Epiglottis is tipped downward. Contraction wave on posterior pharyngeal wall moves downward. c. Soft palate has been pulled down and approximated to root of tongue by contraction of pharyngopalatine muscles, and by pressure of descending pharyngeal contraction wave. Cricopharyngeus muscle is opening to permit entry of bolus into esophagus. Trickle of food enters also laryngeal opening but is prevented from going farther by closure of ventricular folds. d. The contraction wave has reached vallecula and is pressing out last of bolus from them. The bolus has largely passed through the upper sphincter into esophagus. e. Contraction wave has passed pharynx. Epiglottis is beginning to turn up again as Hyoid bone and larynx descend. Communication with nasopharynx has been re-established. f. All structures of pharynx have returned to resting position. (Source: Netter medical illustrations with permission from Elsevier. All rights reserved.)
Physiology of the Oral Phase of Swallowing
Functional Description
The oral phase includes all swallowing activities that occur within the oral cavity. It can be divided into preparatory and transfer phases. The oral cavity is bounded by the lips anteriorly; the cheeks laterally; the teeth, alveolar ridge, hard palate, and soft palate anteriorly; the teeth, alveolar ridge, floor of mouth, and tongue inferiorly; and the soft palate, uvula, tonsillar pillars, and posterior part of the tongue that form the posterior opening of the oral cavity or the oropharyngeal isthmus.
Ingestion of a bolus usually requires active lowering of the mandible, opening of the lips, and depression of the tongue—actions that increase the size of the oral cavity to accommodate the ingested bolus. During ingestion by sucking, such as with a straw, the lips remain sealed around the delivery vessel and the exit to the back of the oral cavity is closed by the tongue and soft palate. Lowering of the mandible along with depression and retraction of the tongue are accompanied by bracing of the cheeks and mouth floor. These actions generate a subatmospheric pressure within the oral cavity that facilitates flow of fluids into the oral cavity. Such suction may also serve to drive entry of saliva into the oral cavity from the salivary glands.
Mastication is necessary for rendering solid ingested boluses into a size, shape, and consistency that is amenable to transport. This action requires complex variations in the force and velocity of mandibular movement, holding and grinding solids with the teeth. During this process the cheeks and tongue function to position the solid over the grinding surfaces. The tongue also helps reduce softer or dissolvable solids by mashing them against the bony structures bounding the oral cavity and mixing them with liquid elements of the ingested bolus. Secreted saliva also facilitates dissolving and lubricating solid boluses and is the major stimulus for the basal swallow rate between periods of ingestion.
Once the bolus has been adequately prepared it is positioned in a recess on the dorsum of the tongue, primarily by action of the tongue, but with assistance for some boluses by action of the muscles that move the lips, cheek, mouth floor, and mandible. The oropharyngeal isthmus open as the transfer phase begins. Not all of the oral cavity contents are necessarily transported together in a single swallow. The bolus is frequently partitioned, with that part not transported remaining within the oral vestibule or on the floor of the mouth. Indeed, in the process of normal combined eating and drinking, solid and liquid bolus material may even enter the pharynx before onset of the oral transfer phase of the majority of swallows.
At the start of the oral transfer phase the superior perimeter of the tongue is pressed against the hard palate, sealing the bolus from the anterior oral cavity. Especially with large liquid boluses, the posterior aspect of the tongue and soft palate are closed together to prevent premature spill of the bolus into the pharynx. In a rapid sequence, the tongue presses against the hard palate, generating a pressure wave directed posteriorly that propels the bolus into the oropharynx. The force of this tongue action can be volitionally modified. Concurrent with this action, the soft palate elevates, while the cheeks, floor of mouth, and jaw are braced. The oral phase can be considered completed when the bolus tail enters the oropharynx, at which point the posterior dorsum of the tongue remains sealed against the soft palate to prevent retrograde escape of bolus back into the oral cavity.
Role of Muscles and Motor Nerves
Several muscle groups participate in the oral phase of swallowing (Tables 1, 2, 3, 4, 5, 6). All of these are striated muscles using acetylcholine for neurotransmission via nicotinic receptors. The cell bodies of the motor neurons supplying these muscles are located in brainstem nuclei located in the pons (trigeminal, facial) and medulla (nucleus ambiguous, hypoglossal) or in the anterior horn of the cervical spinal cord (C1-2). Figures 2 and 3 are illustrations of lateral and anterior-posterior views of the origins of these cranial nerves. Axons from these motor neurons travel via cranial nerves (CNs) V, VII, IX to XII, and the ansa cervicalis.
Figure 2: Origin of cranial nerves involved in swallowing.

This illustration is a lateral view of the brain stem. Note that cranial nerves V and VII arise in pons and IX, X and XII arise in medulla. In medulla, these nuclei are closely packed and can be affected together in medullary lesions. (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)
Figure 3: Origin of cranial nerves involved in swallowing.

This illustration shows an anterior-posterior projection of cranial nerve nuclei. Left half illustrates sensory nuclei and right half shows motor nuclei. Note that the cranial nerve X is connected with the sensory nucleus (nucleus tractus solitarius, NTS) and motor nucleus to striatal muscles of the pharyngeal and larynx (nucleus ambiguous, NA). Dorsal motor nucleus of the vagus (DMV) contains preganglionic nerves that supply smooth muscle of the esophagus and the rest of the gut. (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)

Muscles in the facial group are supplied by CN VII (Figure 4). During mastication they function to seal the oral cavity and position food over the grinding surfaces of the teeth. The muscles of mastication are supplied by CN V. Their actions move the mandible during chewing, providing the force for grinding food. During the oral transport phase action by muscles in this group to raise the mandible counter the push of the tongue against the hard palate.
Figure 4: Distribution of hypoglossal (XII) nerve.

Note that the XII cranial nerve provides motor innervation to tongue and many of the suprahyoid muscles including the geniohyoid muscle. Along with the cervical accessory (XI) nerve, it also innervates the infrahyoid muscles. (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)
The intrinsic muscles of the tongue are supplied by CN XII. They have no bony attachments. Because muscle tissue is incompressible, the muscles of the tongue function as a hydrostat, wherein changes in shape do not result in a change in volume. For instance, contraction of the transverse muscle of the tongue not only narrows the tongue but also lengthens it. The extrinsic muscles of the tongue have their origin on various bony structures and insert into the tongue. Like the intrinsic tongue musculature, their innervation is via CN XII. Although the palatoglossus muscle can also be considered an extrinsic tongue muscle, its different embryonic origin (4th pharyngeal arch) and innervation (nucleus ambiguous) suggest more appropriate placement in the palatal group. Actions of the extrinsic muscles elevate, depress, protrude, and retract the tongue.
The suprahyoid muscles overall act to raise the hyoid bone and larynx, whereas the infrahyoid muscles have the opposite action. The suprahyoid muscles are supplied by motor neurons located in the trigeminal and facial nuclei in the pons, with the exception being the geniohyoid, which, along with the infrahyoid group, is supplied by motor neurons within the anterior horn of the upper cervical spinal cord. During the oral phase, these two groups act in concert to stabilize the position of the hyoid, whereas those suprahyoid muscles with antagonistic action tense the floor of the mouth when acting together. These actions provide a stable base to resist the forces generated by the tongue contracting against such structures as hard palate and teeth. Thus, these muscles can be active during the both preparatory and transport phases of swallowing.
The palatal muscle group is innervated from motor neurons residing in the trigeminal nucleus or nucleus ambiguous. These muscles act during the oral phase of deglutition to stiffen the soft palate, lower the soft palate to prevent premature bolus spill into the pharynx, or elevate the soft palate to open the oral cavity posteriorly.
Role of Afferent Nerves
Sensory input is critical to the oral phase of swallowing, because assessment of the chemical and physical properties of the bolus at this point allows ready expulsion of boluses with noxious properties. Sensory feedback is also required during bolus preparation and transport to allow appropriate positioning of oral structures; modulate the strength, velocity, and timing of muscle contractions; and determine the position and readiness of the bolus for transport. Some sensory pathways subserve protective reflexes, such as the gag reflex. Finally, stimulation of certain sensory receptive fields acts to initiate, or facilitate the initiation of, deglutition.
Afferent sensory neurons important in the oral phase of swallowing travel in CNs V, VII, IX, and XI (Figure 5). Taste sensation is conveyed by special visceral afferent fibers from the anterior two thirds of the tongue (CN VII), the posterior third of the tongue (IX), and epiglottis (X), with these fibers terminating in the nucleus tractus solitarius (NTS). Taste information is conveyed rostrally from the NTS to the thalamus, insula, and hypothalamus. Sensations of light touch, temperature, pressure, pain, muscle stretch, and proprioception for most of the oral cavity and the anterior two thirds of the tongue are conveyed from fibers that ascend in CN V. These fibers terminate in the mesencephalic (stretch, proprioception), spinal (pain, temperature), and main sensory (touch, pressure) nuclei of CN V. General somatic afferent innervation of the posterior third of the tongue and the faucial pillars ascends through CN IX to the NTS. Some neurons that synapse in the NTS also send axons rostrally to the pons and cortex.
Figure 5: Sensory nerve supply of the mucous membrane of the oral cavity and pharynx.

Sensory receptors that initiate swallow reflex are present only in post part of the oral cavity and upper portion of pharynx. The afferents are carried in glossopharyngeal (IX) and vagus (X) nerves. (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)
The importance of sensory input for the initiation of the oral transport phase of deglutition is self-evident by noting the maximal swallowing frequency that can be obtained while drinking a glass of water at the fastest possible rate compared to the lower sustainable deglutitive rate observed with dry swallows. Because of the large degree of cortical input to the oral phase of swallowing, little information exists regarding the receptive fields and sensory stimuli that facilitate the onset of oral transport. Boluses placed on the posterior tongue (glossopharyngeal innervation) trigger swallowing at a lower volume than on the anterior tongue (trigeminal innervation), with acid boluses having the lowest threshold. Once the transport phase is triggered, sensory information regarding bolus volume and consistency modifies the muscle action.
Central Nervous System Control
Spontaneous, swallowing occurs about once per minute in the awake state, is greatly reduced during sleep, and increases during emotional stress. Damage to different areas of the cortex can result in difficulties with mastication and the initiation of swallowing. These observations underline the importance of cortical and cognitive input to the oral phase of swallowing.
Studies on the central control of the oral phase of swallowing have identified a cortical region, the stimulation of which provokes rhythmic jaw and tongue activity consistent with mastication. At the brainstem level there is evidence for a central pattern generator for repetitive masticatory activity, which appears to involve neurons located in the main trigeminal sensory nucleus and medial pontobulbar reticular formation. In humans, functional imaging studies have identified multiple regions above the brainstem that are active during mastication, including the cortex (sensorimotor, prefrontal, supplementary motor area, insula), thalamus, and cerebellum. Subjects with a chewing side preference show dominant activity in the contralateral sensorimotor cortex during tongue movement. Masticatory activities are inhibited by induction of swallowing.
Multiple cortical areas including the sensorimotor, insular, prefrontal, anterior cingulate, parieto-occipital cortex, along with the amygdala, thalamus, basal ganglia, and cerebellum have been shown to be activated during voluntary swallowing. An important observation in most of these studies is that, although activity is bilaterally represented, there is laterality of activity seen in an inconsistent distribution among subjects. The effect of study constraints (e.g., subject confinement/restraint, bolus delivery) on the areas activated is unknown.
Physiology of the Pharyngeal Phase of Swallowing
Functional Description
The pharyngeal phase descriptively is that period from when the swallowed bolus first enters the pharyngeal cavity until the bolus tail exits the UES. Anatomically, the pharynx can be divided into the nasopharynx (above soft palate), oropharynx (from soft palate to pharyngoepiglottic fold), and hypopharynx (pharyngoepiglottic fold to cricopharyngeus muscle). During the pharyngeal phase, three of the potential exits (upper airway, mouth, and lower airway) must close while the bolus is rapidly propelled into the fourth (esophagus). Closure of these passages results in trapping of approximately 15 mL of air within the pharyngeal space, which is then also transported along with the bolus into the esophagus during isolated single swallows. The time from bolus entrance to bolus exit from the pharynx is slightly less than 1 second (Figure 1). This time is longer for larger boluses, due to earlier entrance into the pharynx from the start of the swallow. The forceful backward thrust of the tongue accelerates the bolus head rapidly. With larger bolus volumes, velocity at the level of the UES may exceed 30 cm/sec, whereas velocities of solid particles may approach 40 cm/sec in the supraglottic region (Figure 2). These are much faster velocities than those that are observed at the tail end of the bolus, which average around 10 cm/sec. Passage of the bolus tail temporally approximates the passage of the peak pressure wave that occludes the pharyngeal lumen at that level. All of these velocities are faster than those of the peristaltic stripping wave in the esophageal body (1 to 4 cm/sec) and likely reflect the need to clear the pharynx quickly so that respiration can resume.
During the pharyngeal phase of swallowing the tongue maintains a position against the palate to seal the oropharynx. The soft palate elevates and the proximal pharyngeal walls move medially to seal off the nasopharynx. The vocal cords and arytenoids are adducted, the adducted arytenoids move to the base of the epiglottis, and the epiglottis swings down to cover the laryngeal vestibule. These actions seal the airway from the pharyngeal cavity. With larger boluses, the bolus head reaches the level of the laryngeal vestibule before the epiglottis has completed its downward descent and is channeled around the larynx into the piriform recesses. In addition the hyoid bone and larynx move superiorly and anteriorly, bringing the larynx to a position under the base of the tongue, and out of the path of the bolus as it descends through the pharynx. The pharynx also widens and shortens, which is accompanied by an elevation of the UES by 2 to 2.5 cm.
The pharyngeal phase can be seen as a continuation of the oral transport phase of deglutition. However, swallows can also be initiated at the pharyngeal level, wherein no bolus is transported from the oral cavity. These reflexive or pharyngeal swallows are in response to pharyngeal stimulation, such as due to accumulated food or saliva. With a sufficient level of stimulation, these reflexive swallows appear to be irrepressible.
Role of Muscles and Motor Nerves
All of the muscles involved in the pharyngeal phase of swallowing are striated muscle and use acetylcholine as their neuromuscular transmitter via nicotinic receptors. The cell bodies of the motor neurons supplying these muscles reside in brainstem nuclei located in the pons (trigeminal) and medulla (nucleus ambiguous, hypoglossal) or in the anterior horn of the cervical spinal cord (C1-2). Axons from these motor neurons travel via cranial nerves V, IX to XII, and the ansa cervicalis (Tables 1-6).
The intrinsic and extrinsic muscles of the tongue continue the action initiated in the oral phase. As the tail of the bolus clears the oral cavity, the dorsum of the tongue remains compressed against the hard and soft palate, thus preventing retrograde bolus escape back into the oral cavity. Action of the palatopharyngeus muscles to approximate the palatopharyngeal folds may help seal the oral cavity. In addition, the back of the tongue is compressed forcefully against the back of the oropharynx, clearing the bolus into the hypopharynx. The tongue remains pressed against the back of the oropharynx usually until the bolus tail exits the hypopharynx. The tongue then moves forward to open the passage to the airway.
The muscles in the palatal group act to tense and elevate the soft palate to seal the entrance from the oropharynx to the hypopharynx. The upper portion of the superior pharyngeal constrictor also contracts to close the pharynx medially as part of the nasopharyngeal seal. The soft palate elevation is maintained until the bolus tail exits the hypopharynx, after which the soft palate usually returns to a rest position.
The muscles of the pharynx can be divided into two functional groups, based on their action. Contraction of the longitudinal group (palatopharyngeus, stylopharyngeus, salpingopharyngeus) elevates and shortens the pharynx. The action of the stylopharyngeus also widens the pharynx and opposes anterior movement of the posterior pharynx. The actions of these muscles elevate the larynx as well. Muscles in the circular group (superior, middle, inferior constrictors) have partial overlap at their borders. Contraction proceeds in an aboral direction to clear the trailing portion of the bolus into the esophagus. All of the pharyngeal muscles have their motor neurons located in the nucleus ambiguous and are innervated via the pharyngeal plexus, except for the stylopharyngeus (CN IX) (Figure 6). Distribution of the vagus (CN X) nerve is show in Figure 7 (Figure 7).
Figure 6: Distribution of the CN IX (glossopharyngeal).
The CN IX provides motor nerve supply to stylopharyngeus muscle and sensory innervation to oropharyngeal mucous membrane through the pharyngeal plexus (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)
Figure 7: Distribution of the vagus nerve (X) to oral and pharyngeal areas.

Lower motor neurons arising from nucleus ambiguus (NA) that are carried in vagus nerve innervate most of the pharyngeal and laryngeal muscles, via its many branches including the pharyngeal plexus. The afferent fibers are distributed over the laryngeal and pharyngeal areas (Source: Netter medical illustration with permission of Elsevier. All rights reserved.)
The function of the muscles in the suprahyoid and infrahyoid groups changes as the swallow progresses from the oral preparatory to the oral and pharyngeal transport phases. Actions of the infrahyoid group are inhibited, so that the suprahyoid group can raise the hyoid bone along with the larynx and move them anteriorly. Considerable variation as to which suprahyoid muscles are activated exists among individuals. The one infrahyoid muscle that remains active is the thyrohyoid, which moves the thyroid cartilage to the base of the hyoid, thus further elevating the larynx.
The intrinsic muscles of the larynx function to close the glottis and supraglottic space, approximating the arytenoids cartilages to the base of the epiglottis. The timing of these events is controversial among studies. Some studies report that activation of intrinsic laryngeal muscles occurs after onset of suprahyoid, superior constrictor contractions, and laryngeal elevation and activity in the submental muscles. On the other hand, visual onset of vocal cord closure occurs before onset of activity in the submental muscles. Vocal cord closure occurs before the closure of the laryngeal vestibule by the downward movement of the epiglottis. Downward movement of the epiglottis to a horizontal position depends on forces transmitted via the ligament between the epiglottis and hyoid as the hyoid moves anteriorly and superiorly. Further downward movement to close the vestibule mostly results from passive compression of the epiglottis by the onrushing bolus and pharyngeal constrictor contraction, although in some individuals the aryepiglottic muscle may facilitate epiglottic movement. Passage of the bolus into the esophagus is followed by opening of the vestibule, mostly from elastic recoil of the epiglottis, and then opening of the glottis by the posterior cricoarytenoid muscle. All of the intrinsic laryngeal muscles involved in deglutition have their motor neurons in the nucleus ambiguous, and the axons pass through the inferior laryngeal branch of the recurrent laryngeal nerve (CN X).
Role of Afferent Nerves
Sensory modalities present in the oral cavity are likewise present in the pharynx and larynx. However, the laryngopharynx has more free nerve endings in the mucosa and more slow adapting mechanoreceptors. The maxillary division of CN V supplies part of the nasopharynx and soft palate. Sensation to the oropharyngeal mucosa is also supplied by CN IX. Three branches of the vagus (CN X) supply the laryngopharynx. The pharyngeal branch supplies the mucosa overlying the levator veli palatini and superior and middle pharyngeal constrictors. The internal branch of the superior laryngeal nerve supplies the hypopharynx, epiglottis, and supraglottic laryngeal structures. The recurrent laryngeal branch supplies the subglottic larynx and inferior constrictor. The neurons for these regions synapse within the NTS.
Activation of receptive fields supplied by CN IX and X can trigger reflexive, or pharyngeal, swallows. Receptive fields supplied by the superior laryngeal nerve have the lowest threshold for initiating a swallow. For most receptive fields the rate of elicitation of swallowing depends on the strength of the pressure stimulus, and dynamic stimuli (e.g., vibration, stroking) are more effective than static stimuli. Within the larynx and pharynx, water is an effective stimulus for swallowing. Those neurons that synapse with the NTS or adjacent reticular formation trigger swallowing.
Sensory feedback modulates muscular function during the pharyngeal phase of swallow. This is manifest by alterations in timing and magnitude of neuromuscular events. Both bolus volume and consistency can modulate activity, depending on the parameter measured.
Central Nervous System Control
The network of neurons that constitute the swallowing pattern generator (SPG) that controls the pattern and sequence of activation of the muscles that carry out the swallowing activity is located in the medulla. The SPG conveniently lies within the NTS, which is the primary sensory relay for the sensory information from the pharynx and also receives cortical input. Neurons of the SPG send projections to the lower motor neurons for the oral and pharyngeal muscles. The activity of the SPG is coordinated with other medullary reflexes. For example, it is difficult to elicit a swallow when the cortical masticatory centers are stimulated. The timing of deglutition in response to pharyngeal water stimulation can be volitionally modified. Also, the incidence and relative timing of activation of various deglutitive muscles varies between individuals and between swallows in the same individual.
Physiology of the Upper Esophageal Sphincter
Functional Anatomy and Neuromuscular Organization
The UES is defined manometrically as a region of elevated intraluminal pressure located at the juncture of the hypopharynx and cervical esophagus. On manometry the length of this high pressure zone is usually 2 to 4 cm. Combined manometric and fluoroscopic studies locate the peak of this high-pressure zone about 1 cm below the level of the vocal cords and adjacent to the C5 and C6 vertebral bodies. This location corresponds to that of the cricopharyngeus muscle. The cricopharyngeus muscle is C-shaped muscle, whose ends attach anteriorly to the cricoid lamina. Contraction of its fibers acts to close the lumen, compressing it against the cricoid cartilage. Studies suggest that the lowermost portion of the inferior pharyngeal constrictor contributes to the upper part of the UES. It is unclear whether the uppermost portion of the cervical esophageal muscle also contributes to the lowermost part of the sphincter.
The cricopharyngeus has a high proportion of slow-twitch, highly oxidative fibers, which support the capability of sustained activity. Other features are a high elastic tissue content and the generation of maximal active tension at nearly twice its resting length. The cricopharyngeus also generates a passive tone in response to stretch. The cricopharyngeus is composed of striated muscle using acetylcholine via nicotinic receptors for its neurotransmission. The motor neurons are in the nucleus ambiguus. There is still controversy about the precise pathways over which efferent axons travel to reach the cricopharyngeus, due to possible species differences and limitations in study technique. Available evidence in humans suggests that the pharyngeal plexus (pharyngeal branch of CN X) and recurrent laryngeal nerve provide a dual ipsilateral innervation to the cricopharyngeus.
Afferent sensory neurons from the UES have their cell bodies in the nodose ganglion and synapse in the NTS. A Golgi tendon organ-like structure near the insertion of the cricopharyngeus on the cricoid cartilage may provide feedback on the state of tension in the muscle. Afferent pathways from adjacent structures also participate in reflexes that modulate UES tone.
Modulation of Basal Tone of the Upper Esophageal Sphincter
When not occupied by antegrade or retrograde bolus transport, the UES remains closed. This closure helps prevent violation of the airway by retrograde passage of esophageal or gastric contents. It also prevents diversion of air into the esophagus during respiration. Unlike smooth muscle sphincters, the UES does not exhibit a constantly active tone at rest. Basal tone depends on the level of activity of the motor neurons, which in turn depends on input from afferent sensory and cortical pathways. Pressure in the UES falls during sleep and anesthesia. During such periods a basal intraluminal pressure can be observed, which likely results from the passive elastic tissue properties of the sphincter or compression from adjacent structures. Basal pressure in the UES varies widely from minute to minute. Pressure in the UES increases during speech, acute emotional stress, and agitation. Movement of a catheter through the sphincter also transiently elevates sphincter pressure. Pressure or water stimulation of the pharynx also increases UES pressure, as does stimulation of the larynx with air puffs.
Upper Esophageal Sphincter Function During Deglutition
During deglutition the UES converts rapidly from a closed state to an open state to allow passage of the swallowed bolus into the esophagus. During this opening the lumen assumes an oval cross section. It then closes as the bolus leaves the pharynx. Because of its attachment to the larynx, which moves upward with deglutition, the UES moves upward 2 to 2.5 cm.
Several factors contribute to opening of the UES. There is a fall in the intraluminal pressure within the UES. In part this is due to an inhibition of the tone of the UES, as observed on electromyography (EMG), that lasts for about 300 to 600 milliseconds (ms). In addition, the action of the geniohyoid, mylohyoid, and thyrohyoid muscles to pull the larynx forward indirectly exerts anterior traction on the UES. Indeed, activation of these muscles can decrease intraluminal pressure within the UES even when the tone is not inhibited. In addition, the pressure applied by the onrushing bolus can push open the lumen of the UES. Thus, it is possible for the UES to relax without opening and open without relaxing. Although much of the action of the UES during deglutition appears stereotyped, its function can be modified by sensory feedback from the swallowed bolus. With larger boluses, the UES pressure relaxes earlier and longer and the UES lumen opens longer and wider. The duration of UES opening during deglutition can also be modified volitionally.
Interactions Between the Oropharynx and Upper Digestive Tract
With deglutition, the oropharynx transfers boluses to the esophagus and thence to the stomach. Material can also travel retrograde from the stomach and esophagus back to the oropharynx. Careful coordination of neuromuscular function during transit in both directions is critical to prevent damage of structures and aspiration of material into the airway.
Pharyngoesophageal and Laryngeal Reflexes
Stimulation of the hypopharynx exerts a powerful inhibitory effect on the esophagus and the LES. Small amounts of fluids in the pharynx can attenuate ongoing peristaltic waves in the esophagus and result in isolated relaxation of the LES when there is no peristalsis. This reflex is mediated by long vagovagal pathways.
Reflux of liquids from the stomach to the esophagus occurs commonly after a meal. If this liquid refluxate were to enter the oropharynx, it could result in aspiration. Distention of the esophagus at rates slower than those that occur with air delivery during a belch results in contraction of the UES, particularly when the proximal esophagus is distended. During a gastroesophageal reflux event, the UES pressure increases more than the increase in intraesophageal pressure, thus preventing passage of material into the pharynx. It is controversial whether distention of the esophagus with acid enhances this response. Distention of the esophagus is also associated with closure of the vocal cords as an added airway-protective mechanism. Finally, stimulation of the hypopharynx with water results in vocal cord closure, a reflex mediated by CN IX that can serve to prevent aspiration from refluxed liquids or boluses that fail to clear the esophagus during deglutition.
Pharynx and Upper Esophageal Sphincter During Belching
During the act of belching gas passes abruptly from the stomach into the esophagus, causing abrupt esophageal distention. The passage of gastric gas under pressure is facilitated by the LES, which remains open, and frequent contractions of abdominal muscles occur during belching. The esophageal distention results in neurally mediated reflex relaxation. The UES opening results from the reflex response and also from the pressure of the gas being forced out through the sphincter. The UES response to belching is of slower onset and longer duration than that seen with deglutition. The UES pressure fall results from both a true inhibition of sphincter tone as well as anterior traction on the sphincter by the suprahyoid muscles that pull the hyoid and larynx forward. The vocal cords close before the onset of UES opening, thus preventing inadvertent aspiration of liquid contents that might accompany the expulsion of air.
Pharynx During Vomiting
During vomiting material is rapidly expelled from the stomach through the esophagus and oropharynx. In the initial phase of vomiting the constrictor muscles of the pharynx are relaxed and the pharyngeal dilator muscles are contracted. The UES is relaxed and pulled open by the muscles that move the hyoid and larynx superiorly and anteriorly. The vocal cords are actively closed to prevent aspiration.
Interactions between Oral Cavity, Pharynx, and Respiratory System
In humans, evolutionary changes in the anatomy of passages that subserve respiration, swallowing, and speech has resulted in a common chamber for intake of air and food and for speech. As a result, humans have lost the capacity to swallow and breathe or speak at the same time. This has necessitated the evolution of neural control systems to coordinate swallowing and respiration. Many of the muscles that are involved in deglutition also participate in respiration. There are not separate motor neuron pools for each function. Motor neurons for a given muscle can be active during both processes. Coordinated control between the swallowing and respiratory centers is conveyed through interneurons.
Most swallows occur during the expiratory phase of respiration. During swallowing, the vocal cords are apposed and respiration is interrupted. After deglutition, respiration is resumed in the expiratory phase. The direction of airflow with expiration would help prevent aspiration of any bolus material prematurely spilled from the oral cavity before the swallow or left behind in the hypopharynx after a swallow. This coordination is altered by stress on the deglutitive or respiratory systems. With rapidly repeated swallows, respiration is more likely to halt and resume with inspiration. Also, in the presence of increased respiratory loads and changes in lung volume, swallowing may be associated with halting and resumption of swallowing during inspiration, thus predisposing to aspiration.
During inspiration the UES pressure increases, which serves to direct airflow into the larynx instead of the esophagus. During inspiration, the resulting subatmospheric pressure could collapse the airway. This possibility is countered by the action of those oropharyngeal muscles capable of dilating the airway, such as the genioglossus and stylopharyngeus, and tensor veli palatini. During expiration, activation of muscles such as the pharyngeal constrictors can modulate the resistance to airflow.
