
Abstract
The prevalence of Plasmodium falciparum malaria in Zanzibar has reached historic lows. Improving control requires quantifying malaria importation rates, identifying high-risk travelers and assessing onwards transmission.
Estimates of Zanzibar's importation rate were calculated through two independent methodologies. First, mobile phone usage data and ferry traffic between Zanzibar and mainland Tanzania were re-analyzed using a model of heterogeneous travel risk. Second, a dynamic mathematical model of importation and transmission rates was used.
Zanzibar residents traveling to malaria endemic regions were estimated to contribute 1–15 times more imported cases than infected visitors. The malaria importation rate was estimated to be 1.6 incoming infections per 1,000 inhabitants per year. Local transmission was estimated too low to sustain transmission in most places.
Malaria infections in Zanzibar largely result from imported malaria and subsequent transmission. Plasmodium falciparum malaria elimination appears feasible by implementing control measures based on detecting imported malaria cases and controlling onward transmission.
Similar content being viewed by others

Introduction
The expansion of road, rail and air transport networks and their increasing affordability contribute to the spread of vector-borne diseases through human and vector movement1,2. The relevant concept for malaria was named “vulnerability” by the World Health Organization (WHO) and defined qualitatively as “the frequent influx of infected individuals or groups and/or infective anophelines”3; quantitatively, the rate of malaria importation includes all parasites that cross the border in humans and vectors. The impact of vulnerability depends on an area's “receptivity” to malaria which reflects the conditions of transmission “through the abundant presence of vector anophelines and the existence of other ecological and climatic factors”3. Receptivity is defined quantitatively as the effective reproduction number Rc , which describes the expected number of secondary human infections originating from a single, untreated infected human taking into account vector control measures4,5. As part of renewed effort towards malaria elimination addressed in the Global Malaria Action Plan (GMAP), the malaria Eradication Research Agenda (MalERA) highlighted the importance of modeling strategies in defining vulnerability to plan for sustainable elimination and prevent reintroduction6,7, especially in areas where malaria prevalence has been reduced but receptivity is still favorable to transmission8.
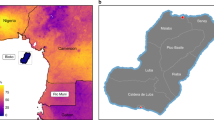
In Zanzibar where the main malaria pathogen is Plasmodium falciparum, the introduction of artemisinin-based combination therapy in 2003 and the escalating ownership of insecticide-treated nets9,10 resulted in an important decrease in malaria prevalence (Figure 1)11. Therefore, the Zanzibar Minister of Health commissioned a report to assess the feasibility of malaria elimination12,13, which highlighted the risk that cases may be imported from surrounding malaria-endemic regions of mainland Tanzania (Figure 1). Recent approaches to quantifying human mobility patterns point to novel insights through the analysis of mobile phone records14 and initial estimates of malaria importation based on such records estimated between 1 and 12 infections imported each year per 1,000 Zanzibari citizens15. Uncertainty in the estimated importation rate spanned a critical value; at the lowest estimates of malaria importation rates, malaria elimination was cost-saving and sustainable, but at the upper estimates, controlling malaria was optimal.

Map of Zanzibar.
(a) Zantel coverage regions in mainland Tanzania15, (b) Zanzibar and its prevalence rate (%) on the two main islands: Unguja and Pemba
Strategic planning for the future of malaria control therefore demands refining the estimate of malaria importation rates to narrow the uncertainty, which could sway the decision of when and whether to eliminate malaria compared with a strategy of control in Zanzibar or elsewhere in Africa13. Here, the concept of vulnerability has been rigorously defined and analyzed to identify high-risk travelers and the most important paths of malaria importation. In addition, mathematical models assuming heterogeneous exposure to malaria, recent malaria surveys and mobile phone usage records and ferry traffic data were used to re-estimate malaria importation rates, cross-validate those estimates and narrow the uncertainty. Finally, the interplay between malaria importation and subsequent local transmission was evaluated through the relationship between vulnerability, receptivity and local malaria dynamics.
Results
The islands of Zanzibar have strong transport connections to mainland Tanzania where transmission levels are higher. While daily flights primarily bring tourists from non-endemic regions, ferry travel from Dar es Salaam and informal movement on small fishing and trading vessels likely represent the highest risk pathways for imported infections.13.
Contributions of residents, visitors and immigrants to imported malaria
A recently published mathematical model identified four ways that malaria parasites can be imported into a region16: human residents of the region can become infected while traveling abroad and then return home for the duration of the infection; human visitors can spend time in Zanzibar after being infected elsewhere; human immigrants infected elsewhere can move permanently into the region; and infected mosquitoes can travel into the region (Figure 2). The frequency of importation through each one of these routes differs, as does the significance of each importation event for potential onwards transmission; some infections are unlikely to contribute to local transmission depending on the receptivity of the place where infections were imported and the duration of stay. Each untreated malaria infection imported in a resident or an immigrant would be counted the same; both are likely to remain in the country as long as they are infectious, providing a long window during which they may infect mosquitoes locally, even though the number of immigrants is likely very small17. Each infected human visiting the region, however, tends to have short visits compared with the long infectious period of malaria. To produce a standardized importation rate, each one of these visitors must be discounted by the length of stay relative to the duration of an untreated infection18. Since Zanzibar is an archipelago separated from the mainland by approximately 40 km, malaria infections imported by mosquitoes are assumed to be rare and they have not been considered further here19.

Qualitative assessment of malaria importation to Zanzibar and its influence on local malaria dynamics.
The pathogen can be introduced into the island according to four ways: 1) Zanzibar residents (R) can become infected while traveling abroad and bring it home; 2) infected visitors (V) to Zanzibar can bring the pathogen from mainland Tanzania; 3) infected immigrants (M) travel and settle permanently in Zanzibar; 4) infected vectors travel to Zanzibar either flying or passively carried out by wind or riding along human means of transportations. Once introduced, the probability for further transmission is based on the length and the receptivity of the area where the pathogen is imported, defining the net importation rate.
Analysis of length-of-stay from phone records in Tanzania suggests that the median visitor trip length to Zanzibar was approximately 13 days, while the duration of untreated malaria infections is on average 200 days18. If there were roughly as many infected returning residents as there were visitors to a region, then on average, each resident who returned infected and who was not properly diagnosed and treated would count for 15 infected visitors. The relative importance of transmission routes can be checked by doing a sensitivity analysis on the number of exogenous infections brought by residents and visitors and the length of stay of visitors relative to the duration of infection (Figure 3). For example, with similar numbers of exogenous infections and visitors staying 10% of the infection duration, residents contribute to 90–95% of imported malaria. These estimations assume both residents and visitors stay in the same places in Zanzibar.

Relative importance of residents on malaria importation.
Contribution of resident travelers to the net malaria importation rate as a function of the number of imported infections from visitors versus residents (δ v/δ r) and the length of stay for visitors (Tv ). The solid red line represents the contribution threshold below which residents contribute to more than 50% to malaria importation.
Estimating the vulnerability of Zanzibar
Simply counting the number of travelers to Zanzibar may not provide accurate estimates of malaria importation, so estimation of malaria risk was done in two ways for cross-validation. First, estimates of importation were made from mobile phone usage records and ferry traffic data. The proportion of residents infected while travelling abroad can be estimated from the sum of their time spent at various levels of risk. An important caveat is that infection risk while traveling is highly heterogeneous20,21. Second, a mathematical model was developed that could explicitly take into account the dynamics of transmission and malaria importation; this model was applied to cross-sectional parasite surveys from Zanzibar in 200711 to estimate the importation rate and Rc .
The first method, based on mobile phone usage data, ferry traffic and heterogeneous risk of infection gives an estimate of between 0.7 and 6 infections imported by residents per 1,000 Zanzibaris, based on the risk of malaria for the entire regions of origin, or their principal cities, respectively (Table 1). Assuming, half of ferry passengers are visitors to Zanzibar22, the annual number of infectious visitors varied from 8.5 to 8.8 per 1,000. The net visitor importation rate is weighed by the visitor length of stay respectively to the duration of infection and varies between 0.7 and 0.9 infections per 1,000 Zanzibaris (Table 1). The total net importation rate to Zanzibar varies between 1.6 if estimates are based on the risk measured in the main cities of each region of origin to 6.7 if estimates are based on transmission risk measured in the region (Table 1). These estimates would also vary up or down depending on the ratio of residents to visitors. As most travel is assumed to occur between Zanzibar and main cities on mainland Tanzania, where malaria risk is low, the importation net rate of 1.6 infections per 1,000 inhabitants per year is kept as a baseline reference for further comparisons.
 representzs visitor net importation rate, the number of infected visitors weighed by the duration of the trip, Tv , relatively to the duration of infection. The risk of infection is calculated with risk estimates from the main city or from the rest of the region of origin on mainland Tanzania.
representzs visitor net importation rate, the number of infected visitors weighed by the duration of the trip, Tv , relatively to the duration of infection. The risk of infection is calculated with risk estimates from the main city or from the rest of the region of origin on mainland Tanzania.In urban Unguja, where an epidemiological survey estimated a parasite rate of 0% (95% Confidence Interval: 0–0.2%)11, the upper bound for the net malaria importation rate, if Rc were equal to 0, was 3.7 per 1,000 inhabitants per year; the lower bound was 0 (Figure 4a). The midpoint of the estimates, 1.6 infections per 1,000 inhabitants per year, is consistent with the findings from mobile phone data analysis. Assuming malaria importation rates tend to be highest in the urban areas that are near the ferry landing, malaria prevalence in rural Unguja and Pemba likely provides more information about local transmission than about imported malaria. Using the estimate from the mobile phone survey of 1.6 imported infections, per 1,000 per year, Rc ranges between 0 and 0.56 in urban Unguja (Figure 4a), between 0.71 and 0.91 in rural Unguja (Figure 4b) and between 0.92 and 0.98 in Pemba (Figure 4c).

Quantitative assessment of malaria importation.
Vulnerability (the number of imported malaria per year per 1,000 inhabitants, δ) and receptivity (the effective reproductive number, Rc ) in three different epidemiological settings in Zanzibar: (a) urban Unguja with a parasite rate of 0% (95% Confidence Interval: 0–0.2%), (b) rural Unguja with a parasite rate of 0.5% (0.3–0.9) and (c) Pemba with a parasite rate of 1.5% (1–2.1). The solid black line represents the mean annual number of imported malaria cases and the dashed black lines the upper and lower bounds of the 95% confidence interval represented by the grey area. The red dotted line represents the empirical estimation of δ in Zanzibar according to travel assessment survey, which is of 1.6 imported malaria cases per 1,000 inhabitants per year.
Relationships between vulnerability, receptivity and malaria prevalence in Zanzibar
The models outlined here illustrate the relationship between the net importation rate, Rc and the prevalence rate for contexts outside of Zanzibar. For the range of malaria importation rates (0 to 10 incoming infections per 1,000 per year) and Rc (0 to 1) values used here, parasite rate estimates are found to be below 8% (Figure 5a). Assuming the malaria importation rate to Zanzibar is less than 1.6 cases, malaria prevalence would not exceed 2% unless Rc was close or equal to 1 (Figure 5a).

Quantitative assessment of the impact of malaria importation on local malaria dynamics.
The effect of vulnerability (the number of imported malaria per year per 1,000 inhabitants, δ) and of receptivity (the effective reproductive number, Rc ) on, (a) the parasite rate (PR) and (b) the proportion of local infection among all malaria infection. The red dashed line represents the empirical estimation of δ in Zanzibar according to the travel assessment survey, which is of 1.6 imported malaria cases per 1,000 inhabitants per year. The solid red line represents the contribution threshold above which local infections contribute to more than 50% to total malaria prevalence
Imported malaria not only brings malaria parasites to the island, but it also adds to local transmission23. As Rc and the net importation rate increase, the proportion of local infection amid all infections increases. Under our current estimation of net importation rate to Zanzibar of 1.6 and as Rc is close to one in rural Zanzibar, even low undetected net importation rate triggers important local non-endemic transmission with high parasite rate that might delay malaria elimination (Figure 5b). Nevertheless, the overall estimates of Rc are below 1, which suggests that if malaria importation ceased, endemic malaria transmission would eventually end except in a few residual local transmission foci.
Discussion
Strategic priorities of national malaria control programs vary depending on many factors, including the natural potential for endemic malaria transmission, the levels of control that have been achieved and the proximity to other malaria endemic countries. In countries where malaria is rare, malaria importation is of primary concern. Countries with well-developed health systems, good surveillance through national case reporting and no local malaria can simply count the number of malaria cases that occur. In the United States in 2008, 1,298 detected malaria cases were imported mainly in tourists inadequately protected by chemoprophylaxis and immigrants and none triggered any further transmission24; autochthonous cases do occur, but only rarely25. Countries that have recently reduced their malaria burden, but that have strong human travel connections with other malaria endemic countries26 with poorly developed health systems, or some level of ongoing transmission must devise alternative methods for estimating malaria importation rates. Key information is required to set up appropriate measures: contributions of various routes of malaria importation, reliable estimates of malaria importation rates and of the potential for local transmission and the total impact of these quantities on the local endemic and non-endemic transmission. These estimates must also be made in a highly dynamic environment as neighboring countries also control malaria. Our analysis suggests that citizens of Zanzibar who travel to malaria endemic regions are likely to be the single most important source of importation. Mobile phone data analysis estimates that less than 1.6 malaria infections are imported per 1,000 Zanzibar residents every year, with a credible value of less than 3.7 infections per 1,000 people per year according to mathematical models. This analysis suggests that Rc is below 1 in most places, as most local transmission is driven by imported malaria. Therefore, our results suggest that, if current levels of control are sustained, malaria would eventually disappear from most of the island, except possibly in a few residual foci if no imported infections occurred.
Therefore, enhanced prevention and control strategies should aim at mitigating pathogen importation to move towards malaria elimination and prevent reintroduction. The government could provide free chemoprophylaxis through the health system to Zanzibar residents travelling to endemic mainland using drugs that minimize the risk of developing resistance27. As immunity to malaria parasite declines in low endemic settings, such travelers are even more vulnerable to infection, stressing the rationale to distribute prophylaxis. In addition, each case of infection should be reported to health authorities, which highlights the need for enhanced surveillance28. Measures should include border screening especially at ports of landing, active case detection and investigation to set up appropriate reactive measures in the environment of the cases. Surveillance tools rely on the availability of sensitive and specific diagnostic tools such as rapid diagnostic tests (RDTs), which require further improvement29. Finally, vector control measures could mitigate the importation of infectious anopheles, for instance by using insecticide in planes flying from malaria endemic region30, even though this is likely to be a minor issue. Some of these measures may be technically, economically and operationally challenging and require prior feasibility assessment combined with public health education campaigns.
Imported malaria contributes differently to local dynamics depending on the number of incoming pathogens and the length of stay as addressed here, but also on when and where malaria is imported. Formal and informal human movements are increasingly becoming amenable to study as humans use mobile phones. Nevertheless, mobile phone usage data are subject to biases based on data availability, ownership and usage patterns. Principal malaria transmission season on mainland starts between November and January and ends approximately between April and June. Therefore, the current survey extending over a three-month period from October to December only captures a subset of potential malaria importation. Furthermore, the available Zantel mobile records did not provide further information on local cell tower usage, so it was not known where residents and visitors stayed in Zanzibar. As a result, even though malaria importation could be quantified for the main regions of Zanzibar, no local foci of residual transmission can be identified at higher spatial resolutions. Finally, even though general population movement to and from Zanzibar mainly rely on ferry transportation, informal movement on small fishing boats also represent a pathway for malaria importation and can only be partially captured through mobile phone records. These movements create hotspots of malaria importation mainly in coastal communities. As health authorities know these hotspots, the Zanzibar Malaria Control Programme (ZMCP) can intervene and mitigate malaria importation in these communities.
Some of these limitations have been addressed by cross-validating estimates with two completely independent methods using different data. Despite the uncertainties, mobile phone usage records have provided useful and reasonably accurate information about the lengths of stay in Zanzibar and the relative importance of various routes of malaria importation. These estimates could be improved through further studies focusing on the places where people stay in Zanzibar and gathering mobile phone data over a longer study period to better take into account malaria seasonality. To move towards elimination, additional tools should be used to complement current assessment especially in terms of risk mapping. The Malaria Atlas Project (MAP) provides with endemicity maps based on prevalence surveys at a global, continental or country level. Using mathematical models31,32,33, these maps were converted to EIR risk maps, a more relevant measure for risk transmission15. Nevertheless, as Zanzibar is getting closer to elimination, finer scale mapping based on environmental, epidemiological, population, vector, social and economical factors is required to identify residual foci in order to implement rapid localized response.
As very low levels of transmission are reached, programs move from a focus on control to a focus on pre-elimination and elimination and finally prevention of re-introduction. Quantitative approaches to human movement and the spread of malaria are increasingly useful for government to appropriately decide when shifting efforts to stemming importation. Mobility patterns can be used to estimate the import of infectious disease into geographic regions with low endemic states. The importance of control methods will depend on the vectors and immuno-epidemiology of the pathogen, as for dengue which has a shorter infectious period, daytime biting vectors and life-long immunity34. As methods improve for quantifying malaria importation and transmission, they can be applied more widely to advise countries on strategic planning across the region and worldwide.
Methods
Contributions of residents, visitors and immigrants to imported malaria
The standardized contributions of imported malaria from all four routes can be added to estimate the malaria importation rate, denoted δ, reported as the equivalent number of untreated new human infections, per thousand populations, per year. Quantitatively, the way residents or visitors influence malaria dynamics mainly depends on the number of infections brought by residents and visitors (δr and δv ) and the length of stay of visitors (Tv ) relative to the duration of infections in residents (1/r). Assuming infectivity is constant over the duration of infection, the relative contribution of one imported malaria case by a resident compared to one by a visitor is estimated according to the following formula:  .
.
Estimating the vulnerability of Zanzibar
Estimating the net malaria importation rate from mobile phone usage data
Anonymized phone call record data, which included both the time each call was made and the location of the nearest mast that each call was routed through, was used to construct trajectories of the movements of individuals over time15. About 9 out 10 Tanzanians have access to a mobile phone35,36 and the Zanzibar telecom (Zantel) mobile phone operator has approximately a 99% market share on Zanzibar35, this likely comprises a representative sample of Zanzibari residents. This does not hold for Tanzania as a whole, as Zantel had only approximately a 10% share of the market on the mainland during the data period. Mobile phone usage records encompassing a three-month period from October to December 2008 were obtained, as the company only archives three months of records. This covers the busiest period in terms of travel to and from Zanzibar and therefore enables conservative upper estimates of malaria importation. Zanzibar residents were identified based on the assumptions that they made the majority of their calls on Zanzibar; the rest were considered to be visitors. Each individual call and message was spatially referenced to one of six areas: Arusha, Dar es Salaam, Dodoma, Mbeya, Mwanza and Zanzibar (Figure 1). Only those making regular calls (more than four a month) with apparent overnights trips were considered, as day trips are of little risk considering the mosquito night biting habits37. The final dataset included 67,236 trips made by visitors between Zanzibar and mainland and 73,095 trips made by for Zanzibari residents, 88% of Zanzibari users did not travel long distance during the study period.
Mobile phone data inform on individual trips made by Zanzibar residents to endemic areas on the mainland, more specifically, where they went and how long they stayed (length of stay, Tr ). The level of malaria endemicity can be measured by the daily entomological inoculation rate (EIR or E), which corresponds to the number of infectious bites received per person per day. Recent research efforts have provided spatial quantification of P. falciparum endemicity enabling estimation of EIR at the locations where Zanzibar residents visit38,39. Two types of population-weighted estimates for EIR were provided based on the endemicity level for each Zantel region either for the entire regions of origin, or their principal cities disaggregated by month to take into account transmission seasonality. For residents, the individual probability of getting infected by malaria parasites during each trip is described by the following formula for the whole trip attack rate that takes into account heterogeneous biting  31,32,33. b represents the probability that an infectious bite leads to infection and α is an index of heterogeneous risk during a trip in an area with average daily exposure E and α = 4.2 so that approximately 20% of the population gets 80% of all the risk20. Combining the information collected with mobile phones to the formula of heterogeneous biting allow for estimating the total number of imported infections from residents, δr , over all Nr people trips made in during the study period, which is
31,32,33. b represents the probability that an infectious bite leads to infection and α is an index of heterogeneous risk during a trip in an area with average daily exposure E and α = 4.2 so that approximately 20% of the population gets 80% of all the risk20. Combining the information collected with mobile phones to the formula of heterogeneous biting allow for estimating the total number of imported infections from residents, δr , over all Nr people trips made in during the study period, which is  .
.
As the mobile phone data do not cover all visitors to Zanzibar, the risk from each individual visitor trip provided by mobile phone data was extrapolated to the number of visitors travelling each month to Zanzibar provided by ferry traffic data. The number of infected visitors traveling to Zanzibar from mainland Tanzania, δv , is calculated according to the following formula  with Nv the overall number of visitors traveling to Zanzibar according to ferry traffic data and X the parasite rate for each region of origin or their principal cities, disaggregated by month. To compare the respective impact of imported malaria from visitors on local transmission to the one from residents, the number of infected visitors was standardized using the formula
with Nv the overall number of visitors traveling to Zanzibar according to ferry traffic data and X the parasite rate for each region of origin or their principal cities, disaggregated by month. To compare the respective impact of imported malaria from visitors on local transmission to the one from residents, the number of infected visitors was standardized using the formula  , with Tv the duration of their trip and r approximately 0.005 d−1.
, with Tv the duration of their trip and r approximately 0.005 d−1.
Estimating the net malaria importation rate from a mathematical model
The second method, which is based on a model of importation and transmission, estimates the malaria importation rate as a function of malaria prevalence and Rc . The model considers only imported malaria cases that are not treated. The dynamics of malaria infection at low intensity can be described by a slightly modified Ross-Macdonald model40,41. At low prevalence, the model is simplified to  32. The expression reflects the local transmission of the disease. But the overall malaria dynamics should also encompass imported malaria and the expression can be improved by explicitly adding per-capita importation rate δ:
32. The expression reflects the local transmission of the disease. But the overall malaria dynamics should also encompass imported malaria and the expression can be improved by explicitly adding per-capita importation rate δ:  . At the equilibrium,
. At the equilibrium,  and the net malaria importation rate is estimated by the following formula:
and the net malaria importation rate is estimated by the following formula:  .
.
Relationships between vulnerability (δ), receptivity (Rc ) and malaria prevalence in Zanzibar
The estimates of receptivity and vulnerability influence malaria prevalence and the proportion of local infection amid all infections. Malaria prevalence (X) at equilibrium is estimated by solving  . In our model, the local force of infection is described by RcXr, therefore the proportion of local infection amid the total number of infections in the area of interest is described by the following formula
. In our model, the local force of infection is described by RcXr, therefore the proportion of local infection amid the total number of infections in the area of interest is described by the following formula  .
.
References
Stoddard, S. T. et al. The role of human movement in the transmission of vector-borne pathogens. PLoS Negl Trop Dis 3, e481 (2009).
Tatem, A. J., Rogers, D. J. & Hay, S. I. Global transport networks and infectious disease spread. Adv Parasitol 62, 293–343 (2006).
World Health Organization. . Technical report Series 324 (1966).
Anderson, R. M. & Anderson, R. M. & May, R. M. Infectious diseases of humans (Oxford University Press, Oxford, 1991).
Dietz K. . The estimation of the basic reproduction number for infectious diseases. Stat Methods Med Res 2, 23–41 (1993).
Alonso, P. L. et al. A research agenda to underpin malaria eradication. PLoS Med 8, e1000406 (2011).
The malERA Consultative Group on Modeling. A research agenda for malaria eradication: modeling. PLoS Med 8, e1000403 (2011).
Sabot, O. et al. Costs and financial feasibility of malaria elimination. Lancet 376, 1604–15 (2010).
Bhattarai, A. et al. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PLoS Med 4, e309 (2007).
Stich, A. H. et al. Insecticide-impregnated bed nets reduce malaria transmission in rural Zanzibar. Trans R Soc Trop Med Hyg 88, 150–4 (1994).
Zanzibar Malaria Control Program. (Zanzibar, 2008).
Tatem, A. J. et al. Ranking of elimination feasibility between malaria-endemic countries. Lancet 376, 1579–91 (2010).
Zanzibar Malaria Control Programme. Malaria Elimination in Zanzibar: A Feasibility Assessment. 1–81 (2009).
Gonzalez, M. C., Hidalgo, C. A. & Barabasi, A. L. Understanding individual human mobility patterns. Nature 453, 779–82 (2008).
Tatem, A. J. et al. The use of mobile phone data for the estimation of the travel patterns and imported Plasmodium falciparum rates among Zanzibar residents. Malar J 8, 287 (2009).
Cosner, C. et al. The effects of human movement on the persistence of vector-borne diseases. J Theor Biol 258, 550–60 (2009).
Gossling, S. & Schulz, U. Tourism-Related Migration in Zanzibar, Tanzania. Tourism Geographies 7, 43–62 (2005).
Snow, R. W. & Gilles, H. M. in Essential Malariology (eds. Warrell D. A., & Gilles H. M., eds.) 85–106 (Arnold, London, 2002).
Service, M. W. Mosquito (Diptera: Culicidae) dispersal—the long and short of it. J Med Entomol 34, 579–88 (1997).
Smith, D. L., Drakeley, C. J., Chiyaka, C. & Hay, S. I. A quantitative analysis of transmission efficiency versus intensity for malaria. Nat Commun 1, 108 (2010).
Smith, D. L., Dushoff, J. & McKenzie, F. E. The risk of a mosquito-borne infection in a heterogeneous environment. PLoS Biol 2, e368 (2004).
Zanzibar Ministry of Communication and Transport. Ferry Passenger data: 2006–2007. (2008).
Cohen, J. M., Moonen, B., Snow, R. W. & Smith, D. L. How absolute is zero? An evaluation of historical and current definitions of malaria elimination. Malar J 9, 213 (2010).
Mali, S., Steele, S., Slutsker, L. & Arguin, P. M. Malaria surveillance – United States, 2008. MMWR Surveill Summ 59, 1–15.
MacArthur, J. R. et al. Probable locally acquired mosquito-transmitted malaria in Georgia, 1999. Clin Infect Dis 32, E124–8 (2001).
Tatem, A. J. & Smith, D. L. International population movements and regional Plasmodium falciparum malaria elimination strategies. Proc Natl Acad Sci U S A 107, 12222–7 (2010).
The malERA Consultative Group on drugs. A research agenda for malaria eradication: drugs. PLoS Med 8, e1000402 (2011).
The malERA Consultative Group on Monitoring, E. and Surveillance. A research agenda for malaria eradication: monitoring, evaluation and surveillance. PLoS Med 8, e1000400 (2011).
The malERA Consultative Group on diagnoses and diagnostics. . A research agenda for malaria eradication: diagnoses and diagnostics. PLoS Med 8, e1000396 (2011).
The malERA Consultative Group on vector control. A research agenda for malaria eradication: vector control. PLoS Med 8, e1000401 (2011).
Smith, D. L., Dushoff, J., Snow, R. W. & Hay, S. I. The entomological inoculation rate and Plasmodium falciparum infection in African children. Nature 438, 492–5 (2005).
Smith, D. L. & McKenzie, F. E. Statics and dynamics of malaria infection in Anopheles mosquitoes. Malar J 3, 13 (2004).
Smith, D. L., McKenzie, F. E., Snow, R. W. & Hay, S. I. Revisiting the basic reproductive number for malaria and its implications for malaria control. PLoS Biol 5, e42 (2007).
Whitehorn, J. & Farrar, J. Dengue. Br Med Bull 95, 161–73 (2010).
Tanzania Communications regulatory Authority. (ed. TCR) (Dar es Salam, 2009).
International Communication Union. (2007).
Sinka, M. E. et al. The dominant Anopheles vectors of human malaria in Africa, Europe and the Middle East: occurrence data, distribution maps and bionomic precis. Parasit Vectors 3, 117 (2010).
Hay, S. I. et al. A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med 6, e1000048 (2009).
Smith, D. L. & Hay, S. I. Endemicity response timelines for Plasmodium falciparum elimination. Malar J 8, 87 (2009).
Mac Donald, G. The epidemiology and control of malaria (Oxford University Press, London, 1957).
Ross, R. The prevention of malaria (John Murray, London, 1910).
Acknowledgements
The author would like to thank members of the Zanzibar Malaria Control Programme. ALM, HR, DLS, AJT are supported by a grant from the Bill and Melinda Gates Foundation (#49446)(http://www.gatesfoundation.org). SIH is funded by a Senior Research Fellowship from the Wellcome Trust (#079091). DLS, AJT and SIH also acknowledge funding support from the RAPIDD program of the Science & Technology Directorate, Department of Homeland Security and the Fogarty International Center, National Institutes of Health (http://www.fic.nih.gov). APP is paid by a Biomedical Resources Grant from the Wellcome Trust (#091835). This work forms part of the output of the Malaria Atlas Project (MAP, http://www.map.ox.ac.uk), principally funded by the Wellcome Trust, U.K (http://www.wellcome.ac.uk). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
DLS and ALM jointly conceived and led the research. ALM, DLS, AT and HR developed the logic of the analyses. ALM performed the analyses and wrote the manuscript. AT, SIH, JMC and APP contributed to the analyses. All authors discussed the study design and results and contributed to drafting and revising the manuscript and figures.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareALike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Le Menach, A., Tatem, A., Cohen, J. et al. Travel risk, malaria importation and malaria transmission in Zanzibar. Sci Rep 1, 93 (2011). https://doi.org/10.1038/srep00093
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep00093
This article is cited by
-
Livelihood activities, human mobility, and risk of malaria infection in elimination settings: a case–control study
Malaria Journal (2023)
-
Risk of imported malaria infections in Zanzibar: a cross-sectional study
Infectious Diseases of Poverty (2023)
-
An insight to better understanding cross border malaria in Saudi Arabia
Malaria Journal (2023)
-
Multiplexed ddPCR-amplicon sequencing reveals isolated Plasmodium falciparum populations amenable to local elimination in Zanzibar, Tanzania
Nature Communications (2023)
-
Modelling the impact of interventions on imported, introduced and indigenous malaria infections in Zanzibar, Tanzania
Nature Communications (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
