1993–2004
The dawn of the therapeutic era in MS

An appreciation that aberrant immunological responses were important in multiple sclerosis led to the development and approval of interferon-β 1b. Glatiramer acetate and additional formulations of interferon-β soon followed, and these injectable therapies were the mainstays of multiple sclerosis therapy for a decade.
Read More- Injectable
- Interferon-Beta
- Glatiramer Acetate
2004
The first monoclonal antibody therapy

A new therapeutic option became available with the approval of natalizumab, which reduces migration of lymphocytes across the blood–brain barrier by inhibiting the interaction between the α4β1 integrin on lymphocytes with VCAM1 on vascular endothelial cells.
Read More- Injectable
- Antibodies
2005
The risk of natalizumab-associated PML is revealed
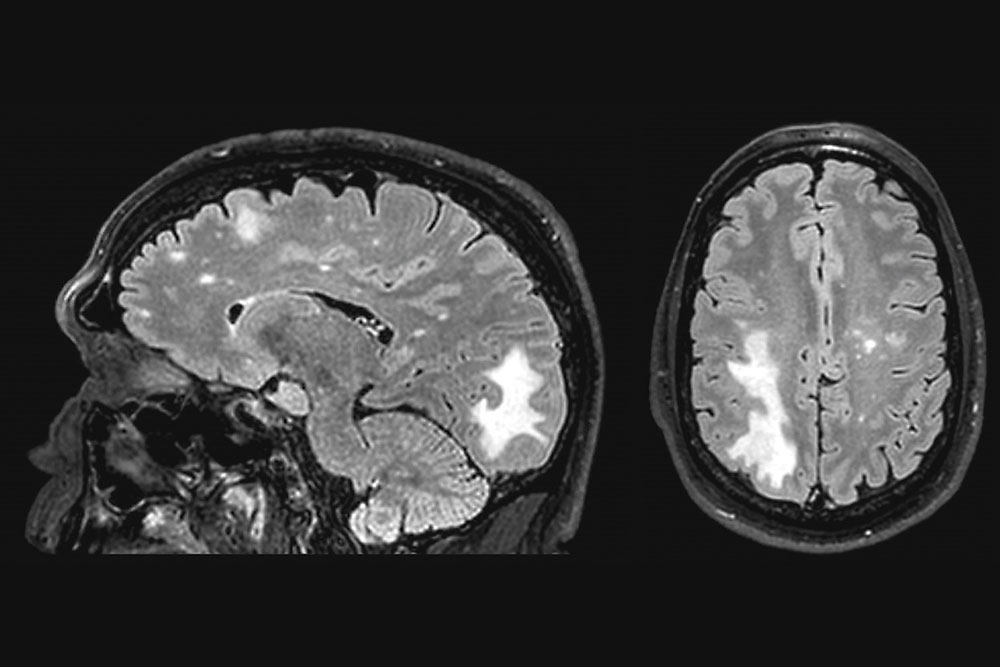
After its approval in 2004, natalizumab was withdrawn from the market in 2005 owing to two cases of progressive multifocal leukoencephalopathy that were associated with the treatment. The therapy was reintroduced — with improved safety warnings — in 2006, and subsequent research has led to ongoing refinement of approaches to risk stratification.
Read More- Injectable
- Antibodies
2010–2013
Oral drugs expand therapeutic options

Three oral therapies for relapsing–remitting multiple sclerosis were approved between 2010 and 2013: fingolimod, teriflunomide and dimethyl fumarate. These three molecules all inhibit the immune activation in the brain that is characteristic of the disease. The option to use oral, rather than injectable, therapies reduced the burden of treatment.
Read More- Oral
- Dimethyl Fumarate
- Teriflunomide
- Fingolimod
2014–2016
Highs and lows with second-generation monoclonal antibodies
Alemtuzumab and daclizumab, which both suppress the immune system but via different mechanisms, were approved for the treatment of relapsing–remitting multiple sclerosis in 2014 and 2016, respectively. However, in 2018, daclizumab was withdrawn from the market owing to concerns of serious adverse effects.
Read More- Injectable
- Antibodies
2014–2018
More treatments create clinical dilemmas

As the therapeutic options for multiple sclerosis increased, several clinical dilemmas arose, and clinicians had to start making decisions about which therapy to use, when to treat patients, and when and how to switch medications in patients with a suboptimal response. These clinical dilemmas continue today, but treatment strategies continue to be refined.
Read More- Injectable
- Interferon-Beta
- Antibodies
- Oral
- Dimethyl Fumarate
- Teriflunomide
- Fingolimod
- Cladribine
- Glatiramer Acetate
2017
The story of cladribine reaches its climax
After a long and, at times, uncertain route to regulatory approval, oral cladribine was approved for treatment of relapsing–remitting multiple sclerosis in 2017. It is currently the only oral drug that has the potential for pulsed immune reconstitution, and its mechanism of action differs from that of other current treatments for multiple sclerosis.
Read More- Oral
- Cladribine
2017
Targeting B cells leads to breakthrough therapy

As B cells emerged as key players in the multiple sclerosis disease process, anti-CD20 antibodies that deplete circulating B cells were tested in patients with relapsing–remitting and progressive multiple sclerosis. The results were groundbreaking.
Read More- Injectable
- Antibodies
2018
Progressive and aggressive MS — new frontiers emerge

The huge progress made in the treatment of relapsing–remitting multiple sclerosis in the past 25 years has not been replicated for progressive or aggressive forms of multiple sclerosis. However, the latest trials in these areas have provided breakthroughs, laying the foundations for another successful 25 years of MS treatment.
Read More- Injectable
- Oral
Nature Milestones: Treatment of multiple sclerosis
Download the Treatment of multiple sclerosis timeline and all the Milestone articles in one PDF.
Topics