
Abstract
Emerging knowledge suggests that post-traumatic stress disorder (PTSD) pathophysiology is linked to the patients’ epigenetic changes, but comprehensive studies examining genome-wide methylation have not been performed. In this study, we examined genome-wide DNA methylation in peripheral whole blood in combat veterans with and without PTSD to ascertain differentially methylated probes. Discovery was initially made in a training sample comprising 48 male Operation Enduring Freedom (OEF)/Operation Iraqi Freedom (OIF) veterans with PTSD and 51 age/ethnicity/gender-matched combat-exposed PTSD-negative controls. Agilent whole-genome array detected ~5600 differentially methylated CpG islands (CpGI) annotated to ~2800 differently methylated genes (DMGs). The majority (84.5%) of these CpGIs were hypermethylated in the PTSD cases. Functional analysis was performed using the DMGs encoding the promoter-bound CpGIs to identify networks related to PTSD. The identified networks were further validated by an independent test set comprising 31 PTSD+/29 PTSD− veterans. Targeted bisulfite sequencing was also used to confirm the methylation status of 20 DMGs shown to be highly perturbed in the training set. To improve the statistical power and mitigate the assay bias and batch effects, a union set combining both training and test set was assayed using a different platform from Illumina. The pathways curated from this analysis confirmed 65% of the pool of pathways mined from training and test sets. The results highlight the importance of assay methodology and use of independent samples for discovery and validation of differentially methylated genes mined from whole blood. Nonetheless, the current study demonstrates that several important epigenetically altered networks may distinguish combat-exposed veterans with and without PTSD.
Similar content being viewed by others

Introduction
Adverse life experiences alter the epigenetic profile1, 2, 3 in a manner that is salient for pathophysiology of post-traumatic stress disorder (PTSD).4, 5, 6 Changes in methylation status of the glucocorticoid receptor gene have been reported previously in combat veterans with PTSD.7 Methylation changes in these same genes were also observed in association with parental trauma, suggesting that such effects may be related to heritable risk profiles.8 Consistent claims were presented by in vivo studies.9, 10 Together, these discoveries drive a strong rationale for screening the epigenetic profiles of patients’ blood to identify next-generation strategies for PTSD risk factors, diagnostics and experimental therapeutics. A growing body of cohort-based studies has linked the epigenetic changes with PTSD development,11, 12, 13 mostly focusing on pre-determined targets such as immunity14, 15, 16 and neuroendocrinology.7, 8, 17, 18
For the present study, strict inclusion–exclusion criteria were used19, 20 to identify a training set comprising 48 male veterans with PTSD (PTSD+) and 51 age-/ethnicity-/gender-matched controls (PTSD−). Control veterans experienced war trauma but were negative for current and past PTSD (Supplementary Table S1). An independent test set comprising 31 PTSD+/29 PTSD− veterans was recruited using the same screening protocol.
Enriched by the differentially methylated genes (DMGs), the epigenetically altered networks are linked to nervous systems' development and function, PTSD-associated somatic complications and endocrine signaling. All of these networks mined from the training set were validated by the test set (Table 1). Subsequently, we consolidated the test and training sets to develop a union set and revaluated the methylation profile using the improved sample size. The result confirmed 65% of the pathways mined from the test and training sets. Going forward, we will consider the methylation profile from this union set as the discovery set to be confirmed in a new validation set, for which subjects are currently being recruited.
Materials and methods
Ethical statement
The Institutional Review Boards of the US Army Medical Research and Materiel Command, the New York University Langone Medical Center (New York, NY, USA), the Icahn School of Medicine at Mt Sinai (New York, NY, USA) and the James J Peters Veterans Administration Medical Center (Bronx, NY, USA) approved this study. Study participants gave written and informed consent to participate. The study was conducted in accordance with the provisions of the Helsinki Declaration.
Cohort recruitment and analysis
The recruitment process involved several steps detailed in the Supplementary Table S1 and in previous communications.19, 20 The training set of 48 PTSD+/51 PTSD− and the test set of 31 PTSD+/29 PTSD− veterans was probed by whole-genome arrays (Agilent, Santa Clara, CA, USA) containing ~27k CpGIs. The outcome was normalized to minimize the confounding factors attributed to batch processing.21 Functional analysis was performed using those DMGs, which encoded CpGIs meeting the cutoff false discovery rate<0.1.
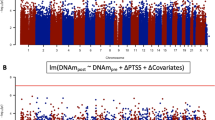
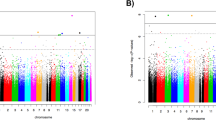
Next, we merged the training and test sets to develop a union set comprising 79 PTSD+/80 PTSD− veterans, which was probed by whole-genome arrays (Illumina, San Diego, CA, USA) containing 450 k probes. The outcome was corrected to minimize heterogeneous cell populations22 and age effects, and was screened at P<0.05 to find DMGs. Available GEO databases are as follows: GSE76401 and GSE85399. ClueGo v2.1.2 and Ingenuity pathway analysis were used for network construction, and pathways that we report met the cutoff of P<0.05.
Results
The primary purpose of the present communication was to identify the functional networks associated with combat-related PTSD, and thereby to provide a better understanding of PTSD pathophysiology. To meet this goal, we recruited 48 PTSD+/51 PTSD− veterans as a training set and 31 PTSD+/29 PTSD− veterans as a test set. To increase the statistical power and to minimize any bias of the Agilent high-throughput array platform, we took two measures. First, we constructed a union set by consolidating the training and test sets, following a recently published strategy.19, 20 Second, we retested the methylation profile, probing the union set using a different array platform manufactured by Illumina. Furthermore, this union set retains sufficient statistical power. Taking a moderate estimate of 50% s.d.'s in probe signals and a relatively conservative estimate for the mean difference (that is, top 1%), 76 people per group should give 95% power to detect an individual probe with a (Bonferroni-adjusted) genome-wide significance of P<1.162931e−07.
Functional analysis of the training set found a host of PTSD-related networks
In the investigation of the 48 PTSD+/51 PTSD− training set, we identified 5578 differentially methylated CpGIs annotated to 3662 genes. We collectively defined the 1698 promoter-bound CpGIs and 157 additional divergent promoter regions as the promoter regions (Supplementary Figure S4A). Altogether, 4721 CpGIs annotated 2401 DMGs that displayed a log2 ratio >0.1 and were defined as hypermethylated. Conversely, 857 CpGIs (672 DMGs) displaying a log2 ratio <0.1 were defined as hypomethylated. The remaining DMGs co-enriched by both hyper- and hypomethylated CpGIs were excluded from the subsequent functional analysis. For the functional analysis, we used those DMGs, which encoded promoter-bound CpGIs, estimated as nearly 60% of total DMGs. Significantly enriched networks with similar functional purposes were grouped together, resulting in four network clusters (Figure 1): nervous system functions (Figure 2a), PTSD-associated somatic complications (Figure 2b), PTSD-relevant endocrine signaling networks (Supplementary Figure S6A) and nervous system development (Supplementary Figure S6B).

Functional enrichment analysis. In all, 352 DMGs encoding promoter-bound differentially methylated CpGIs curated from the training set were enriched for four functional clusters: PTSD-associated somatic complications, PTSD-relevant endocrine signaling, nervous system development and nervous system functions. These clusters were designed to group networks with overlapping functionality. All of these networks were validated by the test set. CRH, corticotrophin-releasing hormone; DMG, differently methylated gene; GC, glucocorticoid; HPA, hypothalamus–pituitary–adrenal; PTSD, post-traumatic stress disorder; REM, rapid eye movement.

(a) Network cluster annotated to nervous system functions significantly enriched by DMGs in the training set. (b) Network cluster annotated to PTSD-associated somatic complications significantly enriched by DMGs in the training set. (c) Network cluster annotated to PTSD-relevant endocrine networks significantly enriched by DMGs in the training set. (d) Network cluster annotated to nervous system development networks significantly enriched by DMGs in the training set. In all the figure, red and green circles are hypermethylated and hypomethylated genes, respectively. Sizes of the circles labeled by the annotation terms are correlated with their significance of enrichment.DMG, differently methylated gene; PTSD, post-traumatic stress disorder.
Test set validated all the networks identified by the training set
There was a significant (P<0.001) overlap at the DMG level between the 48 PTSD+/51 PTSD− training set and the 31 PTSD+/29 PTSD− test set with 779 DMGs in common between the two sets assayed by the Agilent whole-genome array. Furthermore, a significant agreement was noted at the functional level as all of the networks mined from the training set emerged significantly enriched by DMGs identified from the test set (Table 1).
Union set probed by a different array platform validated a majority of networks identified by the training and test sets
The union set probed by the Illumina array resulted in 3339 DMG, 74.4% of which encoded hypermethylated CpGIs (Supplementary Figures S4B and C). One hundred ninety-one DMGs were in common between the training set and union set, and 107 DMGs were in common between the test set and union set (Supplementary Figure S5). There were 852 DMGs encoding promoter-bound CpGIs enriched in networks linked to addiction, long-term impact on cerebral functions, social withdrawal, diabetes, aging, inflammation, circadian rhythm, dopamine-serotonin signaling, neurogenesis, cannabinoid signaling, nerve impulse and synaptic plasticity. In addition, 407 DMGs in shelf and shore regions were enriched in networks associated with REM sleep, circadian rhythm, inflammation, hypothalamic–pituitary–adrenal axis and axon guidance. Altogether, the union set confirmed 15 out of 23 networks mined from the training set and validated by test set. All of the networks clustered under PTSD-associated somatic complications and nervous systems' development were confirmed by the training, test and union sets.
Methylation status of selected DMGs validated by targeted bisulfite sequencing
Forty-two DMGs were selected from the training set based on their methylation status and their relevance to PTSD. Their methylation status was verified by targeted bisulfite sequencing (Zymo Research, Irvine, CA, USA; Table 2).23, 24 Twenty genes out of forty-two DMGs were confirmed with the Agilent array data. Table 2 lists these genes and their relevance to PTSD and associated comorbidities.
Discussion
Clinical measures were in agreement with the epigenetically altered networks and DMGs
Self-reported clinical measures indicated that veterans with PTSD were concurrently experiencing higher levels of fear, social withdrawal, anxiety, hostility, depression and anger than were controls. Epigenetic investigation of DNA extracted from whole blood revealed networks relevant to these PTSD-associated negative emotions. Greater waist size, waist-to-hip ratio and body mass index19 were found in PTSD cases as compared with controls and are consistent with the observed pathways associated with cardiac diseases, diabetes and metabolic syndrome. PTSD-associated immune dysregulation has been previously reported in epigenetic studies.14, 15, 19 Consistent with previous findings,14 our results found a host of innate immunity-associated genes, consisting of 60% of the entire set of DMGs found altered in PTSD patients. In extending this knowledge, we functionally linked a majority of these genes to mobilization of phagocytic macrophages and leukocytes.
In addition, we identified epigenetically altered networks linked to learning and memory that are relevant for PTSD-associated neurocognitive impairment. Previous epidemiology studies suggested that there was an increased risk of premature aging in PTSD.34, 35, 36 We identified two epigenetically altered networks relevant to aging. The first network is telomere management and interaction with pathways of two mediators, wnt/β-catenin37 and p53.38 The epigenetic profile of these aging markers35 was altered in PTSD. The second network is mitochondrial dysfunction, also epigenetically altered in PTSD veterans. Consistent with these markers of premature aging, we found evidence recently for decreased mitochondrial DNA copy numbers in PTSD veterans from this cohort, suggesting a role for energy deprivation in PTSD that escalates the aging process.39
Premature aging40, 41 and other PTSD-associated somatic complications, such as dysregulation of immunity,42 are known to be associated with circadian rhythm. Veterans with PTSD showed epigenetic regulation of some of the key molecular nodes responsible for setting the circadian clock. We identified DMGs encoding CREB3 and GRIN2A, which control photoreception,43 and that are involved in signaling to entrain the circadian clock regulation by CLOCK and PER1 genes.44
Epigenetic changes in neurogenic functional pathways were captured by the differential methylation of members of the neural helix–loop–helix family, including NEUROG1 and HES1 and their regulators ATOH-1, Pax6 and NKX2-2.45, 46 Epigenetic perturbations of networks related to the hypothalamic–pituitary–adrenal axis functions and the synthesis of key feedback regulators, such as corticotrophin and glucocorticoid, as well as epigenetic changes in the serotonergic and dopaminergic networks, may serve as targets for novel therapeutics for PTSD.47
Strengths, limitations and future work
The Diagnostic and Statistical Manual of Mental Disorders-IV diagnostic criteria48 were used to determine the PTSD status, an approach to clinical phenotyping, which has limitations. We attempted to maximize signal detection by employing stringent selection criteria including a requirement of Clinician-Administered PTSD scale scores of 40 or greater for PTSD cases and scores less than 20 for controls.19, 20 Our array-based approach selected two platforms that ensured extensive coverage of the genome and instilled higher confidence in the outcome. We also focused primarily on the promoter regions, as the methylation shifts near transcription start site are most likely to be associated with long-term gene silencing.49
Given the biological heterogeneity of PTSD, our findings are limited by the sizes of our discovery, test and union sets.50 The selection of the Illumina platform was driven by the following three factors: (i) this platform offered nearly twice the number of CpGIs to test in comparison to the Agilent platform; (ii) the significantly lower amount of input DNA required for the Illumina assay (500 ng DNA versus 5 μg for the Agilent, assay) satisfied our need to conserve gradually decreasing DNA stocks; and (iii) the growing preference for the Illumina assay in the epigenetics literature11, 51 was convincing for its selection. The present study recruited the largest cohort size used to date to study the PTSD pathophysiology. The statistical analysis has moderate statistical power attributed to the sample size, which was further enhanced by the strict regulations applied by the pathway enrichment analysis. The epigenetic contributions of many of those genes discovered have been reported as linked to PTSD via transcriptomic variations. In addition, many novel epigenetic markers linked to PTSD were presented here. Together, this study revealed some of the key aspects of PTSD, such as its long-term health implications, which could be best explained by the epigenetic model. However, it is challenging to draw robust mechanistic conclusions due to the non-longitudinal nature of the study; hence, there is a limited scope for making inferences about whether these epigenetic alterations are causes of or consequences of PTSD. This study is also lacking in prospective design, gender balance and systems-wide integration. The findings are compromised further by the fact that the array platforms are potentially unable to provide the extensive coverage typical of deep sequencing.
On the basis of these findings, future work should focus on those epigenetically altered networks presented herein, which showed clinical relevance to PTSD pathophysiology. Our study presented a knowledge-driven data-mining architecture particularly useful to identify potential biomarkers for a multifactorial disease such as PTSD. In particular, we demonstrated how to use the clinical and physical dimensions as the successful guiding cue to mine the molecular markers linked to disease pathophysiology. This data-mining approach will be practised further in our future study that will recruit a new validation set to confirm the results obtained from the union set serving as the better-powered discovery set. We will also recruit a cohort of female veterans to minimize gender bias. Additional data from blood counts and magnetic resonance imaging will be included. System-wide knowledge integration will be performed to identify PTSD biomarkers with the highest efficacy.52, 53, 54, 55, 56
References
Uher R, Weaver IC . Epigenetic traces of childhood maltreatment in peripheral blood: a new strategy to explore gene-environment interactions. Br J Psychiatry 2014; 204: 3–5.
Tammen SA, Friso S, Choi SW . Epigenetics: the link between nature and nurture. Mol Aspects Med 2013; 34: 753–764.
Feil R, Fraga MF . Epigenetics and the environment: emerging patterns and implications. Nat Rev Genet 2011; 13: 97–109.
Chakraborty N, Meyerhoffa J, Gautama A, Muhiea S, Jibitua M, De Limab TCM et al. Gene and stress history interplay in emergence of PTSD-like features. Behav Brain Res 2015; 292: 266–277.
Spiegel D . An ingeneious study of intergenerational transmission of the effects of PTSD. Am J Psychiatry 2014; 171: 811–813.
Stein MB, Jang KL, Taylor S, Vernon PA, Livesley WJ . Genetic and environmental influences on trauma exposure and posttraumatic stress disorder symptoms: a twin study. Am J Psychiatry 2002; 159: 1675–1681.
Yehuda R, Flory JD, Bierer LM, Henn-Haase C, Lehrner A, Desarnaud F et al. Lower methylation of glucocorticoid receptor gene promoter 1F in peripheral blood of veterans with posttraumatic stress disorder. Biol Psychiatry 2015; 77: 356–364.
Yehuda R, Daskalakis NP, Lehrner A, Desarnaud F, Bader HN, Makotkine I et al. Influences of maternal and paternal PTSD on epigenetic regulation of the glucocorticoid receptor gene in Holocaust survivor offspring. Am J Psychiatry 2014; 171: 872–880.
Zovkic IB, Sweatt JD . Epigenetic mechanisms in learned fear: implications for PTSD. Neuropsychopharmacology 2013; 38: 77–93.
Pizzimenti CL, Lattal KM . Epigenetics and memory: causes, consequences and treatments for post-traumatic stress disorder and addiction. Genes Brain Behav 2015; 14: 73–84.
Norrholm SD, Jovanovic T, Smith AK, Binder E, Klengel T, Conneely K et al. Differential genetic and epigenetic regulation of catechol-O-methyltransferase is associated with impaired fear inhibition in posttraumatic stress disorder. Front Behav Neurosci 2013; 7: 30.
Uddin M, Galea S, Chang SC, Koenen KC, Goldmann E, Wildman DE et al. Epigenetic signatures may explain the relationship between socioeconomic position and risk of mental illness: preliminary findings from an urban community-based sample. Biodemogr Soc Biol 2013; 59: 68–84.
Rusiecki JA, Chen L, Srikantan V, Zhang L, Yan L, Polin ML et al. DNA methylation in repetitive elements and post-traumatic stress disorder: a case-control study of US military service members. Epigenomics 2012; 4: 29–40.
Breen MS, Maihofer AX, Glatt SJ, Tylee DS, Chandler SD, Tsuang MT et al. Gene networks specific for innate immunity define post-traumatic stress disorder. Mol Psychiatry 2015; 20: 1538–1545.
Uddin M, Aiello AE, Wildman DE, Koenen KC, Pawelec G, de Los Santos R et al. Epigenetic and immune function profiles associated with posttraumatic stress disorder. Proc Natl Acad Sci USA 2010; 107: 9470–9475.
Rusiecki JA, Byrne C, Galdzicki Z, Srikantan V, Chen L, Poulin M et al. PTSD and DNA methylation in select immune function gene promoter regions: a repeated measures case-control study of U.S. military service members. Front Psychiatry 2013; 4: 56.
Vukojevic V, Kolassa IT, Fastenrath M, Gschwind L, Spalek K, Milnik A et al. Epigenetic modification of the glucocorticoid receptor gene is linked to traumatic memory and post-traumatic stress disorder risk in genocide survivors. J Neurosci 2014; 34: 10274–10284.
Labonte B, Azoulay N, Yerko V, Turecki G, Brunet A . Epigenetic modulation of glucocorticoid receptors in posttraumatic stress disorder. Transl Psychiatry 2014; 4: e368.
Lindqvist D, Wolkowitz OM, Mellon S, Yehuda R, Flory JD, Henn-Haase C et al. Proinflammatory milieu in combat-related PTSD is independent of depression and early life stress. Brain Behav Immun 2014; 42: 81–88.
Yan X, Brown AD, Lazar M, Cressman VL, Henn-Haase C, Neylan TC et al. Spontaneous brain activity in combat related PTSD. Neurosci Lett 2013; 547: 1–5.
Leek JT, Scharpf RB, Bravo HC, Simcha D, Langmead B, Johnson WE et al. Tackling the widespread and critical impact of batch effects in high-throughput data. Nat Rev Genet 2010; 11: 733–739.
Houseman EA, Accomando WP, Koestler DC, Christensen BC, Marsit CJ, Nelson HH et al. DNA methylation arrays as surrogate measures of cell mixture distribution. BMC Bioinformatics 2012; 13: 86.
Wilmot B, Fry R, Smeester L, Musser ED, Mill J, Nigg JT . Methylomic analysis of salivary DNA in childhood ADHD identifies altered DNA methylation in VIPR2. J Child Psychol Psychiatr 2016; 57: 152–160.
Ashktorab H, Daremipouran M, Goel A, Varma S, Leavitt R, Sun X et al. DNA methylome profiling identifies novel methylated genes in African American patients with colorectal neoplasia. Epigenetics 2014; 9: 503–512.
Krishnan V, Han MH, Mazei-Robison M, Iniguez SD, Ables JL, Vialou V et al. AKT signaling within the ventral tegmental area regulates cellular and behavioral responses to stressful stimuli. Biol Psychiatry 2008; 64: 691–700.
Dahlhoff M, Siegmund A, Golub Y, Wolf E, Holsboer F, Wotjak CT . AKT/GSK-3beta/beta-catenin signalling within hippocampus and amygdala reflects genetically determined differences in posttraumatic stress disorder like symptoms. Neuroscience 2010; 169: 1216–1226.
Martinotti G, Sepede G, Brunetti M, Ricci V, Gambi F, Chillemi E et al. BDNF concentration and impulsiveness level in post-traumatic stress disorder. Psychiatr Res 2015; 229: 814–818.
Dell'Osso L, Carmassi C, Del Debbio A, Catena Dell'Osso M, Bianchi C, da Pozzo E et al. Brain-derived neurotrophic factor plasma levels in patients suffering from post-traumatic stress disorder. Prog Neuropsychopharmacol Biol Psychiatry 2009; 33: 899–902.
Su S, Xiao Z, Lin Z, Qiu Y, Jin Y, Wang Z . Plasma brain-derived neurotrophic factor levels in patients suffering from post-traumatic stress disorder. Psychiatr Res 2015; 229: 365–369.
Lu AT, Ogdie MN, Jarvelin MR, Moilanen IK, Loo SK, McCracken JT et al. Association of the cannabinoid receptor gene (CNR1) with ADHD and post-traumatic stress disorder. Am J Med Genet B Neuropsychiatr Genet 2008; 147B: 1488–1494.
O'Donovan A, Sun B, Cole S, Rempel H, Lenoci M, Pulliam L et al. Transcriptional control of monocyte gene expression in post-traumatic stress disorder. Dis Markers 2011; 30: 123–132.
Rameil P, Lecine P, Ghysdael J, Gouilleux F, Kahn-Perles B, Imbert J . IL-2 and long-term T cell activation induce physical and functional interaction between STAT5 and ETS transcription factors in human T cells. Oncogene 2000; 19: 2086–2097.
Young KA, Berry ML, Mahaffey CL, Saionz JR, Hawes NL, Chang B et al. Fierce: a new mouse deletion of Nr2e1; violent behaviour and ocular abnormalities are background-dependent. Behav Brain Res 2002; 132: 145–158.
Zhang L, Hu XZ, Li X, Li H, Smerin S, Russell D et al. Telomere length - a cellular aging marker for depression and post-traumatic stress disorder. Med Hypotheses 2014; 83: 182–185.
Boks MP, van Mierlo HC, Rutten BP, Radstake TR, De Witte L, Geuze E et al. Longitudinal changes of telomere length and epigenetic age related to traumatic stress and post-traumatic stress disorder. Psychoneuroendocrinology 2015; 51: 506–512.
Lohr JB, Palmer BW, Eidt CA, Aailaboyina S, Mausbach BT, Wolkowitz OM et al. Is post-traumatic stress disorder associated with premature senescence? A review of the literature. Am J Geriatr Psychiatry 2015; 23: 709–725.
Zhang DY, Wang HJ, Tan YZ . Wnt/beta-catenin signaling induces the aging of mesenchymal stem cells through the DNA damage response and the p53/p21 pathway. PLoS ONE 2011; 6: e21397.
Artandi SE, Attardi LD . Pathways connecting telomeres and p53 in senescence, apoptosis, and cancer. Biochem Biophys Res Commun 2005; 331: 881–890.
Bersani FS, Morley C, Lindqvist D, Epel ES, Picard M, Yehuda R . Mitochondrial DNA copy number is reduced inmale combat veterans with PTSD. Progr Neuro-Psychopharmacol Biol Psychiatry 2015; 64: 17.
Kondratov RV, Kondratova AA, Gorbacheva VY, Vykhovanets OV, Antoch MP . Early aging and age-related pathologies in mice deficient in BMAL1, the core componentof the circadian clock. Genes Dev 2006; 20: 1868–1873.
Monk TH . Aging human circadian rhythms: conventional wisdom may not always be right. J Biol Rhythms 2005; 20: 366–374.
Scheiermann C, Kunisaki Y, Frenette PS . Circadian control of the immune system. Nat Rev Immunol 2013; 13: 190–198.
Travnickova-Bendova Z, Cermakian N, Reppert SM, Sassone-Corsi P . Bimodal regulation of mPeriod promoters by CREB-dependent signaling and CLOCK/BMAL1 activity. Proc Natl Acad Sci USA 2002; 99: 7728–7733.
Ko CH, Takahashi JS . Molecular components of the mammalian circadian clock. Hum Mol Genet 2006; 15 (Spec No 2): R271–R277.
Sugimori M, Nagao M, Bertrand N, Parras CM, Guillemot F, Nakafuku M . Combinatorial actions of patterning and HLH transcription factors in the spatiotemporal control of neurogenesis and gliogenesis in the developing spinal cord. Development 2007; 134: 1617–1629.
Mulvaney J, Dabdoub A . Atoh1, an essential transcription factor in neurogenesis and intestinal and inner ear development: function, regulation, and context dependency. J Assoc Res Otolaryngol 2012; 13: 281–293.
Asnis GM, Kohn SR, Henderson M, Brown NL . SSRIs versus non-SSRIs in post-traumatic stress disorder: an update with recommendations. Drugs 2004; 64: 383–404.
Association AP Diagnostic Criteria from DSM-IV. The Association: Washington, DC, 1994.
Jones PA . Functions of DNA methylation: islands, start sites, gene bodies and beyond. Nat Rev Genet 2012; 13: 484–492.
Shao L, Fan X, Cheng N, Wu L, Cheng Y . Determination of minimum training sample size for microarray-based cancer outcome prediction-an empirical assessment. PLoS ONE 2013; 8: e68579.
Mehta D, Klengel T, Conneely KN, Smith AK, Altmann A, Pace TW et al. Childhood maltreatment is associated with distinct genomic and epigenetic profiles in posttraumatic stress disorder. Proc Natl Acad Sci USA 2013; 110: 8302–8307.
Gates MA, Holowka DW, Vasterling JJ, Keane TM, Marx BP, Rosen RC . Posttraumatic stress disorder in veterans and military personnel: epidemiology, screening, and case recognition. Psychol Services 2012; 9: 361–382.
Hayes JP, Vanelzakker MB, Shin LM . Emotion and cognition interactions in PTSD: a review of neurocognitive and neuroimaging studies. Front Integr Neurosci 2012; 6: 89.
Solomon Z, Helvitz H, Zerach G . Subjective age, PTSD and physical health among war veterans. Aging Ment Health 2009; 13: 405–413.
Mehta D, Binder EB . Gene x environment vulnerability factors for PTSD: the HPA-axis. Neuropharmacology 2012; 62: 654–662.
McDonald SD, Calhoun PS . The diagnostic accuracy of the PTSD checklist: a critical review. Clin Psychol Rev 2010; 30: 976–987.
Thakur Gunjan S, Daigle Jr Bernie J, Dean Kelsey R, Zhang Yuanyang, Rodriguez-Fernandez Maria, Hammamieh Rasha, Yang Ruoting, Jett Marti, Palma Joseph, Petzold Linda R, Doyle III Francis J . Systems biology approach to understanding post-traumatic stress disorder. Mol. BioSyst 2015; 11 (4): 980–993. 10.1039/C4MB00404C.
Acknowledgements
The project is supported by the USAMRMC Military Operational Medicine Research Program (MOMRP)/Defense Health Agency (DHA)/Congressional Special Interests (CSI) and MOMRP 190040.
Disclaimer
The views, opinions and/or findings contained in this report are those of the authors and should not be construed as an official Department of the Army position, policy or decision, unless so designated by other official documentation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Translational Psychiatry website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Hammamieh, R., Chakraborty, N., Gautam, A. et al. Whole-genome DNA methylation status associated with clinical PTSD measures of OIF/OEF veterans. Transl Psychiatry 7, e1169 (2017). https://doi.org/10.1038/tp.2017.129
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2017.129
This article is cited by
-
Prominent genetic variants and epigenetic changes in post-traumatic stress disorder among combat veterans
Molecular Biology Reports (2024)
-
Circulating cell-free mitochondrial DNA levels and glucocorticoid sensitivity in a cohort of male veterans with and without combat-related PTSD
Translational Psychiatry (2024)
-
Psychological and biological mechanisms linking trauma with cardiovascular disease risk
Translational Psychiatry (2023)
-
Epigenome-wide association study of posttraumatic stress disorder identifies novel loci in U.S. military veterans
Translational Psychiatry (2022)
-
Genome-wide differentially methylated genes associated with posttraumatic stress disorder and longitudinal change in methylation in rape survivors
Translational Psychiatry (2021)
