
Abstract
Behavioral inhibition (BI) is an important early childhood marker of risk for later psychiatric problems. The current 20-year prospective, longitudinal study focused on individual differences in this early temperament and adolescent brain function. As adolescents, 83 participants initially identified in infancy with the temperament of BI were assessed using functional imaging to examine striatal responses to incentives. Five years later, as young adults, these participants provided self-report of their substance use. Our findings show that children’s early temperament interacts with their striatal sensitivity to incentives in adolescence to predict their level of substance use in young adulthood. Those young adults who, as children, showed the highest levels of BI reported the greatest substance use if, as adolescents, they also exhibited striatal hypersensitivity to incentives. These longitudinal data delineate one developmental pathway involving early biology and brain mechanisms for substance use in young adulthood.
Similar content being viewed by others


Introduction
Behavioral inhibition (BI) is a well-studied early childhood temperament, which is an important marker of risk for later psychiatric problems.1, 2 Young children identified during infancy with this temperament show fearful responses to novelty, heightened negative affect, and in early childhood display heightened social reticence to unfamiliar peers.3, 4, 5, 6 Furthermore, individuals characterized by BI are at increased risk for psychopathology, particularly anxiety.7
Recent neuroimaging studies report that adolescents with a history of childhood BI,8, 9, 10 as well as adolescents with social anxiety,11 show striatal hyper-activation not only in response negative monetary incentive cues, but also to positive incentive cues. This hypersensitivity, found across studies, suggests that BI involves perturbed activation in the striatum. This brain region is linked to motivated behavior,12 risk-taking, and substance use,13 and these findings resonate with data on abnormal striatum recruitment by non-drug incentives.14 Indeed, although BI individuals are sensitive to threat,3, 4, 5, 6 research suggests that BI individuals may be also more vulnerable to later substance use compared with typical peers.1, 15, 16
Substance use disorders impart considerable suffering, impairment and health-care costs, affecting physical and mental health, as well as school and job performance. Because predisposing factors can be traced back to childhood, early identification of risk phenotypes is a public health priority.17, 18 Substance use emerges in adolescence and tends to peak in young adulthood,19 when changes in social contexts, such as unstructured socializing, present new opportunities for experimentation and risky behaviors.20, 21 Considerable work in this area focuses on children with disruptive behavior as an early-emerging risk factor.22, 23 Yet, other individuals also face risk for substance use. In particular, anxious adolescents and young adults may turn to alcohol and illicit substances to cope with increasing stress from the new, challenging social environments of young adulthood.24
Complex interactions among factors identified early in life and those that arise later are thought to ultimately predict outcome. Indeed, prior research on temperament suggests that risk for negative outcomes and psychiatric problems is found primarily among BI children who also manifest unique electrophysiological and behavioral response profiles, related to attention and threat monitoring.25, 26, 27, 28, 29 However, these prior studies mainly considered prediction of anxiety; no such prospective research has charted the ways in which early-life brain and behavioral measures predict substance use patterns over time. Advances in neuroscience, and neuroimaging in particular, highlight notable progress that has improved our understanding of the neurobiology of substance use and risk factors related to it.30 Although research on anxiety implicates attention and associated amygdala–frontal dysfunction, research on substance use implicates the striatum. The present study examines how adolescent striatal hypersensitivity to incentives moderates the relation between early childhood BI and young adult substance use. To our knowledge, this is the first prospective longitudinal study to examine the interaction between early childhood temperament and adolescent brain function, as these two factors are independently associated with individual differences in substance use.
Approximately 10 years after being characterized with the temperament of BI in early childhood, adolescents completed the monetary incentive delay (MID) task,12 while undergoing functional magnetic resonance imaging (fMRI). About 5 years after this neuroimaging experiment, participants completed self-report measures of substance use. This longitudinal design allowed us to examine whether substance use could be predicted from a life-course perspective involving the combined influence of temperament in early childhood and brain function in adolescence. Our a priori hypothesis was that striatal activation to monetary incentives would moderate the relation between early childhood BI and adult substance use, such that BI would be positively related to substance use among individuals displaying high striatal activation to incentives. This hypothesis is consistent with other work on BI and risk for psychiatric problems, such as anxiety, where biological indices related to anxiety have been shown to moderate outcome.25, 28, 29
Participants and methods
Participants and procedures
Participants were drawn from two cohorts participating in a longitudinal study of temperament. At the study’s inception, 443 infants were screened at 4 months of age to assess their reactivity to novel auditory and visual stimuli. Videotapes of the screening procedure were coded for positive and negative affect and motor activity during the presentation of novel stimuli. A complete description of the stimuli, coding procedures and inter-rater reliability is presented elsewhere.4, 5, 6 One hundred seventy-eight (86 male), primarily white infants from two parent, middle-class homes were selected to provide a wide range of temperamental reactivity to novelty measures. Specifically, 37% of the selected infants showed high negative/high motor reactivity, 29% showed high positive/high motor reactivity, and 34% showed low reactivity. These infants were followed across childhood and adolescence and into young adulthood as part of the larger longitudinal study.
Following the initial 4-month assessment participants were observed in the laboratory at 14 months, 24 months, 4 years and 7 years of age. Of the original selected sample, 159 mothers of child participants (81 male) completed a temperament questionnaire during at least one of the assessment points across infancy and childhood (n=139 at 14 months; n=133 at 24 months; n=133 at 4 years; and n=116 at 7 years). Those with temperament data at any time point were not significantly different by sex (all P values >0.07).
During adolescence, a total of 91 participants completed the MID task12 while undergoing fMRI. Participants were excluded because of medication use during the time of scan (n=4), motion >3 mm (n=2) or technical difficulties (n=2). As a result 83 participants (39 male, M age=16.33, s.d.=2.79, Range: 10.74–21.00) had useable fMRI data. During young adulthood, 93 participants (40 male, M age=19.85, s.d.=0.97, Range: 18.10–21.18) completed substance use measures, including the customary drinking/drug use record (CDDR31), youth risk behavior surveillance (YRBS32), and Brief Young Adult Alcohol Consequences Questionnaire (B-YAACQ33). A total of 65 (30 male) participants with available fMRI and substance use data were included in the main analyses.
Temperament assessment
At 14 and 24 months of age infants were assessed in the laboratory and were presented with novel and unfamiliar objects and people.5 Furthermore, maternal ratings of social fear were collected at these ages with the Toddler Behavior Assessment Questionnaire.34 At ages 4 and 7 years, children’s reticent behavior with unfamiliar peers was measured using Rubin’s Play Observation Scale.35 In addition, mothers rated shyness at these ages with the Colorado Child Temperament Inventory.36 To create a BI composite measure, behavioral, and maternal report scores across the four testing waves were taken from the entire cohort (regardless of participation at adolescence or adulthood) and standardized. Z-scores were then averaged to create the composite measure of BI.
MID task
The MID task12 included two runs of 56 contiguous 6 s trials, for 112 trials total. At the beginning of each trial a cue was presented for 250 ms. This was followed by a crosshair fixation delay of 2000-2500 ms. Subsequently, a target stimulus was presented for 160–260 ms. This was followed by feedback information (1650 ms). Three types of cues informed the incentive condition: circle cues (n=48) indicated a potential monetary gain, square cues (n=48) indicated a potential monetary loss, and triangle cues (n=16) indicated the absence of incentive. Information on magnitude level of the incentive value was also carried by the incentive cues in the form of lines within the circle or rectangle: single line for small incentive ($0.20; n=32), two lines for medium incentive ($1; n=32) or three lines for high incentive ($5; n=32). Participants were asked to press a button as quickly as possible in response to the target stimulus in order to either gain the anticipated reward or avoid the potential loss. After the target disappeared, participants were notified of both their current and cumulative dollar amount. The order of trial type was random within each run. Participants were told that they would receive a percentage of the dollar amount won. Participants completed a practice MID task in the scanner, providing an estimate of their reaction time. Task difficulty was standardized to a ∼66% success rate by adjusting target duration (five difficulty levels). This approach minimized the potential confound of large performance differences across participants.
fMRI acquisition
Scanning occurred in a Signa 3T scanner (General Electric, Waukesha, WI) for the first 68 participants. For the final 15 participants, scanning occurred in a GE 3T Excite HDX scanner. Both groups used the same GE head coil. The two scanning groups did not differ on the major demographic or research factors (all Ps >0.13), other than age at time of scanning (P<0.0001) and substance use (P<0.05). Thus, in order to account for any potential impacts of scanner differences we included scanner type as a covariate in our main analysis.
A Cedrus Lumina response box (Psychological Software Tools, San Pedro, CA) recorded behavioral data. Task stimuli were projected onto a screen at the foot of the scanner bed and viewed with mirrors mounted on the head coil. Foam padding constrained head movement.
Each brain volume consisted of 30 interleaved slices, 4 mm thick, acquired in the sagittal plane using a T2*-weighted echo-planar sequence with a repetition time of 2500 ms, echo time of 23 ms, and flip angle of 90°. Voxel dimension was 3.75 × 3.75 × 4.0 mm. Matrix size was 64 × 64, and field of view was 24 cm. To allow for signal stabilization, four acquisitions were obtained before task onset. A high-resolution structural image was also acquired for each subject using a T1-weighted standardized magnetization-prepared spoiled gradient-recalled echo sequence: 1241 mm slices, 8100 ms repetition time, 32 ms echo time, 15° flip angle, 256 × 256 matrix and 24 cm field of view.
fMRI data analysis
Analysis of Functional NeuroImages (AFNI) software was used for the analyses.37 Error trials were removed from processing. Standard preprocessing of echo-planar data included slice time correction, motion correction and spatial smoothing with a 6 mm full-width half-maximum smoothing kernel. Signal deviations >2.5 s.d. from the mean were removed using an AFNI despiking algorithm applied on a voxel-wise basis and a bandpass filtering algorithm to remove cyclical fluctuations in signal (either >0.01 or <0.15 Hz) not temporally indicative of a hemodynamic response. We then normalized blood oxygen level dependent (BOLD) signal intensity to percentage signal change using each subject’s voxel-wise time series mean as a baseline.
Preprocessed time series data for each individual were analyzed by multiple regression.38 The regression model included 32 regressors, including both cues and feedback. Of these, there were eight regressors: six regressors modeling effects attributable to residual motion (using the motion correction factors in the x, y and z planes and in the yaw, pitch and roll dimensions), and two regressors modeling baseline and linear trends for each of the two runs. Regressors of interest included cues signaling trial type (for example, potential gains and losses) and were convolved with a gamma variate function that modeled a prototypical hemodynamic response.39 Idealized signal time courses were estimated based on onset time of different event types during the task.
Contrasts of BOLD activation were created for each subject for cues signaling incentive magnitude of (1) large $ gain/loss versus no $, (2) medium $ gain/loss versus no $, and (3) small gain/loss $ versus no $. Our main analysis targeted the interaction between BI and striatal activation in predicting substance use. Therefore, we used a region of interest (ROI) approach focused on the caudate, putamen and nucleus accumbens. ROIs were defined by anatomical boundaries provided by AFNI after spatial normalization,40 in line with previous work with this task.8 Specifically, we extracted values from the ROIs to reflect the moderation of striatal activation in the association between BI and substance use. In this way we hoped to minimize potential biases in the analysis of the imaging data.41
One contrast value was generated per subject for each ROI. This approach was used to balance Type 1 errors associated with multi-voxel testing, which might accrue from multiple testing of specific brain regions or specific event types, with Type 2 errors associated with overly stringent statistical thresholds in between-subject imaging research.42 Moreover, this approach also is consistent with prior findings for the MID task.8 The individual contrast values were extracted from each anatomical ROI. Given that we were interested in the role of striatal activation to both positive and negative incentives in predicting substance use, we made an a priori decision to average across region (nucleus accumbens, caudate, putamen), incentive (gain, loss) and magnitude of incentive (small, medium, large) as well as across laterality (right, left). This generated a single striatal activation composite variable for each subject. With this approach, one index of striatal hypersentivity could serve as a moderator in the relation between BI and substance use. This approach also allowed us to test our hypothesis in one regression model. However, preliminary analyses using non-averaged variables indicated a similar pattern of results.
Substance use composite
During young adulthood, participants responded to self-report measures of substance use. First, participants completed the CDDR,31 a structured interview that assesses recent and lifetime alcohol, drug and tobacco involvement in four domains: consumption, withdrawal characteristics, psychological/behavioral dependence and consequences. The CDDR has been found to have high reliability and validity for each domain for both abusing and community samples.31 These include internal consistency (α=0.68–0.94), test–retest reliability (r=0.86 to 0.93) and inter-rater reliability (99% agreement). Validity scores include convergent validity (r=0.24–0.79), discriminant validity (distinguish substance abusing from non-abusing adolescents Ps >0.01) and criterion validity (k=0.51–0.84). Scoring of the CDDR included calculating whether participants ever used a substance (88% used alcohol, 53% used drugs), age of regular substance use (alcohol M=17.23, s.d.=1.51), age of onset for each substance (alcohol M=15.87, s.d.=2.47, drugs M=16.27, s.d.=1.92), heavy drinking (M=1.85 drinks per episode, s.d.=1.43), as well as time taken to achieve regular smoking (years taken to increase to weekly smoking M=1.41, s.d.=1.53; years taken to increase to daily smoking M=1.56, s.d.=1.36). Each of these scores was then standardized.
Second, participants completed items from the YRBS.32 Items chosen from the larger YRBS assessed risk behaviors, including unsafe driving, aggression, tobacco use, alcohol consumption, drug use and risky sexual behavior. Test–retest reliability has been carried out for each item with kappas ranging from 23.6 to 90.5%, with a mean of 60.7%.32 Data were scored according to standard YRBS procedures. Items with <10% endorsement of behavior were not analyzed. Items that were scored included questions pertaining to alcohol consumption, drug use and risky sexual behavior. Although many questions contain multiple response categories, standard YRBS reports dichotomize responses into ‘no risk’ versus ‘at risk.’ These dichotomized scores were then included in a principal components factor analysis carried out separately for each type of behavior. This analysis confirmed four factors that were saved as variables: alcohol consumption (loadings >0.67), drug use (loadings >0.74), risky sexual behavior (loadings >0.45) and substance-use-related sexual behavior (loadings >0.70).
Finally, participants completed the B-YAACQ,33 a 24-item measure that asses alcohol-related consequences. Dichotomous items (yes/no) were summed for a total number of alcohol-related consequences experienced in the past year. This measure has demonstrated high internal consistency in previous research with college students (α=0.89).33 A sum total score was calculated (M=4.92, s.d.=5.32) and standardized. Subsequently, the standardized scores of the B-YAACQ and CDDR, as well as the factors extracted from the YRBS, were averaged to create a substance use composite score.
Hierarchical regression analyses
As a preliminary step, a series of t-tests were used to examine sex-related differences on all predictor and outcome variables. Significant sex-related differences were found for BI, t(43.63)=2.22, P<0.03 with males (M=0.21, s.d.=0.90) displaying greater BI than females (M=−0.20, s.d.=0.50). No other significant differences were found, all Ps>0.37. Thus, sex was included as a covariate in the hierarchical regression analysis. Next, Pearson inter-correlations were carried out between predictor and outcome variables. A correlation between striatal activation and substance use was found at a trend level, P<0.08. No other significant correlations were found, all Ps>0.62.
Although we did not find a correlation between the predictor variables (that is, BI and striatal activation),43 we examined our a priori hypothesis regarding the potential moderating role of striatal activation in the relation between BI and substance use. We conducted a hierarchical multiple regression analysis using the BI and striatal activation composites as continuous predictors and the substance use composite as an outcome. To reduce multicollinearity and aid in interpretation, mean-centered predictors were used. Next, the interaction term was computed as the product between the BI composite measure and striatal activation. Age at scan time, sex and scanner type were entered as covariates in the first step of the regression analysis. BI and striatal activation were also entered in the first step of the regression analysis as main effects. To test for significant moderation effects of striatal activation on the link between BI and substance use, the interaction product term between BI and striatal activation was entered in the second step of the regression analysis. Although the entire regression model was examined for significance, to test the moderation hypothesis, we examined whether the second step of the model significantly increased the variance explained by the model. Interactions were probed and plotted according to the guidelines by Aiken and West.44 High and low levels of BI and striatal activation were computed as ±1 s.d.
Results
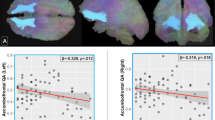
Means and s.d. of predictor (BI and striatal activation) and outcome (substance use) variables are presented in Table 1. We conducted a hierarchical multiple regression analysis with BI and a composite measure representing striatal activation during the MID task (Figure 1) as predictor variables. BI was a continuous composite score, which was comprised of behavioral and maternal report assessments conducted at 14 months, 24 months, 4 years and 7 years of age. In this analysis, a substance use composite was regressed on these predictors, with the key hypothesis testing the BI-by-brain function interaction. This interaction significantly improved the model, ΔR2=0.08, F(1,64)=6.03, P<0.017. The full model with the interaction term was significant F(6, 64)=2.26, P<0.05, f2=0.23, with a medium-to-large effect,45 predicting 19% of the variance in adult substance use (Table 2 and Figure 2). To decompose this interaction, follow-up regressions were conducted. The findings indicate that within participants who exhibited high striatal activation, BI was positively related to substance use, β=0.40, t(64)=2.19, P<0.03. However, when participants showed low striatal activation, BI was not related to substance use, β=−0.28, t(64)=−1.46, P=0.15. In addition, within participants with high BI, striatal activation was related to substance use, β=0.47, t(64)=2.85, P<0.01. However, within participants with low BI, striatal activation was not related to substance use, β=−0.16, t(64)=−0.84, P=0.41.

Striatal activation during the MID task averaged across incentives versus neutral.

Joint effect of BI and striatal activation on substance use.
Discussion
The present longitudinal study highlights the conditions under which a complex pattern of behavior, substance use, arises from bio-behavioral interactions that unfold in a developmental context. Early childhood BI interacted with adolescent striatal activation to predict substance use in young adults. Specifically, individuals who were behaviorally inhibited during early childhood and who exhibited high striatal activation in response to incentives as adolescents reported elevated substance use as young adults.
These data are consistent with research showing striatal hypersensitivity to incentives among BI individuals.8, 9, 10 Our findings are also in line with previous studies, suggesting a relation between BI and substance use.1, 15, 16 Our study extends this previous work by describing functional mechanisms that contribute to this developmental pathway.
During young adulthood, individuals often move away from the home environment and enter new social settings.46 An early-life tendency to display social reticence may render some individuals vulnerable to the use of substances to enhance their ability to socialize.47 Substance use may be viewed by these individuals as a means for social approach and ease the transition into novel social relationships.15 Our findings suggest that this may be particularly salient for behaviorally inhibited individuals with heightened sensitivity to motivational cues, as manifested in hyper-sensitive striatal responses to positive and negative incentives.
Our hierarchical regression used a composite variable representing activation to both positive and negative incentives in different structures within the striatum (nucleus accumbens, caudate and putamen). We found that this average measure of striatal activation moderated the relation between early childhood BI and substance use. This finding is in line with previous work showing that striatal activation is sensitive to positive and negative incentive cues, substance use and BI.8, 9, 10, 12, 48 Specifically, anticipation of increasing monetary reward has been found to selectively recruit nucleus accumbens,12 while the caudate and putamen seem to respond more generally to salient events.48 Furthermore, the results of the present study are in line with motivational accounts of substance use vulnerability, according to which individuals at risk for substance use show perturbations in striatal recruitment by cues predicting non-drug-related incentives.49
Although our findings indicate that striatal activation moderates the link between BI and substance use, our regression model did not reveal direct links between BI and substance use, nor between striatal activation and substance use. Previous studies have shown that the relation between BI and substance use is complex and involves moderating factors such as gender and risk-taking propensity.15 Both high1, 16 and low50 BI may place individuals at increased risk for substance use. Finally, prior research on adverse outcomes, such as anxiety, suggests that neurocognitive and neurophysiological factors moderate the relations between BI and outcome. This work shows that BI predicts risk primarily among youth with biological profiles that also are associated with risk.25, 26, 27, 28, 29 In the current study, this pattern of results emerged for striatal hyper-activity. Although the regression model did not reveal a significant relation between substance use and striatal activation, these variables were found to be related at a trend level in the present sample. This finding is in line with previous work on neural correlates associated with substance use.13, 51 More importantly, among individuals with relatively high levels of striatal activation, early childhood BI did predict substance use.
Although previous work8 has shown a significant difference between high and low BI individuals in striatal activation to incentives, we did not find a significant direct relation between BI and the striatal activation composite in the current study. This inconsistency may be a result of the larger variability of BI in the present sample, coupled with the complexity of associations between BI and reward function in prior studies. The lack of correlation in the present study, along with findings in prior studies, suggests that the relations between BI and striatal activation are complex. This is in line with previous studies,9, 10 suggesting that increased striatal activation involves interactions between BI and various task conditions, such as incentive valence.
Few phenotypes are as well characterized in early childhood as BI. Children with this temperament exhibit a unique pattern of physiological reactivity and behavioral response to novelty. These findings, using early childhood temperament and adolescent brain function, are the first to trace the conditions under which a complex, multi-determined adult behavior is developed.
References
Caspi A, Moffitt TE, Newman DL, Silva PA . Behavioral observations at age 3 years predict adult psychiatric disorders. Arch Gen Psychiatry 1996; 53: 1033–1039.
Lahat A, Hong M, Fox NA . Behavioral inhibition: is it a risk factor for anxiety? Int Rev Psychiatry 2011; 23: 248–257.
Kagan J, Snidman N . Infant predictors of inhibited and uninhibited profiles. Psych Sci 1991; 2: 40–44.
Fox NA, Henderson HA, Marshall PJ, Nichols KE, Ghera MM . Behavioral inhibition: linking biology and behavior within a developmental framework. Annu Rev Psychol 2005; 56: 235–262.
Calkins SD, Fox NA, Marshall TR . Behavioral and physiological antecedents of inhibited and uninhibited behavior. Child Dev 1996; 67: 523–540.
Fox NA, Henderson HA, Rubin KH, Calkins SD, Schmidt LA . Continuity and discontinuity of behavioral inhibition and exuberance: psychophysiological and behavioral influences across the first four years of life. Child Dev 2001; 72: 1–21.
Chronis-Tuscano A, Degnan KA, Pine DS, Perez-Edgar K, Henderson HA, Diaz Y et al. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J Am Acad Child Adolesc Psychiatry 2009; 48: 1–8.
Guyer AE, Nelson EE, Perez-Edgar K, Hardin MG, Roberson-Nay R, Monk CS et al. Striatal functional alteration in adolescents characterized by early childhood behavioral inhibition. J Neurosci 2006; 26: 6399–6405.
Bar-Haim Y, Fox NA, Benson B, Guyer AE, Williams A, Nelson EE et al. Neural correlates of reward processing in adolescents with a history of inhibited temperament. Psych Sci 2009; 20: 1009–1018.
Helfinstein SM, Benson B, Perez-Edgar K, Bar-Haim Y, Detloff A, Pine DS et al. Striatal responses to negative monetary outcomes differ between behaviorally inhibited and non-inhibited adolescents. Neuropsychologia 2011; 49: 479–485.
Guyer AE, Choate VR, Detloff A, Benson B, Nelson EE, Perez-Edgar K et al. Striatal functional alteration during incentive anticipation in pediatric anxiety disorders. Am J Psychiatry 2011; 169: 205–212.
Knutson B, Adams CM, Fong GW, Hommer D . Anticipation of increasing monetary reward selectively recruits nucleus accumbens. J Neurosci 2001; 21: 1–5.
Tapert SF, Cheung EH, Brown GG, Frank LR, Paulus MP, Schweinsburg AD et al. Neural response to alcohol stimuli in adolescents with alcohol use disorder. Arch Gen Psychiatry 2003; 60: 727–735.
Wrase J, Schlagenhauf F, Kienast T, Wustenberg T, Bermpohl F, Kahnt T et al. Dysfunction of reward processing correlates with alcohol craving in detoxified alcoholics. Neuroimage 2007; 35: 787–794.
Williams LR, Fox NA, Lejuez CW, Reynold EK, Henderson HA, Perez-Edgar K et al. Early temperament, propensity for risk-taking and adolescent substance-related problems: a prospective multi-method investigation. Addic Behav 2010; 35: 1148–1151.
Hill SY, Lowers L, Locke J, Snidman N, Kagan J . Behavioral inhibition in children from families at high risk for developing alcoholism. J Am Acad Child Adolesc Psychiatry 1999; 39: 410–417.
Hawkins JD, Catalano RF, Arthur M . Promoting science-based prevention in communities. Addict Behav 2002; 90: 1–26.
Spoth R, Guyull M, Day S . Universal family-focused interventions in alcohol-use disorder prevention: cost effectiveness and cost-benefit analyses of two interventions. J Stud Alcohol 2002; 63: 219–228.
Jackson KM, Sher KJ, Cooper ML, Wood PK . adolescent alcohol and tobacco use: onset, persistence, and trajectories across two samples. Addiction 2002; 97: 517–531.
Johnston LD, O’Malley PM, Bachman JG . National survey results on drug use from the Monitoring the Future Study. National Institute of Drug Abuse 1975–2002, 2003.
Osgood DW, Wilson JK, Bachman JG, O’Malley PM, Johnston LD . Routine activities and individual deviant behavior. Am Sociological Rev 1996; 61: 635–655.
Chassin L, Pitts SC, DeLucia C . The relation of adolescent substance use to young adult autonomy, positive activity involvement, and perceived competence. Dev Psychopathol 1999; 11: 915–932.
Sher KJ, Trull TJ . Personality and disinhibitory psychopathology: alcoholism and antisocial personality disorder. J Abnorm Psychol 1994; 103: 92–102.
Stewart SH, Morris E, Mellings T, Komar J . Relations of social anxiety variables to drinking motives, drinking quantity and frequency, and alcohol-related problems in undergraduates. J Mental Health 2006; 15: 671–682.
McDermott JM, Perez-Edgar K, Henderson HA, Chronis-Tuscano A, Pine DS, Fox NA . A history of childhood behavioral inhibition and enhanced response monitoring in adolescence are linked to clinical anxiety. Biol Psychiatry 2009; 65: 445–448.
Perez-Edgar K, Bar-Haim Y, McDermott JM, Chronis-Tuscano A, Pine DS, Fox NA . Attention biases to threat and behavioral inhibition in early childhood shape adolescent social withdrawal. Emotion 2010; 10: 349–357.
Perez-Edgar K, Reeb-Sutherland BC, McDermott JM, White LK, Henderson HA, Degnan KA et al. Attention biases to threat link behavioral inhibition to social withdrawal over time in very young children. J Abnorm Child Psychol 2011; 39: 885–895.
Reeb-Sutherland BC, Helfinstein SM, Degnan KA, Perez-Edgar K, Henderson HA, Lissek S et al. Startle response in behaviorally inhibited adolescents with a lifetime occurrence of anxiety disorders. J Am Acad Child Adolesc Psychiatry 2009; 48: 610–617.
Reeb-Sutherland BC, Vanderwert RE, Degnan KA, Marshall PJ, Perez-Edgar K, Chronis-Tuscano A et al. Attention to novelty in behaviorally inhibited adolescents moderates risk for anxiety. J Child Psychol Psychiatry 2009; 50: 1365–1372.
Volkow ND, Li TK . The neuroscience of addiction. Nat Neurosci 2005; 8: 1429–1430.
Brown SA, Myers MG, Lippke L, Tapert SF, Stewart DG, Vik PW . Psychometric evaluation of the Customary Drinking and Drug Use Record (CDDR): a measure of adolescent alcohol and drug involvement. J Stud Alcohol 1998; 59: 427–438.
Brener ND, Kann L, McManus T, Kinchen SA, Sundberg EC, Ross JG . Reliability of the 1999 youth risk behavior survey questionnaire. J Adolesc Health 2002; 31: 336–342.
Kahler CW, Strong DR, Read JP . Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: The brief young adult alcohol consequences questionnaire. Alcohol Clin Exp Res 2005; 29: 1180–1189.
Goldsmith HH . Studying temperament via construction of the toddler behavior assessment questionnaire. Child Dev 1996; 67: 218–235.
Rubin KH . The Play Observation Scale (POS). University of Waterloo, 1989.
Rowe DC, Plomin RT . Temperament in early childhood. J Pers Assess 1977; 41: 50–156.
Cox R . AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comp Biomed Res 1996; 29: 162–173.
Neter J, Kutner M, Machtsheim C, Wasserman W . Applied Linear Statistical Models 4th edn. Irwin: Chicago, IL, 1996.
Cohen M . Parametric analysis of fMRI data using linear systems methods. NeuroImage 1997; 6: 93–103.
Talairach J, Tournoux P . Co-planar Sterotaxic Atlas of the Human Brain. Thieme Verlag: Stuttgart, Germany, 1988.
Viviani R . Unbiased ROI selection in neuroimaging studies of individual differences. NeuroImage 2010; 50: 184–189.
Lieberman MD, Cunningham WA, Type I . and Type II error concerns in fMRI research: Re-balancing the scale. Soc Cog Affect Neurosci 2009; 4: 423–428.
Baron RM, Kenny DA . The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol 1986; 51: 1173–1182.
Aiken LS, West GM . Multiple Regression: Testing and Interpreting Interactions. Sage Publishing: Newbury Park, CA, 1991.
Cohen J . Statistical Power Analysis for the Behavioral Sciences 2nd edn. Lawrence Earlbaum Associates: Hillsdale, NJ, 1988.
Arnett JJ . Adolescence and Emerging Adulthood: A Cultural Approach. Prentice Hall: Upper Saddle River, NJ, 2001.
Leigh BC . In search of the seven dwarves: issues of measurement and meaning in alcohol expectancy research. Psychol Bull 1989; 105: 361–373.
Seymour B, Daw N, Dayan P, Singer T, Dolan R . Differential encoding of losses and gains in the human striatum. J Neurosci 2007; 27: 4826–4831.
Blum K, Braverman ER, Holder JM, Lubar JF, Monastra VJ, Miller D et al. Reward deficiency syndrome: a biogenetic model for the diagnosis and treatment of impulsive, addictive, and compulsive behaviors. J Psychoactive Drugs 2000; 32: 1–112.
Zuckerman M . P-impulsive sensation seeking and its behavioral, psychophysiological biochemical correlates. Neuropsychobiology 1993; 28: 30–36.
Braus DF, Wrase J, Grüsser S, Hermann D, Ruf M, Flor H et al. Alcohol-associated stimuli activate the ventral striatum in abstinent alcoholics. J Neural Transm 2001; 108: 887–894.
Acknowledgements
This research was supported by NIH extramural grants HD17899, MH074454 (NAF) and K01 MH073569-01A1 (KPE), and the Intramural Research Program of the National Institute of Mental Health, NIH Career Development Grant MH080076 (AEG).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Lahat, A., Pérez-Edgar, K., Degnan, K. et al. Early childhood temperament predicts substance use in young adults. Transl Psychiatry 2, e157 (2012). https://doi.org/10.1038/tp.2012.87
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2012.87
Keywords
This article is cited by
-
Portuguese adaptation of the Behavioral Inhibition Questionnaire (BIQ)
Journal of Psychopathology and Behavioral Assessment (2024)
-
Determining the Pathways to Alcohol Use Consequences: a Chained Mediation Approach
International Journal of Mental Health and Addiction (2021)
-
Shyness Trajectories across the First Four Decades Predict Mental Health Outcomes
Journal of Abnormal Child Psychology (2017)
-
Toddler temperament and prenatal exposure to lead and maternal depression
Environmental Health (2016)
-
Behavioral inhibition in childhood predicts smaller hippocampal volume in adolescent offspring of parents with panic disorder
Translational Psychiatry (2015)
