
Abstract
To investigate the efficacy of cervical pessary placement in preventing preterm birth and perinatal morbidity and mortality in asymptomatic women with a singleton pregnancy and a short cervix, we searched literature in relevant databases. The meta-analysis of the 3 included trials (1412 women) showed cervical pessary placement did not reduce the risk of spontaneous preterm birth <34 weeks in these women (risk ratio (RR), 0.71; 95% confidence interval (CI), 0.21–2.43, P = 0.59; I2 = 90%). The sensitivity analyses by excluding one trial at one time showed the same results. This meta-analysis also showed that cervical pessary did not prevent preterm birth <34, 30, 28 weeks and was not associated with respiratory distress syndrome, necrotising enterocolitis, intraventricular haemorrhage, neonatal sepsis, retinopathy of prematurity, fetal death, neonatal death, perinatal death, birth weight <1500 g, birth weight <2500 g, premature preterm rupture of membranes, corticosteroid treatment for fetal maturation, and admission to neonatal intensive care unit. Although this meta-analysis showed cervical pessary placement did not reduce the risk of preterm birth in women with a singleton pregnancy and a short cervix, we could not confirm or refute this conclusion, and large-scale randomised controlled trials are urgently needed.
Similar content being viewed by others


Introduction
Preterm birth is defined as any birth before 37 completed weeks of gestation, or fewer than 259 days of gestation1. Preterm birth is a major determinant of neonatal morbidity and mortality and has lifelong adverse consequences on health2. It is estimated that preterm birth accounts for more than one third of the 3.072 million neonatal deaths in the world in one year3. Preterm birth is also the leading cause of child death in nearly all middle and high-income countries3. Moreover, the morbidity associated with preterm birth such as cerebral palsy, learning disability, and chronic disease in adulthood results in enormous economic and social cost1,4.
Spontaneous preterm birth accounts for two thirds of preterm birth, and is also the most common cause of extremely preterm birth, which is any birth before 28 weeks, whereas the rest is medically indicated due to maternal or fetal complications such as preeclampsia, or intrauterine growth restriction5. Spontaneous preterm birth is a syndrome caused by multiple pathological processes such as inflammation, vascular disease, and disruption of maternal-fetal tolerance6. However, the precise cause of spontaneous preterm birth is unexplained in more than 50% of all the cases1. A short cervix, defined as a cervical length ≤25 mm on transvaginal ultrasound in the mid-trimester of pregnancy, which is one of the most important risk factor for preterm birth, has emerged as one of the strongest predictors of preterm birth in asymptomatic women with a singleton pregnancy7,8,9. Despite great efforts in research and treatment over the last few decades, preterm birth remains a formidable challenge to obstetricians.
Cervical pessary made of silicone or plastic, which is available in different shapes and sizes, has been used to prevent preterm birth in the past 50 years10. The precise mechanism of action by which cervical pessary may prevent preterm birth is largely unknown. One potential mechanism is that it functions in a mechanical manner by bending the cervix posteriorly. Thus, the pressure on the internal cervical ostium would be directed on the anterior lower uterine segment11. Another suggested mechanism is that by encompassing the cervix and compressing the cervical canal, the cervical pessary might protect cervical mucus plug, which plays an important role in pregnancy maintenance11.
A previous systematic review showed a need for more randomised trials to confirm the beneficial effects of cervical pessary in reducing preterm birth12. However, the latest trial indicated that cervical pessary did not result in a lower rate of spontaneous preterm birth in women with a singleton pregnancy and a short cervix compared with expectant treatment13. Therefore, we found it necessary to conduct a meta-analysis to evaluate the efficacy of cervical pessary placement in preventing preterm birth in women with a singleton pregnancy and a short cervix.
Methods
Search strategy
We conducted a systematic search for the relevant published literature without language restrictions until November 1st 2016 using the following databases: PubMed, the Cochrane Central Register of Controlled Trials, and Embase. The following medical subject heading (MeSH) terms, keywords, and their combinations were used: pessary; premature birth(‘preterm’, ‘premature’); premature labor(‘preterm’, ‘premature’). Appropriate suffixes were used for each database. We also manually searched the reference lists of the initially identified articles, previously published meta-analyses and reviews for additional relevant publications.
Study selection and data extraction
We included randomised controlled trials comparing pessary therapy with expectant treatment for prevention of preterm birth in asymptomatic women with a singleton pregnancy and a short cervical length ≤25 mm as determined by ultrasonography in the mid-trimester. We excluded trials assessing cervical pessary placement in women with premature rupture of membranes, regular uterine contractions, or mid-trimester bleeding. Two independent reviewers screened the titles and abstracts to identify potentially eligible trials and then retrieved and assessed the full texts of the relevant citations for inclusion. The data extracted included the first author, year of publication, population characteristics, intervention details, reported outcomes, and study design. Data extraction was performed independently by two of the reviewers. Any disagreement between the two reviewers was solved unanimously through discussion. The Cochrane risk of bias tool has been used for risk assessment in included studies14. This tool assesses seven domains of risk of bias (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias), and categorises randomised trials by ‘low, unclear or high risk of bias’ in each domain.
Outcomes
The primary outcome was spontaneous preterm birth <34 weeks of gestation and the secondary outcomes included preterm birth <34, <30 and <28 weeks of gestation; respiratory distress syndrome; necrotising enterocolitis; intraventricular haemorrhage; neonatal sepsis; retinopathy of prematurity; fetal death; neonatal death; perinatal death; birth weight <1500 g and <2500 g; premature preterm rupture of membranes; corticosteroid treatment for fetal maturation; and admission to neonatal intensive care unit.
Data Synthesis
We reported the dichotomous data results after pooling estimates across trials with a random effects meta-analysis as RR with 95% CIs. Heterogeneity was assessed with the I2 statistic. We performed sensitivity analyses to evaluate the effect of risk of bias on the overall results by excluding one trial at one time. All analyses were done using Revman statistical software version 5.
Results
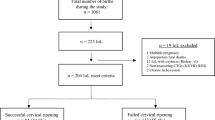
Of the 204 citations identified, 29 were duplicates, and 172 were excluded based on title and abstract. After assessing full texts of the remaining 3 citations, we included 3 randomised controlled trials evaluating efficacy and safety of cervical pessary placement for prevention of preterm birth in this meta-analysis13,15,16. The PRISMA flow diagram illustrating the selection procedure is shown in Fig. 1.

Study selection flow diagram.
Baseline characteristics of the 3 included trials is shown in Table 1.
All the three trials were designed to evaluate the effect of cervical pessary placement on preterm birth in women with a singleton pregnancy and a short cervix13,15,16. Women with a sonographic cervical length <25 mm or ≤25 mm at 18–24 or 20–24 weeks of gestation were included. Women with abnormal conditions such as cervical cerclage, major fetal abnormalities were excluded. Maternal age in the three trials was similar. The women in one trial were Chinese16, and the women in the other two trials were mainly white13,15. All trials used the same type of cervical pessary. Cervical pessary placement was started at 18–22 weeks of gestation in one trial15, at 20–24 weeks of gestation in two trials13,16. Cervical pessary was removed at 37 weeks of gestation, or earlier under certain circumstances such as active vaginal bleeding, painful uterine contractions, and rupture of membranes. Although the primary outcome of the trial by Hui et al.16 differed from that of the other two trials13,15, they were actually the same, as all of the preterm births <34 weeks of gestation were spontaneous preterm births <34 weeks of gestation in this trial16. Control interventions were expectant treatment in these trials13,15,16. Assessment of risk of bias is shown in Fig. 2. Five domains (random sequence generation, allocation concealment, incomplete outcome data, selective reporting and other bias) were assessed as ‘low risk of bias’ in all trials, whereas two domains (blinding of participants and personnel, blinding of outcome assessment) were assessed as ‘high risk of bias’ due to the open-label nature of these trials.

(a) Risk of bias graph, (b) Risk of bias summary (‘+’ low risk; ‘?’ unclear risk; ‘−’ high risk).
Primary outcome
Spontaneous preterm birth <34 weeks of gestation
The meta-analysis of the 3 trials (1412 women) showed cervical pessary placement had no significant effect on spontaneous preterm birth <34 weeks of gestation in women with a singleton pregnancy and a short cervical length ≤25 mm compared with expectant treatment (RR 0.71; 95%CI, 0.21–2.43, P = 0.59; I2 = 90%) (Fig. 3).

Efficacy of cervical pessary placement in preventing spontaneous preterm birth <34 weeks in women with a singleton pregnancy and a short cervix compared with control.
Due to the high heterogeneity, we performed sensitivity analyses to explore the cause of heterogeneity. When we performed the sensitivity analyses by excluding one trial at one time, the results remained the same. However, when the trial by Goya et al.15 was excluded, the high heterogeneity was eliminated (RR 1.14, 95% CI 0.81–1.62, P = 0.46; I2 = 0%).
Secondary outcome
The meta-analysis showed no statistically significant difference between the cervical pessary placement and control groups in preterm birth <34 weeks of gestation (RR 0.75; 95% CI 0.23–2.39, P = 0.62; I2 = 90%), <30 weeks of gestation (RR 1.24; 95% CI 0.78–1.96, P = 0.36; I2 = 0%), <28 weeks of gestation (RR 1.52; 95% CI 0.84–2.74, P = 0.16; I2 = 0%), respiratory distress syndrome (RR 0.79; 95% CI 0.22–2.90, P = 0.72; I2 = 82%), necrotising enterocolitis (RR 0.95; 95% CI 0.11–8.13, P = 0.96; I2 = 47%), intraventricular haemorrhage (RR 1.04; 95% CI 0.63–1.74, P = 0.87; I2 = 0%), neonatal sepsis (RR 0.67; 95% CI 0.23–1.96, P = 0.46; I2 = 69%), retinopathy of prematurity (RR 1.21; 95% CI 0.05–28.10, P = 0.91; I2 = 66%), fetal death (RR 1.61; 95% CI 0.53–4.90, P = 0.40), neonatal death (RR 1.32; 95% CI 0.48–3.66, P = 0.59; I2 = 0%), perinatal death (RR 1.33; 95% CI 0.65–2.76, P = 0.44; I2 = 0%), birth weight <1500 g (RR 0.72; 95% CI 0.18–2.84, P = 0.64; I2 = 90%), birth weight <2500 g (RR 0.60; 95% CI 0.16–2.17, P = 0.43; I2 = 95%), premature preterm rupture of membranes (RR 0.39; 95% CI 0.09–1.71, P = 0.21; I2 = 72%), corticosteroid treatment for fetal maturation (RR 0.75; 95% CI 0.47–1.18, P = 0.22; I2 = 37%), and admission to neonatal intensive care unit (RR 1.23; 95% CI 0.88–1.71, P = 0.23; I2 = 0%) (Table 2).
Discussion
As far as we know, this is the first meta-analysis which combined all the available randomised trials to evaluate the efficacy of cervical pessary in preventing preterm birth and perinatal morbidity and mortality in asymptomatic women with a singleton pregnancy and a short cervix. However, this meta-analysis showed that cervical pessary did not reduce the risk of spontaneous preterm birth <34 weeks of gestation in these women compared with expectant treatment. The sensitivity analyses by excluding one trial at one time showed the same results. This meta-analysis also showed that cervical pessary did not prevent preterm birth <34, 30, 28 weeks of gestation and had no significant adverse effects on perinatal morbidity and mortality.
Cervical pessary is a device which is easily placed and removed without anesthesia, and is inexpensive compared with progesterone and cerclage. Unfortunately, this meta-analysis of the 3 trials showed cervical pessary had no beneficial efficacy in preventing preterm birth in women with a singleton pregnancy and a short cervix, but the heterogeneity is high. Therefore we analysed these trials in detail. First, we noticed that the preterm birth rates in the pessary group were similar in the three trials13,15,16, and the preterm birth rates in the control group were similar in two trials13,16. However, the preterm birth rate in the control group was much higher in the trial by Goya et al.15. In addition, according to the worldwide survey of preterm birth rates in 2010, the preterm birth rate in Spain was less than 10%1, and if we applied this data in this meta-analysis, the result would be the same but the high heterogeneity would be significantly reduced. Therefore, the results of the trial by Goya et al.15 could be a chance finding. Second, in the trial by Nicolaides et al.13, progesterone was used in 45% participants, and as progesterone has proven to be able to prevent preterm birth17,18,19,20, this might compromise the efficacy of cervical pessary. Hence, future large-scale multiple-center randomised trials are urgently needed, before cervical pessary can be generalised in clinical practice.
This meta-analysis showed that cervical pessary had no significant adverse effects on respiratory distress syndrome, necrotising enterocolitis, intraventricular haemorrhage, neonatal sepsis, and perinatal death, among others. No serious side effects were reported in these trials13,15,16, which is consistent with all the published studies21. The most common side effects of cervical pessary placement are an increase in vaginal discharge and pain during the pessary insertion and removal21. Moreover, in the trial by Goya et al.15, 95% of women in the pessary group recommended cervical pessary to others.
This meta-analysis has its limitations. The open-label nature of the trials could result in risk of bias for blinding of participants and personnel and outcome assessment, which hampers the validity of research of cervical pessary. Because of the inconsistence and scarcity of trials, we were unable to explore the effects of maternal age, ethnicity, obstetric history, body mass index, and cervical length on the results. In addition, none of the trials had the power to assess the treatment effect of cervical pessary.
To confirm the efficacy of cervical pessary in preventing preterm birth, future researches may focus on the following respects. First, as progesterone has been suggested to be effective in preventing preterm birth17,18,19,20, combination therapy such as cervical pessary and progesterone compared with progesterone may be considered. Second, although a short cervix is a high-risk factor in preterm birth, the cause of preterm birth is multiple factorial, basic research exploring the mechanisms behind preterm birth is still needed.
In conclusion, although this meta-analysis showed cervical pessary did not reduce the risk of preterm birth in women with a singleton pregnancy and a short cervix, we could not confirm or refute this conclusion, and large-scale randomised controlled trials are urgently needed.
Additional Information
How to cite this article: Jin, X.-H. et al. Cervical Pessary for Prevention of Preterm Birth: A Meta-Analysis. Sci. Rep. 7, 42560; doi: 10.1038/srep42560 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Blencowe, H. et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet (London, England) 379, 2162–2172 (2012).
Beck, S. et al. The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bulletin of the World Health Organization 88, 31–38, doi: 10.2471/BLT.08.062554 (2010).
Liu, L. et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet (London, England) 379, 2151–2161, doi: 10.1016/S0140-6736(12)60560-1 (2012).
Mwaniki, M. K., Atieno, M., Lawn, J. E. & Newton, C. R. Long-term neurodevelopmental outcomes after intrauterine and neonatal insults: a systematic review. Lancet (London, England) 379, 445–452, doi: 10.1016/S0140-6736(11)61577-8 (2012).
Goldenberg, R. L., Culhane, J. F., Iams, J. D. & Romero, R. Epidemiology and causes of preterm birth. Lancet (London, England) 371, 75–84, doi: 10.1016/S0140-6736(08)60074-4 (2008).
Romero, R., Dey, S. K. & Fisher, S. J. Preterm labor: one syndrome, many causes. Science (New York, N.Y.) 345, 760–765, doi: 10.1126/science.1251816 (2014).
Romero, R. et al. Vaginal progesterone decreases preterm birth </=34 weeks of gestation in women with a singleton pregnancy and a short cervix: an updated meta-analysis including data from the OPPTIMUM study. Ultrasound in obstetrics & gynecology: the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 48, 308–317, doi: 10.1002/uog.15953 (2016).
Iams, J. D. et al. The length of the cervix and the risk of spontaneous premature delivery. National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The New England journal of medicine 334, 567–572, doi: 10.1056/NEJM199602293340904 (1996).
Owen, J. et al. Multicenter randomized trial of cerclage for preterm birth prevention in high-risk women with shortened midtrimester cervical length. American journal of obstetrics and gynecology 201, 375 e371–378, doi: 10.1016/j.ajog.2009.08.015 (2009).
Cross, R. G. Treatment of Habitual Abortion Due to Cervical Incompetence. Lancet (London, England) 2, 127–127 (1959).
Arabin, B. & Alfirevic, Z. Cervical pessaries for prevention of spontaneous preterm birth: past, present and future. Ultrasound in obstetrics & gynecology: the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 42, 390–399, doi: 10.1002/uog.12540 (2013).
Abdel-Aleem, H., Shaaban, O. M. & Abdel-Aleem, M. A. Cervical pessary for preventing preterm birth. The Cochrane database of systematic reviews, CD007873, doi: 10.1002/14651858.CD007873.pub3 (2013).
Nicolaides, K. et al. A Randomized Trial of a Cervical Pessary to Prevent Preterm Singleton Birth. The New England journal of medicine 374, 1044–1052 http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/909/CN-01160909/frame.html (2016).
Higgins, J. P. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clinical research ed.) 343, d5928, doi: 10.1136/bmj.d5928 (2011).
Goya, M. et al. Cervical pessary in pregnant women with a short cervix (PECEP): an open-label randomised controlled trial. Lancet (London, England) 379, 1800–1806 http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/235/CN-00832235/frame.html (2012).
Hui, S., Chor, C., Lau, T., Lao, T. & Leung, T. Cerclage pessary for preventing preterm birth in women with a singleton pregnancy and a short cervix at 20 to 24 weeks: a randomized controlled trial. American journal of perinatology 30, 283–288 http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/261/CN-00968261/frame.html (2013).
Fonseca, E. B. et al. Progesterone and the risk of preterm birth among women with a short cervix. New England Journal of Medicine 357, 462–469, doi: 10.1056/NEJMoa067815 (2007).
Hassan, S. S. et al. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound Obst Gyn 38, 18–31, doi: 10.1002/uog.9017 (2011).
Norman, J. E. et al. Progesterone for the prevention of preterm birth in twin pregnancy (STOPPIT): a randomised, double-blind, placebo-controlled study and meta-analysis. Lancet (London, England) 373, 2034–2040, doi: 10.1016/S0140-6736(09)60947-8 (2009).
Rode, L. et al. Prevention of preterm delivery in twin gestations (PREDICT): a multicenter, randomized, placebo-controlled trial on the effect of vaginal micronized progesterone. Ultrasound in obstetrics & gynecology: the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 38, 272–280, doi: 10.1002/uog.9093 (2011).
Wetta, L. A. & Biggio, J. R. Cervical Pessary Use and Preterm Birth. Clinical obstetrics and gynecology 57, 607–615 (2014).
Author information
Authors and Affiliations
Contributions
X.J. and L.H. conceived the idea. X.J. and D.L. screened studies, extracted and analyzed the data. X.J., D.L. and L.H. solved disagreements unanimously. X.J. and D.L. performed statistical analysis. X.J. wrote the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Jin, XH., Li, D. & Huang, LL. Cervical Pessary for Prevention of Preterm Birth: A Meta-Analysis. Sci Rep 7, 42560 (2017). https://doi.org/10.1038/srep42560
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep42560
This article is cited by
-
The impact of cervical conization size with subsequent cervical length changes on preterm birth rates in asymptomatic singleton pregnancies
Scientific Reports (2021)
-
Effectiveness of the cervical pessary for the prevention of preterm birth in singleton pregnancies with a short cervix: a meta-analysis of randomized trials
Archives of Gynecology and Obstetrics (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
