
Abstract
According to the placebo-reward hypothesis, placebo is a reward-anticipation process that increases midbrain dopamine (DA) levels. Reward-based learning processes, such as reinforcement learning, involves a large part of the DA-ergic network that is also activated by the placebo intervention. Given the neurochemical overlap between placebo and reward learning, we investigated whether verbal instructions in conjunction with a placebo intervention are capable of enhancing reward learning in healthy individuals by using a monetary reward-based reinforcement-learning task. Placebo intervention was performed with non-invasive brain stimulation techniques. In a randomized, triple-blind, cross-over study we investigated this cognitive placebo effect in healthy individuals by manipulating the participants’ perceived uncertainty about the intervention’s efficacy. Volunteers in the purportedly low- and high-uncertainty conditions earned more money, responded more quickly and had a higher learning rate from monetary rewards relative to baseline. Participants in the purportedly high-uncertainty conditions showed enhanced reward learning, and a model-free computational analysis revealed a higher learning rate from monetary rewards compared to the purportedly low-uncertainty and baseline conditions. Our results indicate that the placebo response is able to enhance reward learning in healthy individuals, opening up exciting avenues for future research in placebo effects on other cognitive functions.
Similar content being viewed by others

Introduction
Observational and interventional approaches are concomitantly used to study brain networks and their putative contributions to certain brain functions1. While the former approach is necessary to characterize the spatiotemporal patterns of neural activity, the interventional approach constitutes an important step towards facilitating causal inference2. Non-invasive brain stimulation (NIBS) interventions offer the possibility to induce transient perturbations in intact human brain networks by using electromagnetic induction or electrical current, while minimizing possible health risks, financial costs and ethical concerns3,4,5.
Transcranial direct current stimulation (tDCS) is the most frequently employed research tool in studies that use electrical current as a NIBS technique3. It passes constant, low intensity current between two or more electrodes attached to the intact scalp. Depending on the polarity, the externally applied constant current can increase or decrease the spontaneous firing rate (i.e., cortical excitability) of the stimulated brain regions by depolarizing or hyperpolarizing resting membrane potentials3. Although most of the commercially available and certified tDCS devices are equipped with a double-blind operation mode, a large number of studies still use a single-blind study design, no blinding at all or inadequate blinding6. In these cases, the impact of intentional and unconscious preferences, bias and expectations of the participants as well as of the researchers can possibly lead to an overestimation of its effectiveness. While several tDCS methods have been shown to be effective in the motor and cognitive domains, the variability in the response rate to tDCS is relatively high and it is unclear how much of the observed effectiveness is solely due to a placebo effect7,8,9.
The placebo effect is a complex psychobiological response to the application of a simulated intervention10,11,12,13. A prominent conceptual framework focusing particularly on the dopamine (DA)-mediated placebo mechanisms suggests that the placebo response can be considered a special case of a reward anticipation process, characterized by a neural overlap between anticipating the putative beneficial effects of the treatment and anticipating rewards14,15. In line with this hypothesis, substantial placebo-induced release of DA was detected both in the nigrostriatal and mesolimbic DA-ergic pathways, key regions in reward processing16,17,18,19, using positron emission tomography (PET)14,20,21,22,23,24.
Although the overwhelming majority of placebo studies focused primarily on placebo analgesia, a recent study of the placebo effects on reward learning indicates that there may be a common neurobiological mechanism of placebo effects across multiple domains24. Using pharmacological, neuroimaging and computational modeling measures, this study revealed that placebo medication enhances reward learning in Parkinson’s disease (PD) patients, and that the effects were driven by the DA-ergic system. However, due to the characteristics and the pharmacological treatment of PD patients, it remains elusive whether this cognitive placebo effect was mediated by placebo-induced expectations or also partly due to conditioning by the pharmacological treatment that the PD patients were receiving. Since PD patients are characterized by pathological DA-ergic network functioning25, they may constitute a subpopulation that is particularly responsive to the placebo intervention.
In the current study we therefore examined whether placebo interventions associated with different verbal manipulations would be capable of enhancing reward learning in healthy individuals. This active placebo intervention was applied using sham protocols of NIBS for the following reasons. First, in the past decade the application of tDCS has become increasingly popular in neuroscience research investigating both healthy individuals and patient populations. Recent years have seen an enormous increase in the use of tDCS extending well beyond academic and clinical applications to, e.g., do-it-yourself brain stimulation communities and professional athletes26,27. However, the placebo-inducing potential of tDCS is under-researched, although the placebo effect induced by medical devices are as strong or even superior to orally administered placebos28. Second, despite its extensive application in the motor and cognitive domains, its precise mechanism of action remains elusive, and the high inter-individual variability in the response to tDCS has yet to be further investigated7,8,9. Third, the ‘fade-in, short-stimulation, fade-out’ protocol is a well-characterized sham condition for tDCS, that produces a mild degree of cutaneous discomfort, such as itching, tingling or burning sensations on the scalp but does not induce physiological after-effects. Hence, for the purpose of the present study tDCS was an ideal candidate for an active placebo intervention (i.e., inducing mild sensations).
In addition to tDCS, we also employed another NIBS device called transcranial near infrared laser stimulation (tNILS) as a passive placebo (i.e. inducing no sensations). Earlier findings have shown that tNILS can alter cellular respiration processes by increasing mitochondrial adenosine triphosphate synthesis and cellular nitric oxide release29. Due to its effects at the molecular and cellular levels, tNILS has been shown to induce vasodilation that is beneficial in wound healing and in reducing inflammatory processes29. Similar to tDCS, tNILS can modulate cortical excitability in the human motor cortex30. Although tNILS has been applied in neurorehabilitation31, our knowledge about its effect on cognitive functions is limited32. The rationale for the application of tNILS was first to provide different treatment characteristics for the repeated-measures design both for the participants and the operator, and second, to avoid the possibility that participants or the operator would encounter earlier scientific publications on the effect of tDCS on cognitive functions that would contradict the verbal manipulation.
Earlier studies reported that placebo effects are most pronounced when the volunteers believed that they are certain to receive an active intervention33,34,35,36. Therefore, in the present experiment, participants were subjected to two active placebo conditions, in which the participants were misleadingly informed that they would receive an active intervention. Crucially, however, the two placebo conditions differed with regard to the declared certainty about the effectiveness of the intervention. In the low-uncertainty condition, the intervention (tDCS and tNILS) was introduced as a well-established, performance-enhancing method and was claimed to certainly improve the participants’ cognitive performance. In contrast, in the high-uncertainty condition, the active placebo stimulation was introduced as an experimental method whose effectiveness was not yet proven. In reality, all participants received 30 s of sham tDCS as an active placebo using a randomized, triple-blind (i.e., participant, operator and analyst were unaware of the conditions37), cross-over study design.
We considered two competing hypotheses regarding the possible outcomes of our study. First, it is conceivable that participants will show a stronger placebo effect when instructed that the effect is more certain, i.e., better learning will be observed in the low-uncertainty than in the high-uncertainty condition. This expectancy hypothesis is based on the assumption that the verbal manipulation will differentially increase the participants’ expectations, which eventually results in stronger cognitive placebo effects in the low-uncertainty condition, similar to the observations in the domain of placebo analgesia33,35,38. However, the opposite hypothesis, i.e., that the placebo effect would be stronger in the condition where treatment efficacy is less certain, is also conceivable in the light of the placebo-reward theory14,15. Based on the findings in PD patients, this theory proposes that the development of the placebo effect is tightly coupled to the activation characteristics of the reward circuit to reward uncertainty15. It has been shown that the tonic activation of midbrain DA neurons and, correspondingly, reward uncertainty are related by an inverted U-shape function with strongest activation when uncertainty is maximized15,22. If cognitive placebo effects are mediated by the activation of the reward circuit, then the low-uncertainty condition (according to the expectancy hypothesis) or the high-uncertainty condition (according to the placebo-reward hypothesis) could conceivably increase endogenous midbrain DA release, which could modulate reward processing and eventually lead to a more pronounced placebo effect.
Therefore, we hypothesized that if the placebo intervention were indeed capable of modulating reward learning in healthy individuals similar to PD patients24, we would be able to detect its behavioral consequences in a monetary reward-based reinforcement-learning task. This task is a well-characterized paradigm, known to strongly depend on midbrain DA levels17,39,40,41,42,43. In order to gain further insight into the underlying mechanisms of how placebo affects reinforcement learning, we applied a computational, temporal-difference reinforcement learning technique using a hierarchical Bayesian estimation procedure. The learning rate parameter used in our model represents the degree to which participants were able to learn from the reward prediction error, the difference between the obtained and the predicted reward. If the active placebo intervention(s) did indeed activate the reward circuitry, we would expect an increased learning rate from monetary rewards (i.e., optimized learning from gains), similar to the behavioral consequences of pharmacological studies in which the DA-ergic network was triggered by medication44,45.
Results
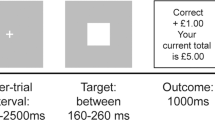
We monitored participants’ performance during three repetitions of a standard reinforcement-learning task using unrelated stimulus sets39. In this task, the participants had to choose between pairs of Chinese symbols that were probabilistically mapped to a reward42. To optimize their monetary outcome, participants had to learn the stimulus that yielded a reward with maximum probability. Participants took part in three sessions. In each experimental session, participants had to learn three distinct stimulus pairs that had different reward contingencies (80/20%, 70/30% and 60/40%, see Fig. 1B). The first session served as a baseline condition and the other two sessions were placebo conditions, in which the participants’ belief about the effectiveness of the intervention was manipulated by verbal instruction (low-uncertainty vs. high-uncertainty condition, see Fig. 1A and Methods for details). Placebo intervention was delivered by an active sham protocol of tDCS (see Methods for details) that is insufficient to induce physiological changes in the brain, but capable of inducing substantial cutaneous sensations46,47.

Flow of the volunteers through the conditions (A) and trials (B). (A) After a neurological screening, all participants first entered a baseline condition followed by the two randomly ordered placebo conditions (low- and high-uncertainty). (B) Participants performed a standard reinforcement-learning task39 where they had to select the better of two Chinese symbols.
For data analysis, we exclusively used Bayesian methods because of their many advantages compared to traditional null-hypothesis testing in general48,49 and in particular because they allow a hierarchical integration of the computational reinforcement-learning model50. We report our results in terms of posterior mean and the 95% highest-density intervals (HDIs), which give the range in which the estimated parameter is expected to be located with probability 0.95 given the model assumptions.
Placebo increases objective performance measures
We analyzed learning performance by submitting the accuracy and reaction time data from the learning part of the experiment to independent Bayesian hierarchical generalized regression models. We included trial number, condition (baseline; low- uncertainty, LU; high-uncertainty, HU) and pair number (1, 2, 3) as predictors and let the intercept vary by subject (Methods for details). Non-informative priors were placed on all parameters (see Table 1 for a summary of the models’ results).
The results from this analysis clearly show substantially increased performance compared to baseline, both with regard to accuracy (bLU = 0.217, HDI = [0.146, 0.279] and bHU = 0.435, HDI = [0.370, 0.503]) as well as to reaction times (bLU = −0.116, HDI = [−0.124, −0.107] and bHU = −0.145, HDI = [−0.153, −0.136]). Even though new and randomized stimuli were used in each of the three sessions, it is possible that these effects are at least partly driven by a between-session practice effect from baseline to the (randomized) placebo conditions. Crucially, however, the performance boost was greater (evidenced by a greater increase in accuracy and a greater reduction in RT) in the high-uncertainty condition than in the low-uncertainty condition as indicated by the non-overlapping HDIs for all parameters.
We also found the expected effect of trial number on accuracy, b = 0.144, HDI = [0.127, 0.160], and RT, b = −0.043, HDI = [−0.045, −0.041], indicating learning over the course of the experiment. Finally, the effect of pair number, reflecting increasing difficulty due to lower reward contingencies, was in the expected directions for accuracy, b = −0.497, HDI = [−0.532, −0.463] and reaction times, b = 0.023, HDI = [0.019, 0.027]. Descriptive statistics of the performance data are summarized in Fig. 2.

Descriptive statistics for accuracy (% correct, (A)) and reaction time (in s, (B)) for each condition and stimulus pair. Error bars show the standard error of the mean (SEM). Accuracy increases and reaction time decreases in both placebo conditions, but more strongly in the high-uncertainty condition. Accuracy and RT also depend on stimulus pair, reflecting their increasing degree of difficulty due to lower stimulus-reward contingencies. HU: high-uncertainty; LU: low-uncertainty placebo conditions
Uncertainty modulates learning rate parameters of the reinforcement-learning model
To investigate the possible impact of our placebo manipulations on the learning rates, we fitted a computational reinforcement- learning model specifically designed for this task39 (see Methods). This model was designed to capture two independent learning-rate parameters, αG and αL, reflecting the participants’ propensity to learn from gains and losses, respectively39,51. It has been suggested39 that learning from losses and gains might be implemented in different underlying neural mechanisms. In a data-driven model-comparison, we found that this more complex model clearly outperforms a model that does not separate between gains and losses, ΔWAIC = 539.93. We fitted a hierarchical Bayesian version of this model (see Methods) and estimated the effects of the placebo intervention on the learning rate parameters αG and αL and the noise parameter β.
At the group level, the estimates for the learning rates and the noise parameter were in a reasonable range with the learning- rate for losses being lower than that for gains,  , HDI = [0.03, 0.12],
, HDI = [0.03, 0.12],  , HDI = [0.004, 0.03] and μβ = 0.21, HDI = [0.18, 0.25] (see Fig. 3). The effect of the placebo interventions was restricted to the learning-rate parameters (see Table 2: Learning from gains was improved in both placebo conditions and substantially more so in the high-uncertainty condition (δLU = 0.83, HDI = [0.55, 1.10] and δHU = 1.17, HDI = [0.96, 1.39], P(δHU > δLU) = 0.99), mirroring the results from the analysis of accuracy and reaction times. In addition, both placebo manipulations induced a substantial, but small, decrement of the learning rate from losses, δLU = −0.74, HDI = [−1.11, −0.36], δHU = −0.86, HDI = [−1.37, −0.37] but the two conditions did not differ from one another. Finally, there was no effect on the noise-parameter β (δLU = −0.02, HDI = [−0.11, 0.07]; δHU = 0.05, HDI = [−0.04, 0.14]). To better interpret the size of the effects, which are give on the logit/log scales, we transformed them to the original scale when the intercept was at the mean (Fig. 4). While the effect on αG was quite strong (≈0.1), it was much weaker for the αL parameter (≈−0.01).
, HDI = [0.004, 0.03] and μβ = 0.21, HDI = [0.18, 0.25] (see Fig. 3). The effect of the placebo interventions was restricted to the learning-rate parameters (see Table 2: Learning from gains was improved in both placebo conditions and substantially more so in the high-uncertainty condition (δLU = 0.83, HDI = [0.55, 1.10] and δHU = 1.17, HDI = [0.96, 1.39], P(δHU > δLU) = 0.99), mirroring the results from the analysis of accuracy and reaction times. In addition, both placebo manipulations induced a substantial, but small, decrement of the learning rate from losses, δLU = −0.74, HDI = [−1.11, −0.36], δHU = −0.86, HDI = [−1.37, −0.37] but the two conditions did not differ from one another. Finally, there was no effect on the noise-parameter β (δLU = −0.02, HDI = [−0.11, 0.07]; δHU = 0.05, HDI = [−0.04, 0.14]). To better interpret the size of the effects, which are give on the logit/log scales, we transformed them to the original scale when the intercept was at the mean (Fig. 4). While the effect on αG was quite strong (≈0.1), it was much weaker for the αL parameter (≈−0.01).

Dots indicate the posterior mean and the flankers the 95% highest-density interval (HDI). Black solid line indicates the mean of the group-level distribution and dashed lines the 95% HDI for that parameter.

Circles represent the posterior mean, solid bars show the corresponding HDI. The thin red line indicates zero effect.
Subjective expectation and experience is unaffected by placebo intervention
We also asked our participants whether they anticipated or experienced a positive, negative or no impact of the intervention on their performance. The results of the responses to these questions are summarized in Fig. 5. We submitted these data to a softmax-regression model49 using type of question (anticipated vs. experienced changes) and condition (low- and high-uncertainy) as well as their interaction as predictors (see section 6 for details). None of the predictors showed a substantial deviation from zero (see Table 3). There was no strong evidence of a main effect of question (anticipated vs. experienced changes in performance), β2,decline = −1.53, HDI = [−4.72, 1.50], β2,improve = −0.92, HDI = [−2.10, 0.21] (both HDIs include zero). There was no apparent effect of condition (low- vs. high-uncertainty), β1,decline = 0.50, HDI = [−1.66, 2.77] and β1,improve = −0.06, HDI = [−1.25, 1.15] and neither an interaction of question and condition showed β3,decline = 2.02, HDI = [−1.41, 5.64], β3,improve = −0.51, HDI = [−2.25, 1.24]. All of the HDIs include zero and we cannot conclude with confidence that subjective anticipations or experiences were influenced by the placebo intervention.

The anticipated and experienced impact (decline, no change or an improvement) of the intervention reported by the participants in the high-uncertainty (HU) and low-uncertainty (LU) placebo conditions.
To make the results of this model more interpretable, we calculated the associated probabilities p for each of the conditions and questions. These values indicate estimated probabilities for each condition to anticipate or experience a decline, no change, or an improvement in performance due to the placebo intervention. In both conditions, anticipated changes in performance were similar and mainly neutral or positive, pLU = (0.07, 0.34, 0.59) and pHU = (0.10, 0.34, 0.56), (Fig. 6, left). Regarding the experienced performance changes, the estimated probabilities show a somewhat stronger tendency to experience no change, and more “decline”, and fewer “improve” ratings in the HU condition pLU = (0.03, 0.56, 0.41), pHU = (0.26, 0.52, 0.22), (see Fig. 6, right). However, the 95% highest-density regions (HDRs) for these estimates overlap (corresponding to the inconclusive HDIs on the interaction parameter) and any putative difference must therefore be interpreted carefully.

Dots show the posterior mean, outlines show the 50%, 80% and 95% Highest-density regions (HDRs).
Self-reported arousal was unaffected by placebo intervention
To exclude the possibility that our results reflect the effect of a general arousal due to the presence of an intervention rather than a genuine placebo effect, we asked our participants to rate their arousal before and after each experimental session on a scale from one to ten. This data was subjected to a similar analysis as the one above.
In general, our participants reported being quite awake as indicated by the fact that most responses were located at the upper end of the scale, μ0 = 7.22, HDI = [6.56, 7.86]. Participants’ responses after an experimental session were generally lower than before, βafter = −0.91, HDI = [−1.71, −0.11] (approximately one point on the ten point scale). There was no apparent effect of either condition (βLU = −0.32, HDI = [−1.05, 0.51], βHU = −0.18, HDI = [−0.91, 0.62]) or a modulation of the before/after effect due to condition (βLU×after = 0.10, HDI = [−1.05, 1.19], βHU×after = −0.11, HDI = [−1.23, 1.02]. We conclude that there is no apparent effect of the placebo stimulation on subjectively experienced arousal.
Discussion
We investigated whether verbally manipulating the participants to be more or less certain about the effectiveness of the applied placebo NIBS would influence the performance of healthy individuals in a reinforcement-learning task, i.e., induce a cognitive placebo effect. We found that performance was increased in both low- and high-uncertainty conditions but more strongly in the high-uncertainty condition. Our Bayesian analysis revealed that participants in the high-uncertainty condition learned better from monetary rewards, compared to the low-uncertainty and training conditions. We found no difference in the subjective expectations reported in the two sessions.
The question of whether the placebo response is confined to placebo analgesia or patient-reported symptoms of various diseases has provoked a considerable debate in the placebo literature during the past years52. To date, only a handful of studies have investigated the placebo effect in the cognitive domain24,53,54, and even fewer studies deal with healthy persons55,56,57,58. Only one study investigated the possible biological systems involved in the generation of cognitive placebo effects by examining PD patients24. The study showed that placebo medication enhanced reward learning. The results of neuroimaging and computational measurements led to the conclusion that the observed cognitive improvement was mediated by the DA-ergic system24. Nevertheless, it remained unclear whether verbal manipulation alone can induce a cognitive placebo effect, or whether this is mediated by a combination of verbal manipulation and conditioning. PD patients have typically undergone several months or even years of DA-ergic treatment, and prior experience with the beneficial effect of the pharmacological intervention is thought to promote positive preconceived expectations from the treatment, also known as conditioning. Thus, PD patients with a malfunctioning DA-ergic system might constitute a special patient population that is particularly responsive to placebo intervention in reward learning, since the same DA-ergic system is targeted by the DA-restoring pharmaceuticals. We therefore only recruited healthy individuals who had no prior experience with DA-ergic medication.
Our findings constitute the first behavioral evidence of a cognitive placebo effect in a reinforcement-learning task in healthy individuals induced by the combined application of verbal manipulation and sham protocols of NIBS interventions. Furthermore, the pattern of our behavioral and computational modeling results are conceptually compatible with the findings in the reward learning in PD patients reviewed above, as both studies observed behavioral improvement in reward learning and optimized learning rate parameters for rewards. We extended earlier findings on cognitive placebo effects to include healthy adults and to NIBS interventions. This is of particular importance given that our results can potentially be applied to a wide range of laboratory situations.
In order to induce physiological or behavioral after-effects, tDCS needs to be applied at least for three minutes at 1 mA, because shorter stimulation protocols only induce immediate effects59. Beyond the primary physiological effects that constitute the main focus of most of the NIBS studies, the application of tDCS even at relatively low intensities (starting from about 0.4 mA) induces intensity- and electrode size-dependent cutaneous sensations, also known as the secondary induced effect of tDCS, which requires the use of an active sham control47,60,61. The most frequently applied sham protocol for tDCS is the so called ‘fade-in, short stimulation, fade-out’ protocol46, which is thought to lack any physiological or behavioral after-effects due to the low stimulation intensity and short stimulation duration59. Still, the present experiment has demonstrated that even an active sham protocol of tDCS is able to modify cognitive performance in healthy individuals when it is combined with verbal manipulation. Although tDCS is the most popular electrical NIBS intervention, its placebo-inducing potential in the cognitive domain was unknown until now. This is an important knowledge gap given that its precise mechanism of action is not fully understood, and that there is a relatively high response variability7,8,9. We therefore posit that, in addition to other variance-inflating factors such as individual brain anatomy and brain state before and during stimulation, individual differences in the susceptibility to the placebo intervention are important factors to consider when elucidating for which individuals tDCS would be effective.
Our results highlight the importance of careful study designs and data acquisition in NIBS studies. We argue that uncertainties regarding the expected efficacy of tDCS can be conveyed to the participants via the consent forms or during the interactions between participants and researchers in a manner similar to our verbal manipulations, and can induce cognitive placebo effects and increase effectiveness of the treatment. As most of the ISO certified stimulators are capable of operating in double-blind study mode, performing randomized double-blind placebo-controlled tDCS studies does not require additional investments, and double-blind designs should be required. Further, tDCS studies may consider assessing preconceptions, expectancy and former knowledge on the part of the participants about the expected efficacy of tDCS as our results indicate that these preconceptions might shape the resulting effect of the intervention. In spite of best efforts, blinding efficacy cannot always be maintained throughout the stimulation6. We therefore further recommend collecting information on the blinding efficacy and the perceived treatment if blinding is inadequate.
Our behavioral and computational data showed greater learning enhancement in the high-uncertainty condition compared to the low-uncertainty condition. It may be that the perceived improvement relative to baseline, or the less notable difference relative to the low-uncertainty condition led the participants to believe that the stimulation was, in fact, effective. In the domain of placebo analgesia, Rief and colleagues35 compared the effect of passive placebo (i.e., causing no sensations) and active placebo (i.e., causing minor sensations, such as in the present study) when the probability of receiving a drug was 0, 0.5 and 1. The authors found that active placebo, which is conceptually equivalent to our low- and high-uncertainty conditions substantially increased the placebo effect compared to the passive placebo in the 0.5 probability condition. It is assumed that the participants attributed the minor side-effects associated with the active placebo treatment to having received an active treatment. Thus, in the context of the present study the improvement in the high-uncertainty condition relative to the training session together with the cutaneous sensations may have implicitly biased the participants toward believing that the behavioral improvement was due to the applied intervention. The experience of improvement in the high-uncertainty condition may further reinforce the participants’ belief while performing the cognitive task that the intervention was effective and actually enhanced their performance. This hypothesized effect may be analogous to observations in the pain domain, where the relief from pain is rewarding in itself62.
Our main finding of enhanced learning in the high- relative to the low-uncertainty condition is based solely on behavioral data and computational modeling results, and we did not measure brain activity directly. Nevertheless, we can speculate that a biologically plausible explanation for our results is that the placebo stimulation together with the verbal instructions, triggered DA release in the midbrain as observed earlier in PD patients24. Because the placebo responses access the DA-ergic network which neurophysiologically overlaps with the neural network involved in reinforcement-learning, the increased DA levels would hypothetically be able to induce enhanced task performance and optimize learning rate from monetary rewards. This effect has been observed in earlier studies in which DA-ergic signaling was enhanced pharmacologically44,45. Since the tonic response of the midbrain DA-ergic neurons is maximized when reward uncertainty is high, we posit that the higher uncertainty triggered endogenous midbrain DA release that could have in turn improved the learning performance. As our study lacks physiological or neuroimaging data to support our assumptions, future research concentrating on the biological mechanisms of cognitive placebo effects in healthy participants will provide more insight into the role of DA-level dynamics in this phenomenon.
Reducing performance in the reinforcement learning task to the model-free learning system might be an oversimplification, since there are different neurobiological systems that support performance in the this task. We showed that placebo influenced the model-free learning system, but our results do not exclude the possibility that the cognitive placebo effect might be modulated by more explicit decision strategies (model-based system) that are not captured by the model used here, or by attentional influences that might be modulated by uncertainty63. In addition, DA is only one of the neurotransmitters involved in generating the placebo response, as opioid, endocannabinoid and serotonergic systems have also been shown to be contributing factors although in different domains of interest13,64,65,66,67. Moreover, although we found no difference in the subjectively reported arousal level between any of the applied conditions, differences in the stress level induced by the different stimulation setups could have influenced the observed placebo effect68. Future studies are needed to address the impact of arousal and stress on the cognitive placebo effect.
The fact that we observed no difference between the two placebo conditions in terms of subjectively reported expectations is somewhat surprising, given the explicit differences in the instructions. Together with the clear behavioral differences between the conditions, this intriguing pattern of results needs to be investigated in future studies using more in-depth measures of subjective expectations. Our experiment assessed explicit expectations with a single question: “What do you think? Will the stimulation change your performance?” posed immediately after the instruction and before the stimulation. This simple question might have been too coarse to detect differences in expectancy. Furthermore, our approach did not differentiate between different dimensions of expectancy such as strength and confidence. For instance, it would be interesting to study whether expectancy confidence or strength of expectancy was modulated by the placebo intervention. In addition, expectancy shifts and confidence levels could be assessed multiple times during the experiment to evaluate the development of these values in the course of performing the tasks. It is also possible that the introduction of the NIBS device in the high-uncertainty condition distracted the participants in such a fashion that they were less able to concentrate on the verbal manipulation. In order to investigate this scenario, additional experiments are required that employ the NIBS device without the verbal manipulation. Alternatively, future studies could combine verbal manipulation with conditioning by surreptitiously manipulating the feedback given the participants in each trial, which would make the task subjectively easier or more difficult. We expect that such a procedure would have the potential to influence the participants’ expectations to a larger extent.
Another limitation is the gender of the participants, as the present study recruited only males to avoid gonadal steroid mediated changes in DA signaling observed in an earlier study with females69. By controlling estradiol and progesterone levels between the different conditions, future studies that include females could investigate the placebo response in both genders70,71. Furthermore, the present findings are confined to the placebo effect, and it has yet to be investigated whether a cognitive nocebo effect, a decrease in learning performance following the administration of an simulated intervention, could be similarly evoked by verbal instruction53,68,72. Finally, careful replication studies are needed, preferably performed by independent laboratories, in order to confirm our findings and investigate whether the present results can be generalized to various other cognitive tasks, personality traits, genetic factors or different cultures11,53,57,73.
Overall, our behavioral and computational modeling results support the idea that placebo is a powerful phenomenon to improve reward learning even in healthy individuals. We showed that a cognitive placebo effect in healthy individuals does not necessarily require a conditioning procedure but can be evoked purely by verbal manipulation combined with sham NIBS protocols. Our results open up novel and exciting avenues of future research on the effects of cognitive placebo and highlight the importance of carefully designing informed consent forms, controlling contextual information and social interaction in NIBS studies.
Methods
Participants
Thirty participants were recruited for the experiment via online advertisement. All participants signed an informed consent form. The experiment was approved by the Ethic Committee of the University Medical Center Göttingen and was performed in accordance with relevant guidelines and regulations. Twenty-nine volunteers completed the study (mean age: 23.3 ± 2.95 yrs; mean years of education: 15.8 ± 2.35 yrs), as one participant did not return after the first session. In order to avoid menstrual cycle-dependent alterations in reward-related neural processing69, only male participants were recruited. None of the participants was familiar with Chinese or Japanese characters, similar to the procedure of an earlier study39. Before being finally recruited, the volunteers went through a neurological screening performed by a neurologist at the Department Clinical Neurophysiology, University Medical Center Göttingen, who was blinded to the genuine purpose of the study. Exclusion criteria included a history of current medical, neurological or psychiatric illnesses including epilepsy, drug and/or alcohol addiction, and the presence of metal implants in the head, neck and chest. Participants were asked about prior experience with brain stimulation. Only one participant had had prior experience with transcranial magnetic stimulation (TMS) and one other with transcranial direct current stimulation (tDCS). In both cases, the stimulation had been delivered to the motor cortex.
Placebo induction and blinding procedure
The operator responsible for participant recruitment and for data collection was blinded to the purpose of the study and to the stimulation parameters during the time course of the entire study. The efficacy of blinding was confirmed verbally at the end of the study by the primary investigator. The operator was a native German medical student (22 year-old, female), naïve to tDCS and transcranial near infrared light stimulation (tNILS) studies and had no prior experience with non-invasive brain stimulation research. Before the start of the study, the operator received several weeks of special training in data collection. As the emotional characteristic of the experiment was not manipulated, the operator was instructed to use a neutral style during the consultation. In addition, the researcher performing the formal data analysis was unaware of which of the three conditions was the baseline, low- and high-uncertainty condition, respectively, until the data analysis was completed. This approach, often referred to as a triple-blind design37, was taken to minimize the cognitive biases that have recently been shown to be pervasive in scientific data acquisition and analysis74.
Treatment characteristics
Following the protocols of previous procedures, we used expectation-inducing verbal instructions with the purpose of manipulating the uncertainty about the declared effectiveness of the stimulation22,38. We implemented a low-uncertainty (LU) and a high-uncertainty (HU) condition. In the LU condition, participants were given the information that they would receive a combined stimulation of both tDCS and tNILS that had previously been shown to be an effective intervention to improve human cognition. In the HU condition, participants were informed that they would receive a tDCS intervention whose effect was not yet experimentally proven.
We used different treatment characteristics in the HU and LU conditions. Sham tDCS was used in the HU while both sham tDCS and an inactive tNILS device were used in the LU. For tNILS, four inactive laser needles were selected, a fact unknown both to the operator and to the participants. The laser needles were carefully focused on the left DLPFC, and were fixed using a metal crown during the stimulation period and removed afterwards. In addition, the operator was required to wear goggles as protection from the “laser beam”, while the participants were asked to close their eyes during the stimulation. Participants received only sham tDCS in both treatment conditions (HU, LU). The anodal electrode was placed over the F3 location corresponding to the left dorsolateral prefrontal cortex (DLPFC), the cathode over the F4 location corresponding to the right DLPFC. The stimulation current was 1 mA following the fade in (15 s), short stimulation (30 s) fade out (15 s) approach46. With this procedure, the stimulation-induced cutaneous sensations were physically equivalent in the LU and HU conditions. Therefore, any difference in performance change detected between the two conditions cannot be explained by different stimulation setups.
The rationale for the different treatment characteristics was first to provide different conditions for the repeated-measures design both for the participants and the operator, and second, to avoid the possibility that participants or the operator might encounter earlier scientific publications on the effect of tDCS on cognitive functions that were in contradiction to the LU condition, when only sham tDCS would have been applied in that condition. Third, as the actively operating tNILS can induce qualitatively and quantitatively different cutaneous sensations, we decided to use only the sham tDCS protocol in both conditions as an active sham stimulation, in order to keep stimulation- generated cutaneous sensation constant between the sessions. Thus, the different treatment characteristics for the HU and LU conditions (tDCS + tNILS vs. tDCS only), were necessary due to the triple-blind nature of the study design, as operator blindness could not have been maintained under a full randomization of the stimulation devices.
Paradigm
A probabilistic learning and decision-making task was used, which is a well-characterized task in humans39,41,42. It consists of a learning phase and a subsequent decision-making phase (see Fig. 1). During the learning phase, participants are repeatedly presented with three pairs (AB, CD and EF) of Chinese characters42. The participants’ task was to learn to choose the better option from a pair by trial and error. After each decision, the participants received feedback, and unknown to the participants, each symbol was probabilistically associated with reward (A – 80%, B – 20%; C – 70% D – 30%; E – 60% and F – 40%). The learning phase consisted of six experimental blocks; each block containing 20 repetitions of AB, CD and EF pairs in a random order. The presentation of each symbol pair was counterbalanced for the left and right side for each pair in each block (i.e., AB or BA).
Each trial started with a fixation cross (0.3), which was followed by the presentation of the symbol pair. Participants had a maximum of 1.7 s to respond, after which their choice was highlighted (0.5 s), and followed by the feedback (0.5 s). Each trial lasted for 3.5 s. In order to keep the motivational level constant between the treatment conditions, the participants were informed that they would receive 5 EUR per every started hour, plus 0.01 EUR after each correct decision (indicated by a green smiley face and a 0.01 EUR sign) or 0 EUR after an incorrect response (red, sad face and 0 EUR sign) or after a missed response (yellow confused face and the word ‘late’ in German). The test phase consisted of decisions involving all 15 possible combinations of the symbols; 12 new ones that were not presented during learning (e.g., AC or BF) as well as the three “old” combinations (AB, CD and EF). The symbol pairs were repeated 12 times resulting in a total of 180 decisions, and each symbol pair was counterbalanced for left and right side presentation. No feedback was provided during the testing phase, but the participants were informed that they would receive 0.01 EUR after each correct decision.. Taken together, in all three conditions (baseline, LU and HU), participants were motivated equally by performance-dependent financial remuneration. This procedure ensured that participants’ goal was to maximize their financial earnings.
After completing the final experimental session, the participants were informed about the amount of the financial compensation for their time and their additional earnings during the experiment. However, unknown to both participants and the operator, the final amount of the reimbursement was individually calculated according to 8.5 EUR per every started hour.
Data analytic strategy
For data analysis, we only used Bayesian methods because of their many advantages compared to traditional null-hypothesis testing in general48,49 and in particular because they allow a hierarchical integration of the computational reinforcement-learning model50. We report our results in terms of posterior mean and the 95% highest-density intervals (HDIs), which give the range in which the estimated parameter is located with probability 0.95.
Model-fitting
All reported models were fitted using Hamiltonian Monte-Carlo (HMC) techniques. We sampled from the joint posterior distribution of the parameters given the model using the HMC algorithms implemented in the Stan software75,76,77. All fits used eight parallel chains, each with a warm-up period of 1000 samples. Chains were initialized at random values and we sampled 1000 samples from each of the converged chains. We used no thinning as this was not deemed necessary by visual inspection of the chains and autocorrelation statistics. Resulting samples for each individual variable were visually inspected for convergence to ensure good mixing behaviour. We also applied the Gelman-Rubin diagnostic78 and ensured that all reported results had  . We used the Watanabe information criterion (WAIC) which resolves several of the difficulties of the deviance information criterion79,80,81. Differences in WAIC larger than 10 can be considered strong82.
. We used the Watanabe information criterion (WAIC) which resolves several of the difficulties of the deviance information criterion79,80,81. Differences in WAIC larger than 10 can be considered strong82.
Analysis of performance data
We analysed learning performance by submitting the accuracy data from the learning part of the experiment to a Bayesian hierarchical logistic regression model. We included trial number, condition (baseline; low-expectancy, LU; high-expectancy, HU; dummy-coded) and pair number (1, 2, 3; coded numerically) as predictors and let the intercept vary by subject. Specifically, the accuracy in trial t for subject i was modeled as

where the intercepts were constrained by a group-level distribution

Non-informative (uniform) priors were placed on all variables. In words, the probability to respond correctly in a given trial was modeled as a function of the number of the current trial (because we expect performance to increase over the experiment as the subject learns the correct mapping), the pair number (the pairs had different reward probabilities and pairs with lower reward probabilities should therefore be harder to learn), the condition (reflecting potential placebo effects of the inert intervention) and the intercept accounting for between-subject variation in learning efficiency.
A similar analysis, using the same set of predictors, was applied to the reaction times (RTs). Specifically, the model was

where the intercepts were constrained by a group-level distribution

Non-informative (uniform) priors were placed on all variables. We used log-transformed reaction times because reaction times commonly have a non-normal distribution with a steep front and long tails, and are more appropriately modeled by a log-normal distribution83 but the results are qualitatively similar for non-transformed RTs.
Analysis of subjective measures
In both experimental conditions, the participants were asked to anticipate whether the (inert) stimulation would improve, impair or not affect their performance relative to the baseline task. Similarly, they were asked immediately after the task whether they felt that their performance had been impaired, improved or not affected. We subjected the resulting categorical data for the anticipated and experienced effect of the stimulation for subject i to a softmax-regression model49:

where conditionHU is an indicator variable which is 0 in the LU condition and 1 in the HU condition, questionExp is the indicator variable for the two different questions (anticipated vs. experienced change in performance; 0 = Anticipated, 1 = Experienced) and β is a 4 × 3 matrix of parameters (intercept, condition, question, condition × question vs. decline, neutral, improve). We set “neutral” as reference category and fix  to make the parameter set identifiable. The softmax-function for a vector θ is defined as
to make the parameter set identifiable. The softmax-function for a vector θ is defined as

and yields a vector p = (pdecline, pneutral, pimprove) whose components are constrained to sum to one and represent the probabilites for each category.
To exclude the possibility that our results reflect the effect of a general arousal due to the presence of an intervention rather than a genuine placebo effect, we asked our participants to rate their arousal before and after each experimental session. The rating was done on an 11-point Likert scale where 0 indicated very tired and 10 fully awake. We submitted the resulting data to a Bayesian hierarchical linear regression model with condition (baseline, LU, HU) and time (before vs. after) and their interaction as variables:

where the intercepts were constrained by a group-level distribution

Here, “LU”, “HU”, and “after” are indicator variables that are 0 or 1 depending on the condition and time. In addition, j[i] indicates from which subject datapoint i was recorded. Non-informative (uniform) priors were placed on all parameters.
Reinforcement-learning model
We used a fully Bayesian hierarchical modeling approach for fitting the QLearning model to the individual data. This approach has been successfully used previously in fitting reinforcement-learning models50 and is superior to classical, maximum-likelihood based inference for a number of reasons see, e.g., ref. 49: Firstly, it includes the likelihood of the data of all subjects in all conditions under a single comprehensive model. This allows for a very flexible choice of distributional assumptions and dependencies of the parameters. Second, the hierarchical structure enables a “partial pooling” of the individual estimates, resulting in more stable estimates48.
We implemented a standard QLearning model39,84. The accuracy data for each trial  of subject i was modeled as as
of subject i was modeled as as

where the n-vector pi ∈ {1, 2, 3}n indicates the number of the pair that was shown to subject i in each trial and ri ∈ {0, 1}n is the vector indicating whether or not the subject received a reward in each trial (0-no reward, 1-reward present). The two parameters α and β are the learning rate and softmax-noise parameter, respectively. The learning-rate α influences the likelihood of the model by accumulating the expected value of all stimuli s ∈ {A, B, C, D, E, F} in the so-called Q-values

where t indexes trials  . Here, r(t) − Qs(t) is the so-called prediction error and is slowly integrated into the general estimated reward-probability depending on the size of the learning-rate α ∈ [0, 1]. To account for uncertainty in the choice-reward mapping, the actual choice in the model is done probabilistically as well, where option A is chosen over option B in trial t with probability
. Here, r(t) − Qs(t) is the so-called prediction error and is slowly integrated into the general estimated reward-probability depending on the size of the learning-rate α ∈ [0, 1]. To account for uncertainty in the choice-reward mapping, the actual choice in the model is done probabilistically as well, where option A is chosen over option B in trial t with probability

This is the so-called soft-max rule where the uncertainty in making a choice (or “noise”) is captured in the inverse-temperature parameter β. The likelihood is calculated as the product of these probabilities for each trial.
For each participant i, separate parameters αi and βi are estimated and they are constrained by group-level distributions

and

We were mainly interested in how our placebo manipulation would affect the model parameters and we therefore modeled the influence of the manipulation by adding them as fixed effects to the individual parameters:

where LUi and HUi are indicator variables specifying whether the current dataset i (iterating over the subject × condition space) was acquired in condition LU or HU, respectively. Similarly,

For a fully Bayesian approach, we had to specify prior distributions to the group-level parameters {μα, μβ, σα, σβ, δα,LU, δα,HU, δβ,LU, δβ,HU}. We assigned mildly informative priors to the parameters such that the parameter estimates were allowed to vary across a large number of parameter values while constraining them to a plausible range48,85. The results were robust to the choice of prior. During the model fitting, we experimented with different “degrees of non-informativeness” by changing the standard-deviation and limits of the prior distributions but the results were unchanged. Concretely, the reported analyses used the following prior

where θ ∈ {α, β} and c ∈ {LU, HU}.
As discussed above, we implemented a model where separate learning rates for learning from gains and learning from losses were estimated39 as learning from positive and negative outcomes appears to be implemented in by different sectors of striatal neurons. Concretely, equation (1) becomes

where [x]+ is x if positive and 0 otherwise and [x]− is x if negative and 0 otherwise. All other elements of the hierarchical model (including the prior) remained identical, except that all group-level distributions and effects were calculated for αG, αL and β independently.
Additional Information
How to cite this article: Turi, Z. et al. Placebo Intervention Enhances Reward Learning in Healthy Individuals. Sci. Rep. 7, 41028; doi: 10.1038/srep41028 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Buzsáki, G. Rhythms of the Brain (Oxford University Press, USA, 2006).
Sober, E. Black Box Inference: When Should Intervening Variables Be Postulated? British Journal for the Philosophy of Science 49, 469–498 (1998).
Paulus, W. Transcranial electrical stimulation (tES − tDCS; tRNS, tACS) methods. Neuropsychological Rehabilitation: An International Journal 21, 37–41 (2011).
Ridding, M. & Rothwell, J. Is there a future for therapeutic use of transcranial magnetic stimulation? Nature Reviews Neuroscience 8, 559–567 (2007).
Rossi, S. et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clinical Neurophysiology 120, 2008–2039 (2009).
O’Connell, N. E. et al. Rethinking clinical trials of transcranial direct current stimulation: participant and assessor blinding is inadequate at intensities of 2 mA. PloS One 7, e47514 (2012).
Chew, T., Ho, K.-A. & Loo, C. Inter- and intra-individual variability in response to transcranial direct current stimulation (tDCS) at varying current intensities. Brain Stimulation 8, 1130–1137 (2015).
López-Alonso, V., Cheeran, B., Ro-Rodrguez, D. & Fernández-Del-Olmo, M. Inter-individual variability in response to non-invasive brain stimulation paradigms. Brain Stimulation 7, 372–380 (2014).
Wiethoff, S., Hamada, M. & Rothwell, J. Variability in response to transcranial direct current stimulation of the motor cortex. Brain Stimulation 7, 468–475 (2014).
Colloca, L. & Miller, F. How placebo responses are formed: a learning perspective. Philosophical transactions of the Royal Society of London. Series B, Biological sciences 366, 1859–1869 (2011).
Colagiuri, B., Schenk, L., Kessler, M., Dorsey, S. & Colloca, L. The placebo effect: From concepts to genes. Neuroscience 307, 171–90 (2015).
Finniss, D., Kaptchuk, T., Miller, F. & Benedetti, F. Biological, clinical, and ethical advances of placebo effects. The Lancet 375, 686–95 (2010).
Peciña, M. & Zubieta, J. Molecular Mechanisms of Placebo Responses in Humans. Molecular Psychiatry 20, 416–423 (2015).
de la Fuente-Fernández, R. et al. Expectation and dopamine release: mechanism of the placebo effect in Parkinson’s disease. Science 293, 1164–6 (2001).
de la Fuente-Fernández, R., Schulzer, M. & Stoessl, A. Placebo mechanisms and reward circuitry: clues from Parkinson’s disease. Biological Psychiatry 56, 67–71 (2004).
Schultz, W. Getting formal with dopamine and reward. Neuron 36, 241–63 (2002).
Schönberg, T., Daw, N., Joel, D. & O’Doherty, J. Reinforcement learning signals in the human striatum distinguish learners from nonlearners during reward-based decision making. The Journal of Neuroscience 27, 12860–7 (2007).
Wise, R. Roles for nigrostriatal-not just mesocorticolimbic-dopamine in reward and addiction. Trends in Neurosciences 32, 517–524 (2009).
Lee, D., Seo, H. & Jung, M. Neural basis of reinforcement learning and decision making. Annual Review of Neuroscience 35, 287–308 (2012).
de la Fuente-Fernández, R. et al. Dopamine release in human ventral striatum and expectation of reward. Behavioral Brain Research 136, 359–363 (2002).
Scott, D. et al. Placebo and nocebo effects are defined by opposite opioid and dopaminergic responses. Archives of General Psychiatry 65, 220–31 (2008).
Lidstone, S. et al. Effects of expectation on placebo-induced dopamine release in Parkinson disease. Archives of General Psychiatry 67, 857–65 (2010).
Peciña, M., Stohler, C. & Zubieta, J. Neurobiology of placebo effects: Expectations or learning? Social Cognitive and Affective Neuroscience 9, 1013–1021 (2014).
Schmidt, L., Braun, E., Wager, T. & Shohamy, D. Mind matters: placebo enhances reward learning in Parkinson’s disease. Nature Neuroscience 17, 1793–1797 (2014).
Redgrave, P. et al. Goal-directed and habitual control in the basal ganglia: implications for Parkinson’s disease. Nature Reviews Neuroscience 11, 760–772 (2010).
Reardon, S. Performance boost paves way for ‘brain doping’. Nature News 531, 283–284 (2016).
Wexler, A. The practices of do-it-yourself brain stimulation: implications for ethical considerations and regulatory proposals. Journal of Medical Ethics 42, 211–215 (2016).
Kaptchuk, T. J. et al. Sham device versus inert pill: randomised controlled trial of two placebo treatments. BMJ (Clinical research ed.) 332, 391–7 (2006).
Chung, H. et al. The Nuts and Bolts of Low-level Laser (Light) Therapy. Annals of Biomedical Engineering 40, 516–533 (2012).
Konstantinovic, L. et al. Transcranial application of near-infrared low-level laser can modulate cortical excitability. Lasers in Surgery and Medicine 45, 648–653 (2013).
Hashmi, J. et al. Role of low-level laser therapy in neurorehabilitation. PM R 2, S292–S305 (2010).
Chaieb, L., Antal, A., Masurat, F. & Paulus, W. Neuroplastic effects of transcranial near-infrared stimulation (tNIRS) on the motor cortex. Frontiers in Behavioral Neuroscience 9, 1–8 (2015).
Colagiuri, B. Participant expectancies in double-blind randomized placebo-controlled trials: potential limitations to trial validity. Clinical Trials 7, 246–255 (2010).
Kirsch, I. & Weixel, L. Double-blind versus deceptive administration of a placebo. Behavioral Neuroscience 102, 319–323 (1988).
Rief, W. & Glombiewski, J. The hidden effects of blinded, placebo-controlled randomized trials: An experimental investigation. Pain 153, 2473–2477 (2012).
Sinyor, M. et al. Does inclusion of a placebo arm influence response to active antidepressant treatment in randomized controlled trials? Results from pooled and meta-analyses. Journal of Clinical Psychiatry 71, 270–279 (2010).
Friedman, L. M., Furberg, C., DeMets, D. L., Reboussin, D. M. & Granger, C. B. Fundamentals of clinical trials vol. 4 (Springer, 2010).
De Pascalis, V., Chiaradia, C. & Carotenuto, E. The contribution of suggestibility and expectation to placebo analgesia phenomenon in an experimental setting. Pain 96, 393–402 (2002).
Frank, M., Moustafa, A., Haughey, H., Curran, T. & Hutchison, K. Genetic triple dissociation reveals multiple roles for dopamine in reinforcement learning. Proceedings of the National Academy of Sciences of the United States of America 104, 16311–6 (2007).
Frank, M., Seeberger, L. & O’Reilly, R. By carrot or by stick: cognitive reinforcement learning in parkinsonism. Science 306, 1940–3 (2004).
Jocham, G., Klein, T. a. & Ullsperger, M. Dopamine-mediated reinforcement learning signals in the striatum and ventromedial prefrontal cortex underlie value-based choices. The Journal of Neuroscience 31, 1606–13 (2011).
Klein, T. et al. Genetically determined differences in learning from errors. Science 318, 1642–5 (2007).
O’Doherty, J. et al. Dissociable roles of ventral and dorsal striatum in instrumental conditioning. Science 304, 452–4 (2004).
Pessiglione, M., Seymour, B., Flandin, G., Dolan, R. J. & Frith, C. D. Dopamine-dependent prediction errors underpin reward-seeking behaviour in humans. Nature 442, 1042–5 (2006).
Rutledge, R., Lau, B., Myers, C. & Gluck, M. Dopaminergic drugs modulate learning rates and perseveration in Parkinson’s patients in a dynamic foraging task. The Journal of Neuroscience 29, 15104–14 (2009).
Ambrus, G. et al. The fade-in–short stimulation–fade out approach to sham tDCS–reliable at 1 mA for nave and experienced subjects, but not investigators. Brain Stimulation 5, 499–504 (2012).
Turi, Z. et al. When size matters: large electrodes induce greater stimulation-related cutaneous discomfort than smaller electrodes at equivalent current density. Brain Stimulation 7, 460–7 (2014).
Gelman, A. et al. Bayesian Data Analysis, Third Edition. Chapman & Hall/CRC Texts in Statistical Science (Taylor & Francis, 2013).
Kruschke, J. Doing Bayesian data analysis: A tutorial introduction with R (Academic Press, 2010).
Steingroever, H., Wetzels, R. & Wagenmakers, E.-J. Validating the pvl-delta model for the iowa gambling task. Frontiers in Psychology 4 (2013).
Shen, W., Flajolet, M., Greengard, P. & Surmeier, D. Dichotomous dopaminergic control of striatal synaptic plasticity. Science 321, 848–851 (2008).
Hróbjartsson, A. & Gotzsche, P. C. Is the placebo powerless? Update of a systematic review with 52 new randomized trials comparing placebo with no treatment. Journal of Internal Medicine 256, 91–100 (2004).
Keitel, A., Ferrea, S., Südmeyer, M., Schnitzler, A. & Wojtecki, L. Expectation modulates the effect of deep brain stimulation on motor and cognitive function in tremor-dominant Parkinson’s disease. PLoS One 8, 18–21 (2013).
Keitel, A. et al. Motor and cognitive placebo-/nocebo-responses in Parkinson’s disease patients with deep brain stimulation. Behavioural Brain Research 250, 199–205 (2013).
Colagiuri, B. & Boakes, R. Perceived treatment, feedback, and placebo effects in double-blind RCTs: an experimental analysis. Psychopharmacology 208, 433–441 (2010).
Colagiuri, B., Livesey, E. & Harris, J. Can expectancies produce placebo effects for implicit learning? Psychonomic Bulletin & Review 18, 399–405 (2011).
Schwarz, K. & Büchel, C. Cognition and the Placebo Effect – Dissociating Subjective Perception and Actual Performance. Plos One 10, e0130492 (2015).
Foroughi, C., Monfort, S., Paczynski, M., McKnight, P. & Greenwood, P. Placebo effects in cognitive training. Proceedings of the National Academy of Sciences 201601243 (2016).
Nitsche, M. & Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. Journal of Physiology 527, 633–639 (2000).
Ambrus, G., Paulus, W. & Antal, A. Cutaneous perception thresholds of electrical stimulation methods: comparison of tDCS and tRNS. Clinical Neurophysiology 121, 1908–14 (2010).
Fertonani, A., Ferrari, C. & Miniussi, C. What do you feel if I apply transcranial electric stimulation? Safety, sensations and secondary induced effects. Clinical Neurophysiology 126, 2181–2188 (2015).
Navratilova, E. & Porreca, F. Reward and motivation in pain and pain relief. Nature Neuroscience 17, 1304–1312 (2014).
Brown, C., Seymour, B., Boyle, Y., El-Deredy, W. & Jones, A. Modulation of pain ratings by expectation and uncertainty: Behavioral characteristics and anticipatory neural correlates. Pain 135, 240–250 (2008).
Benedetti, F. et al. Conscious expectation and unconscious conditioning in analgesic, motor, and hormonal placebo/nocebo responses. The Journal of Neuroscience 23, 4315–4323 (2003).
Benedetti, F., Amanzio, M., Rosato, R. & Blanchard, C. Nonopioid placebo analgesia is mediated by CB1 cannabinoid receptors. Nature Medicine 17, 1228–30 (2011).
Diederich, N. J. & Goetz, C. G. The placebo treatments in neurosciences: New insights from clinical and neuroimaging studies. Neurology 71, 677–84 (2008).
Wrobel, N., Wiech, K., Forkmann, K., Ritter, C. & Bingel, U. Haloperidol blocks dorsal striatum activity but not analgesia in a placebo paradigm. Cortex 57, 60–73 (2014).
Aslaksen, P., Zwarg, M., Eilertsen, H., Gorecka, M. & Bjorkedal, E. Opposite effects of the same drug: reversal of topical analgesia by nocebo information. Pain 156, 39–46 (2015).
Dreher, J.-C. et al. Menstrual cycle phase modulates reward-related neural function in women. Proceedings of the National Academy of Sciences of the United States of America 104, 2465–70 (2007).
Klosterhalfen, S. et al. Gender and the nocebo response following conditioning and expectancy. Journal of Psychosomatic Research 66, 323–328 (2009).
Aslaksen, P., Bystad, M., Vambheim, S. & Flaten, M. Gender differences in placebo analgesia: event-related potentials and emotional modulation. Psychosomatic Medicine 73, 193–199 (2011).
Andani, E., Tinazzi, M., Corsi, N. & Fiorio, M. Modulation of Inhibitory Corticospinal Circuits Induced by a Nocebo Procedure in Motor Performance. PLoS One 10, e0125223 (2015).
Peciña, M. et al. Personality trait predictors of placebo analgesia and neurobiological correlates. Neuropsychopharmacology 38, 639–46 (2013).
Nuzzo, R. How scientists fool themselves – and how they can stop. Nature News 526, 182 (2015).
Hoffman, M. D. & Gelman, A. The no-U-turn sampler: Adaptively setting path lengths in Hamiltonian Monte Carlo. arXiv 1111 (2011).
Stan Development Team. Stan Modeling Language Users Guide and Reference Manual, Version 2.5.0 (2014).
Stan Development Team. Stan: A c++ library for probability and sampling, version 2.5.0 (2014).
Gelman, A. & Rubin, D. B. Inference from iterative simulation using multiple sequences. Statistical science 457–472 (1992).
Watanabe, S. A widely applicable bayesian information criterion. The Journal of Machine Learning Research 14, 867–897 (2013).
Gelman, A., Hwang, J. & Vehtari, A. Understanding predictive information criteria for bayesian models. Statistics and Computing 24, 997–1016 (2014).
Vehtari, A., Gelman, A. & Gabry, J. Efficient implementation of leave-one-out cross-validation and waic for evaluating fitted bayesian models arXiv, preprint arXiv:1507.04544 (2015).
Pratte, M. S. & Rouder, J. N. Assessing the dissociability of recollection and familiarity in recognition memory. J Exp Psychol Learn 38, 1591 (2012).
Ratcliff, R. & Murdock, B. B. Retrieval processes in recognition memory. Psychological Review 83, 190 (1976).
Turi, Z. et al. Transcranial direct current stimulation over the left prefrontal cortex increases randomness of choice in instrumental learning. Cortex 63, 145–154 (2015).
Gelman, A. & Shalizi, C. R. Philosophy and the practice of bayesian statistics. Brit J Math Stat Psy 66, 8–38 (2013).
Acknowledgements
The authors wish to thank Dr. Dezső Németh, Dr. Gábor Csifcsák and Dr. Per M. Aslaksen for comments and helpful discussions and Dr. Caspar Stephani for the neurological examinations. The authors wish to thank to Sophie Alexandra Schäfer for the data collection and Christine Crozier who assisted in the proof-reading of the manuscript. This study was supported by the DFG (PA 419/15-1) awarded to WP.
Author information
Authors and Affiliations
Contributions
Conceptualization: Z.T.; Methodology: Z.T., Software: Z.T. (experimental paradigm) and M.M. (data analysis); Formal Analysis: M.M.; Resources: W.P. and A.A.; Data Curation: Z.T. and M.M.; Writing – Original Draft: Z.T., M.M., W.P. and A.A.; Visualization: M.M. and Z.T.; Supervision: Z.T., M.M. and A.A.; Project Administration: Z.T. and A.A.; Funding Acquisition: W.P. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Turi, Z., Mittner, M., Paulus, W. et al. Placebo Intervention Enhances Reward Learning in Healthy Individuals. Sci Rep 7, 41028 (2017). https://doi.org/10.1038/srep41028
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep41028
This article is cited by
-
Investigating the Effects of tDCS on Visual Orientation Discrimination Task Performance: “the Possible Influence of Placebo”
Journal of Cognitive Enhancement (2020)
-
Efficacy of tRNS and 140 Hz tACS on motor cortex excitability seemingly dependent on sensitivity to sham stimulation
Experimental Brain Research (2019)
-
Evidence for Cognitive Placebo and Nocebo Effects in Healthy Individuals
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
