
Abstract
Several meta-analyses comparing early functional rehabilitation and traditional immobilization following surgical Achilles tendon repair after acute rupture have been published. However, they have led to conflicting conclusions. The aims of this systematic review were to select high-quality meta-analyses from multiple discordant meta-analyses and to provide a postoperative rehabilitation strategy following surgical repair using currently available evidence. We performed a comprehensive search using the PubMed and Embase databases and the Cochrane Library. Assessment of Multiple Systematic Reviews (AMSTAR) instrument was used to assess the methodological quality. Three investigators independently applied the Jadad decision algorithm. Their results were then compared to ensure selection of a meta-analysis that provided the highest quality of evidence. Six meta-analyses met the eligibility criteria. AMSTAR scores ranged from 6 to 10. According to the Jadad decision algorithm, a high-quality meta-analysis with a greater number of RCTs was selected. This meta-analysis showed that early functional rehabilitation was superior to cast immobilization in terms of patient satisfaction and the time to return to pre-morbid sporting levels. There were no differences regarding major complications or the time before return to prior employment and sporting activity. Thus, we recommend early functional rehabilitation as the postoperative strategy for acute Achilles tendon ruptures.
Similar content being viewed by others

Introduction
Ruptures of the Achilles tendon are common, with an overall incidence of 18 per 100,000 per year1. Although conservative treatment has its advantages, surgical intervention appears to be the available method for athletes and young people2. Traditionally, surgical management of acute Achilles tendon rupture was combined with ankle immobilization for 6 weeks. This remained the standard approach until the late 1980s2,3,4.
Postoperative functional rehabilitation after Achilles tendon repair has been increasingly discussed during recent years5. The traditional rehabilitation protocol has involved rigid cast immobilization, usually in a below-knee non-weight bearing rigid cast for six weeks, followed by mobilization of the ankle joint and strengthening exercises2,3. However, initial clinical trials6,7 using early postoperative ankle mobilization and functional rehabilitation showed a low rate of re-rupture. Subsequently, multiple authors reported numerous randomized controlled trials (RCTs)7,8,9,10,11,12,13 to compare early functional rehabilitation with cast immobilization. Based on the proliferation of RCTs, several systematic reviews and meta-analyses14,15,16 were published. However, they have led to conflicting conclusions. The best postoperative rehabilitation strategy for acute Achilles tendon rupture remains a topic of debate.
The aims of this systematic review were as follows: (1) to conduct a systematic review of meta-analyses comparing early functional rehabilitation and traditional immobilization following surgical Achilles tendon repair after acute rupture; (2) to select high-quality meta-analyses among multiple discordant meta-analyses; and (3) to provide a postoperative rehabilitation strategy following surgical repair using currently available evidence.
Materials and Methods
We performed this systematic review in accordance with the PRISMA guidelines17.
Literature Search
We conducted a comprehensive search using the PubMed and Embase databases and the Cochrane Library. The following keywords were used: ((((Achilles tendon) OR Achilles) OR tendoachilles)) AND ((((rupture) OR injury) OR lesion) OR tear). We limited the article types to meta-analyses or systematic reviews. The selected articles were from the English literature. The search was performed on December 27, 2015. The references of the included studies were also manually searched such that no meta-analyses were missed. Furthermore, we manually searched the following journal contents from the past 3 years for any additional studies: The Journal of Bone and Joint Surgery, The British Journal of Sports Medicine, The Bone and Joint Journal, and The American Journal of Sports Medicine.
Eligibility Criteria
We identified meta-analyses/systematic reviews comparing early functional rehabilitation with traditional immobilization following surgical Achilles tendon repair after acute rupture. The exclusion criteria were as follows: (1) narrative review without a reported and organized search algorithm; (2) meta-analysis that included non-RCTs; (3) systematic review that did not perform a meta-analysis; and (4) meta-analysis without clinical outcome data.
Selection of Studies
Full-text articles for studies meeting eligibility criteria were selected. Two investigators independently extracted information from each included study. The following information was extracted for the included meta-analyses: journal of publication, levels of evidence, primary author, date of literature search and publication, eligibility criteria, search database, design of primary studies, number of primary RCTs, software use, performance of heterogeneity analysis, sensitivity or subgroup analysis and conflicts of interest. Outcome data were also extracted, such as ankle function, patient satisfaction and adverse events.
Assessment of Methodological Quality
Two authors independently assessed the methodological quality of the included studies. We assessed the risk of bias using the Assessment of Multiple Systematic Reviews (AMSTAR) instrument. This instrument provides 11 categories for evaluating meta-analyses/systematic reviews according to the quality of their reporting and methodology18. We also graded meta-analysis quality using The Oxford Evidence-based Medicine Levels of Evidence19.
Application of the Jadad Decision Algorithm
We interpreted and selected the discordant meta-analyses using the Jadad decision algorithm20, which is a useful tool to differentiate overlapping systematic reviews/meta-analyses. The Jadad Decision Algorithm20 was designed based on following questions: (1) Do the meta-analyses ask the same question? (2) Do the meta-analyses include the same studies? (3) Do the meta-analyses containing the same trials have the same methodologic quality? (4) Do the discordant meta-analyses including different trials use the same selection criteria20? Three investigators independently applied this algorithm, and their results were then compared to ensure selection of the meta-analysis that provided the highest quality of evidence to develop recommendations for a postoperative rehabilitation strategy after surgical repair.
Results
Search Results
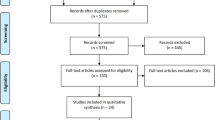
We initially identified 274 abstracts. Six studies14,15,16,21,22,23 met the eligibility criteria and were included. A flow diagram is shown in Fig. 1. These studies were published between 2004 and 2016. Three15,21,23 of them were published within the past two years (Table 1). All of the studies performed a meta-analysis. Thirteen RCTs were included in the various meta-analyses. The number of trials cited in the meta-analyses ranged from 5 to 10, with a median of seven primary RCTs cited (Table 2). The number of included patients ranged from 273 to 570, with an average of 377 patients per study.

Flow diagram summarizing the selection process of meta-analyses.
Search Methodology
All studies comprehensively searched databases. Each meta-analysis used at least four different databases to research RCTs. All studies included meta-analyses searched from PubMed or Medline, Embase and the Cochrane Library. There was heterogeneity among the other databases that were used. Details of the search methodology are summarized in Table 3.
Study Quality and Validity
Only RCTs were included for all meta-analyses. The AMSTAR scores were assessed for the included meta-analyses and ranged from 6 to 10 points, with a median of 7.3 points (with the maximum possible score of 11 points). One Cochrane Review22 was assessed as the best-quality study. The AMSTAR score for each meta-analysis is shown in Table 4. According to the Oxford Levels of Evidence, three meta-analyses15,16,22 were assessed as Level I evidence, and four studies14,21,23 were assessed as Level II evidence (Table 5).
Heterogeneity Assessment
Statistical heterogeneity was assessed in each included meta-analysis using the I2 statistic value. Revman software was used for all meta-analyses (Table 5). Only one meta-analysis23 performed subgroup analyses. Five other meta-analyses14,15,16,21,22 did not perform sensitivity or subgroup analyses (Table 5).
Results of the Jadad Decision Algorithm
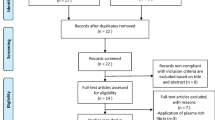
Three authors independently selected the same flow path according to the Jadad decision algorithm. Because (1) all included meta-analyses analysed the same question (comparing early functional rehabilitation with traditional immobilization following surgical Achilles tendon repair after acute rupture), (2) the included meta-analyses did not include the same RCTs, and (3) they did not have the same selection criteria, we selected the highest-quality meta-analysis based on the following factors: publication status of the primary studies, methodology of the primary studies, language restrictions and the analysis of data on individual patients. None of the eligible meta-analyses stated a restriction on the publication status of primary studies. Regarding the methodology of primary studies, all meta-analyses exclusively included RCTs with superior methodologies. McCormack and Bovard15 restricted the study quality using a minimum of 19 items of the Downs and Black-validated 27-item checklist24. Concerning the publication characteristics, the included meta-analyses were published over an extended period. Thus, more recent meta-analyses were preferred to less recent meta-analyses. Additionally, all meta-analyses appropriately analysed the data. Finally, three authors selected the study by McCormack and Bovard15 as the meta-analysis offering the best current evidence (Fig. 2).

Flow diagram of the Jadad decision algorithm.
McCormack and Bovard15 reported that early functional rehabilitation was superior to cast immobilization regarding patient satisfaction and the time interval of return to prior sporting level. Furthermore, they found no differences concerning major complications and the rate of return to prior employment and sporting activity in their study. Hence, they concluded that early functional rehabilitation following surgical repair of acute Achilles tendon rupture was safe and leaded to higher patient satisfaction and earlier return to function.
Discussion
Multiple RCTs9,10,11,12,13 comparing early functional rehabilitation with cast immobilization have been reported. However, they have presented conflicting findings regarding which strategy is better. Furthermore, many meta-analyses of RCTs, representing the highest grade of evidence, have been reported to compare two postoperative rehabilitation strategies. Although three meta-analyses15,21,23 comprehensively searched databases during the most recent two years, they included different RCTs and reached conflicting results. Such discordance has confused decision makers (such as policymakers, clinicians and patients) who make choices based on these meta-analyses.
The possible sources of discordant results among meta-analyses were analysed and reported by Jadad et al.20 Meanwhile, they designed a decision tool to choose high-quality evidence among discordant systematic reviews. This decision tool has been widely used to find the best available evidence among overlapping systematic reviews/meta-analyses25,26. Khan et al.22 performed a Cochrane systematic review comparing early functional rehabilitation with immobilization after surgical Achilles tendon repair. The Cochrane systematic review is internationally recognized as “the highest standard” in evidence-based health care resources and should be updated every two years to provide the most current evidence to decision makers. The Cochrane review by Khan et al.22 obtained the highest scores based on the AMSTAR instrument in the current study. However, their review was performed in 2004 and was not updated for 13 years regarding the postoperative strategy, although multiple newly available RCTs have emerged. Hence, we did not select Khan et al.22 as the best review. McCormack and Bovard15 included the maximum number of RCTs and appropriately analysed the RCT data. Hence, the McCormack and Bovard15 meta-analysis was selected to represent the best available current evidence.
McCormack and Bovard15 found that the early rehabilitation group had three times the odds of rating patient satisfaction as ‘good’ or ‘excellent’ compared to the traditional immobilization group (p = 0.01; OR, 3.13; 95% CI 1.30 to 7.53). They also reported that there were no differences concerning major complications (including tendon re-rupture, deep infection, tendon adhesions, persistent functional/neurological deficit, thrombophlebitis/compartment syndrome and wound slough) or the rate of return to prior employment and sporting activity. However, five of the six included RCTs showed that the early rehabilitation group had a shorter time interval before return to prior sporting level than the traditional immobilization group. They concluded that early functional rehabilitation resulted in higher patient satisfaction and earlier return to function, with no increase in complications15. Thus, early functional rehabilitation may contribute to evidence-based practice for postoperative management after Achilles tendon repair.
The phases of tendon healing have been divided into inflammation, proliferation and remodelling5. Throughout these phases, the tensile strength of the tendon gradually increases, although it remains inferior to the uninjured tissue. The new scar tissue is biomechanically inferior, which causes increased stiffness and subsequent visco-elastic properties27. Animal studies have demonstrated that early rehabilitation can decrease excessive adhesion formation, improve biomechanical properties of the scar tissue and subsequently enhance the gliding function of the tendon28,29. Active or passive ankle joint motion exercises can eliminate local oedema and prevent joint stiffness and the atrophy of calf muscles8. Re-rupture following surgical repair is a potential complication for early function. Many surgeons worry that early function may increase the re-rupture rate. However, the results of the current study demonstrate that early functional rehabilitation after Achilles tendon repair does not increase the re-rupture rate and also improves patient satisfaction and facilitates earlier return to activity.
Our study has several strengths. First, this study can be considered as the first systematic review of overlapping meta-analyses to evaluate the rehabilitation strategy following surgical management of acute Achilles tendon rupture. Second, our study provides high-quality evidence for a postoperative rehabilitation strategy following surgical repair based on comprehensive summarization of previously published meta-analyses on this topic. Our study is a systematic review of overlapping meta-analyses, which is used to appraise the methodological quality and quality of reporting of meta-analyses. It is different from traditional systematic reviews that analyse primary studies. In this study, we selected the best of the currently published meta-analyses and provided high-level evidence to decision makers. Hence, the results of our study have greater strength than other systematic reviews or RCTs.
There are several limitations to this systematic review. First, this systematic review was not registered on prospective registration systems for systematic reviews. Prospective registration could improve the quality of a systematic review and increase confidence in the findings. Second, the AMSTAR tool showed that the methodological quality of the included meta-analyses was low. Although we only assessed meta-analyses, including RCTs, to ensure high methodological quality, three of the studies were assessed as Level II evidence. Most included meta-analyses did not provide a priori design. Furthermore, none of them assessed the likelihood of publication bias. Third, only English language studies were researched in this systematic review. Our search strategy may have excluded non-English studies meeting eligibility criteria. Fourth, there was a clear lack of blinding in all trials, which may have influenced patient-reported outcome measures, such as patient satisfaction. However, blinding was not possible for participants and clinicians because of the nature of surgical interventions. Fifth, the surgical techniques varied between trials, which also might have presented significant residual confounding. However, we also noted that several RCTs reported no significant differences in postoperative outcomes between traditional open and minimally invasive surgery30,31,32.
In brief, this systematic review of meta-analyses concludes that early functional rehabilitation can improve patient satisfaction and facilitate earlier return to activity without increased complication rates. Thus, we recommend early functional rehabilitation as the postoperative strategy for acute Achilles tendon ruptures.
Additional Information
How to cite this article: Zhao, J.-G. et al. Early functional rehabilitation versus traditional immobilization for surgical Achilles tendon repair after acute rupture: a systematic review of overlapping meta-analyses. Sci. Rep. 7, 39871; doi: 10.1038/srep39871 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Leppilahti, J. & Orava, S. Total Achilles tendon rupture. A review. Sports Med 25, 79–100 (1998).
Maffulli, N. Rupture of the Achilles tendon. J Bone Joint Surg Am 81, 1019–1036 (1999).
Gillies, H. & Chalmers, J. The management of fresh ruptures of the tendo achillis. J Bone Joint Surg Am 52, 337–343 (1970).
Holm, C., Kjaer, M. & Eliasson, P. Achilles tendon rupture–treatment and complications: a systematic review. Scand J Med Sci Sports 25, e1–10 (2015).
Kearney, R. S. & Costa, M. L. Current concepts in the rehabilitation of an acute rupture of the tendo Achillis. J Bone Joint Surg Br 94, 28–31 (2012).
Troop, R. L. et al. Early motion after repair of Achilles tendon ruptures. Foot Ankle Int 16, 705–709 (1995).
Solveborn, S. A. & Moberg, A. Immediate free ankle motion after surgical repair of acute Achilles tendon ruptures. Am J Sports Med 22, 607–610 (1994).
Cetti, R., Henriksen, L. O. & Jacobsen, K. S. A new treatment of ruptured Achilles tendons. A prospective randomized study. Clin Orthop Relat Res, 155–165 (1994).
Suchak, A. A., Bostick, G. P., Beaupre, L. A., Durand, D. C. & Jomha, N. M. The influence of early weight-bearing compared with non-weight-bearing after surgical repair of the Achilles tendon. J Bone Joint Surg Am 90, 1876–1883 (2008).
Kangas, J., Pajala, A., Siira, P., Hamalainen, M. & Leppilahti, J. Early functional treatment versus early immobilization in tension of the musculotendinous unit after Achilles rupture repair: a prospective, randomized, clinical study. J Trauma 54, 1171–1180. discussion 1180–1171 (2003).
Kangas, J., Pajala, A., Ohtonen, P. & Leppilahti, J. Achilles tendon elongation after rupture repair: a randomized comparison of 2 postoperative regimens. Am J Sports Med 35, 59–64 (2007).
Groetelaers, R. P. et al. Functional treatment or cast immobilization after minimally invasive repair of an acute Achilles tendon rupture: prospective, randomized trial. Foot Ankle Int 35, 771–778 (2014).
Costa, M. L. et al. Randomised controlled trials of immediate weight-bearing mobilisation for rupture of the tendo Achillis. J Bone Joint Surg Br 88, 69–77 (2006).
Suchak, A. A., Spooner, C., Reid, D. C. & Jomha, N. M. Postoperative rehabilitation protocols for Achilles tendon ruptures: a meta-analysis. Clin Orthop Relat Res 445, 216–221 (2006).
McCormack, R. & Bovard, J. Early functional rehabilitation or cast immobilisation for the postoperative management of acute Achilles tendon rupture? A systematic review and meta-analysis of randomised controlled trials. Br J Sports Med 49, 1329–1335 (2015).
Khan, R. J. et al. Treatment of acute achilles tendon ruptures. A meta-analysis of randomized, controlled trials. J Bone Joint Surg Am 87, 2202–2210 (2005).
Panic, N., Leoncini, E., de Belvis, G., Ricciardi, W. & Boccia, S. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS One 8, e83138 (2013).
Shea, B. J. et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol 7, 10 (2007).
Wright, J. G., Swiontkowski, M. F. & Heckman, J. D. Introducing levels of evidence to the journal. J Bone Joint Surg Am 85-A, 1–3 (2003).
Jadad, A. R., Cook, D. J. & Browman, G. P. A guide to interpreting discordant systematic reviews. CMAJ 156, 1411–1416 (1997).
Mark-Christensen, T., Troelsen, A., Kallemose, T. & Barfod, K. W. Functional rehabilitation of patients with acute Achilles tendon rupture: a meta-analysis of current evidence. Knee Surg Sports Traumatol Arthrosc (2014).
Khan, R. J., Fick, D., Brammar, T. J., Crawford, J. & Parker, M. J. Surgical interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev, CD003674 (2004).
Huang, J. et al. Rehabilitation regimen after surgical treatment of acute Achilles tendon ruptures: a systematic review with meta-analysis. Am J Sports Med 43, 1008–1016 (2015).
Downs, S. H. & Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 52, 377–384 (1998).
Zhao, J. G., Wang, J. & Long, L. Surgical versus conservative treatments for displaced midshaft clavicular fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore) 94, e1057 (2015).
Zhao, J. G., Wang, J., Wang, C. & Kan, S. L. Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore) 94, e599 (2015).
Evans, N. A. & Stanish, W. D. The basic science of tendon injuries. Curr Orthop 14, 403–412 (2000).
Enwemeka, C. S. Functional loading augments the initial tensile strength and energy absorption capacity of regenerating rabbit Achilles tendons. Am J Phys Med Rehabil 71, 31–38 (1992).
Lin, T. W., Cardenas, L. & Soslowsky, L. J. Biomechanics of tendon injury and repair. J Biomech 37, 865–877 (2004).
Kolodziej, L., Bohatyrewicz, A., Kromuszczynska, J., Jezierski, J. & Biedron, M. Efficacy and complications of open and minimally invasive surgery in acute Achilles tendon rupture: a prospective randomised clinical study--preliminary report. Int Orthop 37, 625–629 (2013).
Gigante, A. et al. Open versus percutaneous repair in the treatment of acute Achilles tendon rupture: a randomized prospective study. Knee Surg Sports Traumatol Arthrosc 16, 204–209 (2008).
Karabinas, P. K. et al. Percutaneous versus open repair of acute Achilles tendon ruptures. Eur J Orthop Surg Traumatol 24, 607–613 (2014).
Author information
Authors and Affiliations
Contributions
J.G.Z. and S.L.K. contributed to the conception and design of the study and the critical revision of the article. J.G.Z., L.L. and X.H.M. searched and selected the studies, analysed the data, prepared figures and drafted the article. J.G.Z., Z.X.T. and S.L.K. participated in the interpretation of data. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhao, JG., Meng, XH., Liu, L. et al. Early functional rehabilitation versus traditional immobilization for surgical Achilles tendon repair after acute rupture: a systematic review of overlapping meta-analyses. Sci Rep 7, 39871 (2017). https://doi.org/10.1038/srep39871
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep39871
This article is cited by
-
Lower re-rupture rates but higher complication rates following surgical versus conservative treatment of acute achilles tendon ruptures: a systematic review of overlapping meta-analyses
Knee Surgery, Sports Traumatology, Arthroscopy (2023)
-
Modified triple Kessler with least risk of elongation among Achilles tendon repair techniques: a systematic review and network meta-analysis of human cadaveric studies
Knee Surgery, Sports Traumatology, Arthroscopy (2023)
-
A randomized controlled trial of stem cell injection for tendon tear
Scientific Reports (2022)
-
Treatment of partial injury of the calcaneus tendon with heterologous fibrin biopolymer and/or photobiomodulation in rats
Lasers in Medical Science (2022)
-
Evolving concepts in ventral hernia repair and physical therapy: prehabilitation, rehabilitation, and analogies to tendon reconstruction
Hernia (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
