
Abstract
Although the associations between carotid plaque and cardiovascular disease risk factors have been identified in previous studies, there is limited information on sex-related differences in factors associated with the development of carotid plaque. We aimed to determine sex differences in the prevalence of carotid plaque and associated risk factors in rural China. A total of 3,789 subjects aged ≥45 years without history of stroke or cardiovascular disease were recruited to the study. B-mode ultrasonography was performed to determine the presence of carotid plaque. The mean age of male subjects was greater than that of female subjects. In addition, there was a higher prevalence of carotid plaque in men than in women (50.1% vs. 35.5%; P < 0.001) irrespective of age group, education level, and presence of risk factors. Older age, hypertension, diabetes mellitus, and high concentrations of low-density lipoprotein cholesterol were pronouncedly associated with the risk of carotid plaque in both men and women. These findings suggest that it is vital for physicians to be aware that conventional risk factors and other related factors are of equal importance among rural residents in China; patients should thus be treated accordingly so that reduce the burden of stroke and cardiovascular disease.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD), including ischemic heart disease and stroke, is a leading cause of death in both developed and developing countries worldwide1. The aging and growth of populations has led to an increase in the total number of cardiovascular deaths, accounting for almost one-third of all deaths globally in 2013. Ischemic heart disease, ischemic stroke, and hemorrhagic stroke continue to cause the most cardiovascular-related and circulatory-related deaths in almost all countries2. Death due to CVD accounted for more than 40% of total deaths (44.6% in rural areas and 42.5% in urban areas) in China3. The economic burden of CVD in China between 2005 and 2015 was estimated to be approximately 550 billion USD4.
Carotid artery atherosclerosis is a strong predictor of ischemic stroke events as a result of both luminal stenosis and plaque rupture5,6. Carotid atherosclerosis has also been shown to be associated with an increased risk of CVD7,8.
Atherosclerotic plaques are prone to rupture because of their intrinsic composition, as they may have intra-plaque hemorrhaging and large lipid cores; consequently, atherosclerotic plaques are associated with subsequent thromboembolic ischemic events9,10,11. Several previous studies have indicated that carotid plaque and carotid intima-media thickening are risk factors for future CVD and cerebrovascular diseases12,13,14,15,16.
Sex-related differences are becoming increasingly recognized as potentially important factors in atherosclerosis17. Moreover, plaques in men seemed to have higher rates of erosion, ulceration, and subsequent healing18. Although associations between carotid plaque and CVD risk factors have been identified in previous studies19,20,21,22, studies on sex-related differences in risk factors associated with the development of carotid plaque are rare. Therefore, we aimed to assess sex-related differences in the prevalence of and risk factors for carotid plaque among adults aged 45 years and older in rural China.
Results
Selection of the study population and response rate
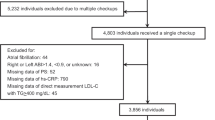
A total of 5,380 residents aged 45 years or older were qualified to participate in this study. Of these, 4,012 residents agreed to participate, resulting in a response rate of 75%. Finally, 3,789 residents participated in this study, after the exclusion of 223 residents with a previous history of CVD or stroke.
Sex differences in demographic characteristics and physical examination findings
Of the 3,789 participants in this study, 1,560 (41.2%) were men and 2,229 (58.8%) were women. Compared to women, there were more men aged 65–74 years (21.7% vs. 17.3%; P = 0.001), aged ≥75 years (10.3% vs. 7.0%; P < 0.001), and with >6 years of education (46.4% vs. 31.9%; P < 0.001). Compared to men, there were more women aged 45–54 years (36.2% vs. 27.6%; P < 0.001); moreover, women had a higher illiteracy rate (23.4% vs. 8.8%; P < 0.001). Women had greater body mass indexes and total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) concentrations than men (all P < 0.001), but systolic and diastolic blood pressure levels were greater in men than in women (P = 0.002 and P < 0.001, respectively; Table 1).
Sex differences in the prevalence of risk factors
As shown in Table 2, there was a higher prevalence of hypertension, current smoking, alcohol consumption, and low HDL-C in men, but a higher prevalence of obesity, passive smoking, high TC, high TG, and high LDL-C in women (all P < 0.001). The prevalence of diabetes mellitus was similar between men and women (P = 0.719).
Sex differences in the prevalence of carotid plaque by demographic characteristics and risk factors
The prevalence of carotid plaque was 41.5% overall (50.1% in men and 35.5% in women; P < 0.001). There was a significantly greater prevalence of carotid plaque in men than in women across risk factor groups. Moreover, the prevalence of carotid plaque was significantly higher in men than in women for every age and education group (all P < 0.05; Table 3).
Sex differences in risk factors for carotid plaque
Table 4 indicates that age, education, hypertension, diabetes mellitus, and high LDL-C concentrations were associated with the risk of carotid plaque in both men and women in the univariate analysis. Moreover, alcohol consumption was a significant risk factor for carotid plaque in men.
The multivariate analysis indicated that age, hypertension, diabetes, and high LDL-C concentrations were significantly associated with the risk of carotid plaque in both men and women. The risk of carotid plaque increased with age; the corresponding adjusted odds ratios (ORs) (95% confidence intervals [CIs]) in men were 2.55 (1.94–3.37) in the 55–64-year age group, 3.64 (2.59–5.10) in the 65–74-year age group, and 9.49 (5.83–15.44) in the ≥75-year age group; the reference was the 45–54-year age group. Moreover, individuals with hypertension, diabetes mellitus, and high LDL-C concentrations had a higher risk of carotid plaque, with adjusted ORs (95% CIs) of 1.59 (1.25–2.03) for hypertension, 1.38 (1.01–1.89) for diabetes mellitus, and 4.07 (2.30–7.22) for high LDL-C concentration in men. The corresponding ORs (95% CIs) in women were 2.62 (2.04–3.36) in the 55–64-year age group, 2.95 (2.17–4.06) in the 65–74-year age group, and 5.53 (3.61–8.47) in the ≥75-year age group; in women, adjusted ORs (95% CIs) were 1.45 (1.17–1.79) for hypertension, 1.57 (1.21–2.03) for diabetes mellitus, and 5.11 (3.39–7.70) for high LDL-C concentration (Table 5).
Discussion
This is the first population-based report of the prevalence rates of carotid plaque and relevant risk factors in a low-income population in China. We reported a carotid plaque prevalence of 41.5% overall, with a significantly higher prevalence in men (50.1%) than in women (35.5%). Age, hypertension, diabetes mellitus, and high LDL-C concentration were risk factors for carotid plaque in both men and women.
There is currently great controversy regarding the prevalence of carotid plaque, because the reported prevalence varies widely, ranging from 13.3% to 78%15,23,24,25. The Northern Manhattan Cohort Study, a population-based cohort study with a unique race/ethnicity profile, reported an overall carotid plaque prevalence of 57% among community-dwelling residents aged ≥39 years26. Similar prevalence rates were reported in other studies, with rates ranging from 47–58%15,26,27,28,29. The San Daniele Project, a population-based asymptomatic carotid atherosclerosis study in Italy, reported a lower prevalence rate of carotid plaque (13.3% in men and 13.4% in women) in 199230. The highest reported prevalence rate of carotid plaque was in Americans aged 55–80 years among Humana Health System residents in 2012; carotid plaque was identified in 78% of these individuals25. Recently, several studies have reported the prevalence of carotid plaque in Chinese populations. A lower prevalence has been reported in Hong Kong and Taiwan (14.5% and 14.3%, respectively)31,32. The prevalence of carotid plaque was reported to be 52% for working Chinese subjects aged 40 years and older24,25 and 60.3% among urban residents aged 43–81 years in Beijing33. In contrast to these two studies, we observed a lower prevalence of carotid plaque in a low-income rural population, with a rate of 41.5% overall. Ethnic diversity or socioeconomic status could partly explain these differences, although the mechanisms involved remain to be established26,34. Furthermore, variations in the definitions of carotid plaque, study designs, and age structures of the study populations may have contributed to the differences in the reported prevalence rates of carotid plaque. In addition, consistent with previous studies, we observed a higher prevalence in men than in women35,36. Estrogens play a fundamental role in most aspects of plaque growth, conferring a cardiovascular advantage in women37. Moreover, atherosclerosis in men exhibits inflammatory and histological features distinct from atherosclerosis features in women38,39. In addition, relative to the external carotid artery and to the common carotid artery, the internal carotid artery was larger in women than in men, and in relation to the inflow area, women have a larger outflow area40. Bifurcation anatomy has been implicated in the development of plaque, and sex differences in bifurcation anatomy could partly account for the sex differences in the prevalence of carotid plaque.
Although extensive research has been conducted on the associations between atherosclerotic plaque and conventional risk factors, including hypertension, diabetes mellitus, dyslipidemia, and current smoking, the relationships between conventional risk factors and carotid plaque remain controversial.
Age is considered an important risk factor for atherosclerotic plaque, and a positive relationship between the prevalence of carotid plaque and age has been reported previously. An increased prevalence of carotid plaque with increasing age has been identified in previous studies33,41,42,43,44. In China, the reported prevalence of carotid plaque was almost 70% in those aged ≥60 years and 80% in those aged ≥70 years33. In Germany, the reported prevalence of extracranial carotid artery stenosis (>50%) was approximately 6.9% in patients aged >65 years, but it increased further with age42,43. In the present study, the prevalence of carotid plaque increased with age, and there was a greater prevalence in men than in women for each age group. The reference group was individuals aged 45–54 years, and the risk of carotid plaque in men increased by 1.55-fold for those aged 55–64 years, 2.64-fold for those aged 65–74 years, and 8.49-fold for those aged 75 years and older. Similar trends were observed in women; the risk of carotid plaque increased by 1.62-fold for those aged 55–64 years, 1.95-fold for those aged 65–74 years, and 4.53-fold for those aged 75 years and older. There was a greater risk of carotid plaque in men than in women among individuals over 75 years old.
In an earlier cross-sectional investigation, low socioeconomic status was associated with an increased prevalence of atherosclerotic changes in the carotid arteries, and women with low educational levels had an increased risk of carotid artery stenosis compared to those with higher educational levels45. Individuals with less education were reported to have larger carotid plaques, even after adjusting for vascular risk factors46,47. Moreover, low socioeconomic status was associated with progression of atherosclerosis in a middle-aged population with subclinical atherosclerosis34. In this study, we noted that individuals (both men and women) with low educational levels had a greater risk of carotid plaque than did those with higher educational levels; there was an especially high prevalence of carotid plaque in illiterate women. However, the association between education level and the prevalence of carotid plaque was not significant after adjusting for other risk factors.
Traditional risk factors, including age, sex, smoking status, systolic blood pressure, diastolic blood pressure, diabetes mellitus, HDL-C concentration, and LDL-C concentration, have been reported to be associated with carotid plaque12,15,31,44,48,49,50. However, these risk factors could explain approximately 50% of the effects on the prevalence of carotid plaque in prior studies15,49,50. Our findings suggested that age, hypertension, diabetes, and LDL-C concentration were significantly associated with carotid plaque in both men and women.
There were some limitations in this study. First, the study population was from a local town in Tianjin, China, so these results may not be representative of the general Chinese population. Second, the cross-sectional design may have led to a selection bias, especially among the healthy elderly. However, excluding subjects with histories of stroke and CVD likely overcame this limitation. Moreover, all participants with carotid plaque were asymptomatic, which may have decreased bias.
Conclusions
This study was the first to report sex differences in the prevalence of carotid plaque and associated risk factors among adults aged 45 years and older in rural China. In this cross-sectional study, we assessed these sex differences among participants aged 45 years and over. There was a conspicuously higher prevalence of carotid plaque in men than in women across age groups, educational levels, and across all risk factors. Age, hypertension, diabetes mellitus, and LDL-C concentration were significantly associated with carotid plaque in both men and women. Therefore, it is vital for physicians to be aware that conventional risk factors and other related factors are of equal importance in rural residents in China; patients should be treated accordingly in order to reduce the burden of stroke and cardiovascular disease.
Materials and Methods
Participants and study design
This was a population-based cross-sectional study conducted from April 2014 to January 2015. The participants were from the Tianjin Brain Study which was described previously22,27,30,31,32. In brief, the total population included 14,251 individuals from 18 administrative villages. Approximately 95% of the populations were low-income farmers, with a per capita disposable income of <1600 USD in 201451. In 2011, the average length of education was 5.26 years. All residents aged 45 years and older without a previous history of CVD and stroke were recruited to this study, while those with a previous history of CVD and stroke were excluded.
All investigative protocols were approved by the ethics committee of Peking University First Hospital and Tianjin Medical University General Hospital; the methods were carried out in accordance with the approved guidelines, and informed consent was obtained from each participant.
Risk factors and physical examination
This study was conducted through face-to-face interviews by trained research staff. A pre-designed questionnaire was used to collect the following information: demographic information (including name, sex, date of birth, and educational level), individual and family medical history (including the presence or occurrence of hypertension, diabetes mellitus, stroke, transient ischemia attack, and coronary heart disease), and lifestyle factors (including cigarette smoking [defined as ≥1 cigarette per day for ≥1 year], passive smoking [defined as ≥1 person smoking in the room], and alcohol consumption [defined as drinking ≥500 g of alcohol per week for 1 year]).
A physical examination was performed to obtain information on blood pressure, height, and weight; the serum levels of fasting blood glucose, TC, TG, HDL-C, and LDL-C were measured. Carotid ultrasonography and 12-lead echocardiography were also performed. Body mass index was calculated as the individual’s weight (kg) divided by the square of the individual’s height (m2).
Ultrasonography measurements
One trained technician blinded to participants’ information performed all ultrasound examinations. The patients were examined while they were in the supine position using B-mode ultrasonography (Terason 3000; Burlington, MA, US) with a 5–12 MHz linear array transducer. The extracranial carotid artery trees (i.e., the common carotid artery, the bifurcation, and the internal and external carotid arteries) on both sides were screened for plaque. Images were obtained and digitally stored according to a standard protocol28. Both longitudinal and transverse dynamic images of each plaque were stored.
Definitions of risk factors
Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or taking medication for hypertension. Diabetes mellitus was defined as a fasting blood glucose concentration ≥7.0 mmol/L or taking medication for diabetes. Obesity was defined as a body mass index of ≥28.0 kg/m2, and overweight was defined as a body mass index of 24.0–27.9 kg/m2 52. High TC was defined as a TC concentration of ≥6.22 mmol/L. High TG was defined as a triglyceride value of ≥2.26 mmol/L. High LDL-C was defined as an LDL-C concentration of ≥4.14 mmol/L, and low HDL-C was defined as an HDL-C concentration of ≤1.04 mmol/L26.
Carotid plaque was defined as a focal structure encroaching into the arterial lumen by at least 0.5 mm or 50% of the surrounding intima-media thickness value, or demonstrated as a thickness of >1.5 mm from the intima-lumen interface to the media adventitia interface29. Subjects with carotid plaque were defined as those having at least one lesion overall, regardless of the actual number of carotid plaques.
Statistical analyses
Continuous variables were presented as means and standard deviations, and sex differences were compared using Student t-tests. Categorical variables were presented as numbers with frequencies, and sex differences were compared using chi-squared tests. All participants were categorized into four age groups (45–54, 55–64, 65–74, and ≥75 years) and three education groups (0, 1–6, and >6 years). The risk factors for carotid plaque were assessed individually for men and women using logistic regression analyses. Results of the univariate analysis were presented as unadjusted ORs and 95% CIs; results of the multivariate analysis were presented as adjusted ORs and 95% CIs after adjustment for covariates. Of these, age group and education group were analyzed as categorical variables, referenced as 45–54 years and >6 years, respectively; hypertension, diabetes mellitus, obesity, current smoking, passive smoking, alcohol consumption, and high TC, high TG, low HDL-C, and high LDL-C levels were analyzed as dichotomous variables. P values < 0.05, <0.0166, and <0.0125 were considered statistically significant for dichotomous variables, categorical variables with three groups, and categorical variables with four groups, respectively. SPSS for Windows (version 15.0; SPSS Inc., Chicago, IL, USA) was used for analyses.
Additional Information
How to cite this article: Zhao, W. et al. Sex Differences in Prevalence of and Risk Factors for Carotid Plaque among Adults: A Population-based Cross-Sectional Study in Rural China. Sci. Rep. 6, 38618; doi: 10.1038/srep38618 (2016).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Lloyd-Jones, D. et al. Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 119, 480–486 (2009).
Naghavi, M. et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 385, 117–171 (2015).
National Center for Cardiovascular Diseases, China. Report on Cardiovascular Diseases in China (2015) (Encyclopedia of China Publishing House, 2016).
The Ministry of Health of the People’s Republic of China: China Health Statistics Yearbook 2011 (China Union Medical University Press, 2011).
Gomez, C. R. Carotid plaque morphology and risk for stroke. Stroke. 21, 148–151 (1990).
Glagov, S. & Zarins, C. K. What are the determinants of plaque instability and its consequences? J Vasc Surg. 9, 389–390 (1989).
Hulthe, J. et al. Atherosclerotic changes in the carotid artery bulb as measured by B-mode ultrasound are associated with the extent of coronary atherosclerosis. Stroke. 28, 1189–1194 (1997).
Salonen, R. et al. Ultrasonographic manifestations of common carotid atherosclerosis in elderly eastern Finnish men: prevalence and associations with cardiovascular diseases and risk factors. Arterioscler Thromb. 14, 1631–1640 (1994).
Virmani, R., Burke, A. P., Farb, A. & Kolodgie, F. D. Pathology of the vulnerable plaque. J Am Coll Cardiol. 47, C13–18 (2006).
Virmani, R., Ladich, E. R., Burke, A. P. & Kolodgie, F. D. Histopathology of carotid atherosclerotic disease. Neurosurgery. 59, S219–227 (2006); discussion S3–13.
Virmani, R., Kolodgie, F. D., Burke, A. P., Farb, A. & Schwartz, S. M. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 20, 1262–1275 (2000).
Cao, J. J. et al. Association of carotid artery intima-media thickness, plaques, and C-reactive protein with future cardiovascular disease and all-cause mortality: the Cardiovascular Health Study. Circulation. 116, 32–38 (2007).
Lorenz, M. W., von Kegler, S., Steinmetz, H., Markus, H. S. & Sitzer, M. Carotid intima-media thickening indicates a higher vascular risk across a wide age range: prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke. 37, 87–92 (2006).
van der Meer, I. M. et al. Predictive value of noninvasive measures of atherosclerosis for incident Myo-cardial infarction: the Rotterdam Study. Circulation. 109, 1089–1094 (2004).
Kuo, F. et al. Traditional Cardiovascular Risk Factors Explain the Minority of the Variability in Carotid Plaque. Stroke. 43, 1755–1760 (2012).
Rundek, T. et al. Carotid plaque, a subclinical precursor of vascular events: the Northern Manhattan study. Neurology. 70, 1200–1207 (2008).
Shaw, L. J. et al. Women’s Ischemic Syndrome Evaluation: current status and future research directions: report of the National Heart, Lung and Blood Institute workshop: October 2–4, 2002: section 5: gender-related risk factors for ischemic heart disease. Circulation. 109, e56–e58 (2004).
Sangiorgi, G. et al. Sex-related differences in carotid plaque features and inflammation. J Vasc Surg. 57, 338–344 (2013).
Herder, M., Johnsen, S. H., Arntzen, K. A. & Mathiesen, E. B. Risk factors for progression of carotid intima-media thickness and total plaque area: a 13-year follow-up study: the Tromsø Study. Stroke. 43, 1818–1823 (2012).
van der Meer, I. M. et al. Risk factors for progression of atherosclerosis measured at multiple sites in the arterial tree: the Rotterdam Study. Stroke. 34, 2374–2379 (2003).
Chambless, L. E. et al. Risk factors for progression of common carotid atherosclerosis: the Atherosclerosis Risk in Communities Study, 1987–1998. Am J Epidemiol. 155, 38–47 (2002).
Zhan, C. et al. Prevalence and Risk Factors of Carotid Plaque Among Middle-aged and Elderly Adults in RuralTianjin, China. Sci Rep. 31, 23870 (2016).
Li, Q. et al. The Association between Serum Uric Acid Levels and the Prevalence of Vulnerable Atherosclerotic Carotid Plaque: A Cross-sectional Study. Sci Rep. 5, 10003 (2015).
Yang, X. et al. Homocysteine and Carotid Plaque Stability: A Cross-Sectional Study in Chinese Adults. PLoS ONE. 9, e94935 (2014).
Sillesen, H. et al. Carotid Plaque Burden as a Measure of Subclinical Atherosclerosis. JACC Cardiovasc Imaging. 5, 681–689 (2012).
Yang, D. et al. Cigarette Smoking and Carotid Plaque Echodensity in the Northern Manhattan Study. Cerebrovasc Dis. 40, 136–143 (2015).
Högberg, D., Kragsterman, B., Björck, M., Tjärnström, J. & Wanhainen, A. Artery Atherosclerosis Among 65-year-old Swedish Men: A Population-based Screening Study. Eur J Vasc Endovasc Surg. 48, 5–10 (2014).
Tattersall, M. C. et al. Predictors of Carotid Thickness and Plaque Progression During a Decade The Multi-Ethnic Study of Atherosclerosis. Stroke. 45, 3257–3262 (2014).
Rodondi, N. et al. Impact of Carotid Plaque Screening on Smoking Cessation and Other Cardiovascular Risk Factors. Arch Intern Med. 172, 344–352 (2012).
Prati, P. et al. Prevalence and determinants of carotid atherosclerosis in a general population. Stroke. 23, 1705–1711 (1992).
Leng, X. Y. et al. Association Between Metabolic Syndrome and Carotid Atherosclerosis: A Community-Based Study in Hong Kong. Metab Syndr Relat Disord. 11, 109–114 (2013).
Chien, K. L. et al. Carotid Artery Intima-Media Thickness, Carotid Plaque and Coronary Heart Disease and Stroke in Chinese. PLoS ONE. 3, e3435 (2008).
Wang, W. et al. Distribution characteristics and risk factors of carotid atherosclerosis in middle-aged and elderly Chinese. Chin J Cardiol. 38, 553–557 (2010).
Rosvall, M. et al. Socioeconomic differences in the progression of carotid atherosclerosis in middle-aged men and women with subclinical atherosclerosis in Sweden. Social Science & Medicine. 62, 1785–1798 (2006).
Iemolo, F., Martiniuk, A., Steinman, D. A. & Spence, J. D. Sex Differences in Carotid Plaque and Stenosis. Stroke. 35, 477–481 (2004).
Ota, H. et al. Sex Differences in Patients With Asymptomatic Carotid Atherosclerotic Plaque. Stroke. 41, 1630–1635 (2010).
Jacobs, A. K. Women, ischemic heart disease, revascularization, and the gender gap: what are we missing? J Am Coll Cardiol. 47, S63–65 (2006).
Frink, R. J. Gender gap, inflammation and acute coronary disease: are women resistant to atheroma growth? Observations at autopsy. J Invasive Cardiol. 21, 270–277 (2009).
Xing, D., Nozell, S., Chen, Y. F., Hage, F. & Oparil, S. Estrogen and mechanisms of vascular protection. Arterioscler Thromb Vasc Biol. 29, 289–295 (2009).
Schulz, U. G. & Rothwell, P. M. Sex differences in carotid bifurcation anatomy and the distribution of atherosclerotic plaque. Stroke. 32, 1525–1531 (2001).
Kwon, T. G. et al. Prevalence andsignificance of carotid plaques in patients withcoronary atherosclerosis. Korean Circ J. 39, 317–321 (2009).
Eckstein, H. H. et al. Multidisciplinary German-Austrian Guideline Based on Evidence and Consensus. The diagnosis, treatment and follow-up of extracranial carotid stenosis. Dtsch Arztebl Int. 110, 468–476 (2013).
Pelisek, J., Eckstein, H. H. & Zernecke, A. Pathophysiological mechanisms of carotid plaque vulnerability: impact on ischemic stroke. Arch Immunol Ther Exp (Warsz). 60, 431–442 (2012).
Ebrahim, S. et al. Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women: the British Regional Heart Study. Stroke. 30, 841–850 (1999).
Rosvall, M. et al. Occupational status, educational level, and the prevalence of carotid atherosclerosis in a general population sample of middle-aged Swedish men and women: results from the Malmö Diet and Cancer Study. Am J Epidemiol. 152, 334–346 (2000).
Nash, S. D. et al. Socioeconomic status and subclinical atherosclerosis in older adults. Prev Med. 52, 208–212 (2011).
Lutsey, P. L. et al. Associations of acculturation and socioeconomic status with subclinical cardiovascular disease in the multi-ethnic study of atherosclerosis. Am J Public Health. 98, 1963–1970 (2008).
Fine-Edelstein, J. S. et al. Precursors of extracranial carotid atherosclerosis in the Framingham Study. Neurology. 44, 1046–1050 (1994).
Lanktree, M. B., Hegele, R. A., Schork, N. J. & Spence, J. D. Extremes of unexplained variation as a phenotype: an efficient approach for genome-wide association studies of cardiovascular disease. Circ Cardiovasc Genet. 3, 215–221 (2010).
Spence, J. D., Barnett, P. A., Bulman, D. E. & Hegele, R. A. An approach to ascertain probands with a non-traditional risk factor for carotid atherosclerosis. Atherosclerosis. 144, 429–434 (1999).
Gepner, A. D. et al. Comparison of Coronary Artery Calcium Presence, Carotid Plaque Presence, and Carotid Intima-Media Thickness for Cardiovascular Disease Prediction in the Multi-Ethnic Study of Atherosclerosis. Circ Cardiovasc Imaging. 8, e002262 (2015).
Ebrahim, S. et al. Carotid Plaque, Intima Media Thickness, Cardiovascular Risk Factors, and Prevalent Cardiovascular Disease in Men and Women: The British Regional Heart Study. Stroke. 30, 841–850 (1999).
Acknowledgements
This study was funded by Tianjin Medical University General Hospital and Peking University First Hospital.
Author information
Authors and Affiliations
Contributions
J.W., X.N., R.J. and J.Z. contributed to the study design. J.W. and X.N. performed data collection, data interpretation, and critical review. J.W. and X.N. performed data analysis. W.Z. contributed to drafting of the article. W.Z., Y.W., M.S., L.B., J.T., and Z.G. performed data collection, case diagnoses, and confirmation of case diagnoses.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhao, W., Wu, Y., Shi, M. et al. Sex Differences in Prevalence of and Risk Factors for Carotid Plaque among Adults: A Population-based Cross-Sectional Study in Rural China. Sci Rep 6, 38618 (2016). https://doi.org/10.1038/srep38618
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep38618
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
