
Abstract
In this multi-center cohort study, suicide attempters presenting to hospital (N = 355, 63% women) were interviewed using the Karolinska Interpersonal Violence Scale (KIVS) and followed-up by medical record review. Main outcome was non-fatal or fatal repeat suicide attempt within six months. Also, repeat attempt using a violent method was used as an additional outcome in separate analyses. Data were analyzed for the total group and for men and women separately. Repeat attempts were observed within six months in 78 persons (22%) and 21 (6%) of these used a violent method. KIVS total score of 6 or more was associated with repeat suicide attempt within six months (OR = 1.81, CI 1.08–3.02) and predicted new attempts with a sensitivity of 62% and a specificity of 53%. A three-fold increase in odds ratio was observed for repeat attempt using a violent method (OR = 3.40, CI 1.22–9.49). An association between exposure to violence in adulthood and violent reattempt was seen in women (OR = 1.38, CI 1.06–1.82). The overall conclusions are that information about interpersonal violence may help predict short-term risk for repeat suicide attempt, and that structured assessment of interpersonal violence may be of value in risk assessment after attempted suicide.
Similar content being viewed by others


Introduction
Suicide and suicide attempts are major public health concerns worldwide1. Essential for prevention is to facilitate the identification of patients with high risk for suicidal behavior in the short-term perspective after a health care visit2. A suicide attempt is the strongest known risk factor for later suicide3,4 and approximately half of all people who die by suicide have made at least one previous attempt5,6. In the year prior to their death from suicide, 15–20% visited a hospital in connection with a suicide attempt in a large study based in the UK7.
Suicide attempters presenting to hospital constitute a high-risk group for repeat suicide attempts. Young age and female gender influence the risk of repetition8,9,10,11. Coexisting severe psychiatric disorder and violent method used at an initial attempt indicate higher risk of a subsequent suicide3,12,13. A repeat attempt further elevates the risk of suicide mortality14,15. However, most studies of risk factors among suicide attempters have used a long-term follow-up (from years to decades), and therefore provide limited guidance in the shorter time perspective. For clinical management, the risk of repeat attempt in a time frame of weeks and months is more relevant for decisions concerning the immediate care16. Further research on factors related to short-term risk among suicide attempters is needed to guide preventive efforts2,16.
Violent methods such as using firearms, hanging and jumping from a height are associated with higher immediate lethality of an attempt17 as well as elevated risk of future suicide12,13. Further, violent methods are less common than poisonings and have been shown to be associated with higher levels of reported lifetime aggression18. Thus, identification of factors associated with violent suicide attempts may improve risk assessments.
An early traumatic life event is a known risk factor for later suicide 4, and exposure to violence in childhood is associated with later suicidal behavior19. Also, bullying victimization increases the risk for suicidal behavior as an adult, even after adjustment for psychiatric comorbidity20,21. A relationship between exposure to domestic violence and risk for suicide attempts has also been reported22. However, not only the victim of violence, but also the perpetrator, seems to have an increased risk for suicidal behavior4. Mutual pathways to aggressive and suicidal behavior have been suggested to involve traits of impulsivity and aggression4,23. High levels of aggression have been found among individuals who died by suicide when compared with psychiatric control subjects24.
Increased risk of suicide has been observed among suicide attempters with an experience of interpersonal violence25. The Karolinska Interpersonal Violence Scale (KIVS) is a short and useful tool for gathering information about a patient’s experiences of interpersonal violence as a child and as an adult, and both of exposure and expression of violence. The severity of the violence is graded using preset definitions (Appendix 1). Exposure to violence as a child and expression of violence as an adult measured with KIVS predicted suicide in a study with a follow-up period of 4–15 years25. In another study based on the same cohort, the predictive value of a combination of the KIVS and the Suicide Intent Scale (SIS) was analyzed, and the positive predictive value was enhanced further26. The scores on KIVS and SIS did not correlate with each other, indicating that the scales measure different aspects contributing to the risk of suicide in a long-term perspective. However, whether information about interpersonal violence can help predict suicide attempts in a short-term perspective has not been studied before. Therefore, in this clinical cohort study of suicide attempters, we aimed to evaluate the ability of the Karolinska Interpersonal Violence Scale to predict a repeat suicide attempt (non-fatal or fatal) within a short-term follow-up period of 6 months.
Our research questions were:
-
1
Can information about interpersonal violence, measured with KIVS, predict repeat suicide attempt within six months?
-
2
Are high scores on KIVS associated with repeat suicide attempt using a violent method?
-
3
Does the KIVS’s ability to predict suicide attempts differ according to gender?
Method
Study settings and population
This study is the first to use data from a multicenter study conducted in Sweden since 2012 at three psychiatric departments: at St. Göran’s Hospital in Stockholm, at Sahlgrenska University Hospital in Gothenburg and at Umeå University Hospital. Patients aged 18 and above presenting to hospital within a week after an act of deliberate self-harm with or without suicide intent were considered for participation. To enable follow-up through medical records, the inclusion criteria also included having a Swedish personal identity number, and being a resident of the catchment area of the specific hospital. Patients who were deemed unable to take part in the interview, either due to lacking language skills or due to acute symptoms interfering with verbal communication, were not asked to participate in the study. This included persons who were too confused, aggressive, psychotic or demented. Eligible patients were asked to participate and all participants gave written informed consent. Structured interviews were conducted within days after presenting to the hospital. Specially trained mental health care professionals conducted all interviews during daytime from April 25, 2012 to April 28, 2014.
Scorings and outcomes
The interview included the KIVS as well as a set of other instruments not analyzed in the present study. The KIVS consists of four subscales measuring expressions of violence and exposure to violence as a child (age 6–14), and expressions of violence and exposure to violence as an adult (age 15 and above). The two subscales capturing interpersonal violence as a child (age 6–14) also include experiences of bullying and bullying victimization. All subscales are scored from 0 to 5, with 0 corresponding to no violence at all and 5 to severe forms of interpersonal violence. Hence, the maximum total score on the KIVS is 20 points. In addition to the five continuous variables based on the total score and the four subscales of the KIVS, a dichotomized variable was created based on the total scores split at the median (0–5 vs. 6 or more). The reason for adding this binary variable in the analyses is to investigate a cut-off that possibly could be of pragmatic clinical use. This precise cut-off was chosen mainly because the score of 6 was both the mean and the median score of the suicide attempters in the previous cohort studied by Jokinen and coworkers 2010, but also because this score implies that at least two subscales have generated the score, not merely one. Also, the score of at least one subscale needs to be 2 or higher. For instance, a person with a total score of 6 or more has at least been involved in physical fights or has been bullied as a child, or has been either the perpetrator or victim of intimate partner violence as an adult. The full scale is presented in Appendix 1. The KIVS has previously been validated against the Buss–Durkee Hostility Inventory (BDHI), the “Urge to act out hostility” item from the Hostility and Direction of Hostility Questionnaire (HDHQ), and the Early Experiences Questionnaire (EEQ)25. The inter-rater reliability in the same study varied from r = 0.91 to r = 0.95 in the four subscales25. To be able to describe the cohort in diagnostic terms, the interview also included a synoptic diagnostic screening using the Mini International Neuropsychiatric Interview (M.I.N.I.)27.
Outcome was a new fatal or non-fatal suicide attempt within six months after the index attempt. We used the definition of actual suicide attempt used in the C-SSRS: a potentially self-injurious act committed with at least some wish to die, as a result of the act28. In additional analyses we used suicide attempt with a violent method as the outcome, defining violent method as all methods except poisoning (i.e. cutting, hanging, using shotgun, jumping from a height etc.). This distinction between violent method and poisoning is established in previous research17,29. It is also supported by research showing that the risk of subsequent suicide is significantly lower after poisoning when compared with other methods12,13. Information regarding outcome was extracted from the patient’s electronic medical records.
Statistical analyses
T-tests (2-tailed) were used to detect significant gender differences in mean age, and chi-square tests to determine gender differences in the results on the KIVS and the prevalence of diagnoses. Logistic regression analysis was used to calculate odds ratios for repeat suicide attempt. The four subscales and the total score were analysed as continuous variables. The odds ratios represent how risk changes with a one-step elevation on the scores. The variable “KIVS total score 6 or more” was analysed as a dichotomous variable. No adjustments have been made in the logistic regression models. Receiver operating characteristics (ROC) curves were used to further evaluate predictive properties of the KIVS subscales and the total score. All gender-specific results were made through separated analyses for men and women. All statistical analyses were made with SPSS Version 22.030.
Ethical statement
Ethical approval was obtained for this study from the Gothenburg Regional Ethics Committee (589–10). The methods used in this study were in accordance with the ethical approval. Written informed consent was obtained from all included subjects.
Results
Participants
In total 665 self-harming patients were eligible for inclusion and 452 agreed to participate (68.0%). For the purpose of this paper, 82 persons without suicidal intention at the index self-harm act as defined by the Columbia Suicide Severity Rating Scale28 were excluded from the analyses, as were those lacking KIVS data (n = 15). The current study is thus based on data for 355 suicide attempters (133 men and 222 women), with a mean age of 40 years (range 18 to 92 years, median 35). The women were younger than the men (mean age 37 years vs. 45, p < 0.001), and women predominated in age groups up to 44 years (Table 1). According to the results of the M.I.N.I.-interviews, a majority (60%) of the participants met criteria for ongoing major depression. An ongoing episode of bipolar disorder was reported in 15% of the participants. Anxiety disorders were common (72%), and ongoing psychotic syndrome was found in 6%. The only significant gender differences observed were found in the diagnostic categories of ongoing substance use disorder (47% of male participants and 31% of female, p = 0.004), and ongoing eating disorder which was reported by 13% of the female participants and 3% of the men (p = 0.003).
Risk of repeat suicide attempt
In the cohort of 355 suicide attempters, 78 (22.0%) made a fatal or non-fatal repeat suicide attempt within six months (50 women, 28 men) and five of these were suicides (three women, two men). Violent methods were used in four of these suicides (one man used poisoning as method). In all, fatal or non-fatal repeat attempt with violent method was recorded for 21 participants (5.9%). Sixteen were noted for women (7.2% of all women) and five for men (3.8%).
KIVS score
The mean total KIVS score was 6.0 with no gender difference (men 6.1, women 6.0, p = 0.189). Gender differences were observed with higher scores for men in the two subscales covering expression of violence, and higher scores for women in the two subscales covering exposure to violence. There was no significant gender difference in the total scores (Table 2).
KIVS score in relation to risk of repeat suicide attempt
In bivariate logistic regression, having a KIVS total score of 6 or more was associated with an increased risk for repeat suicide attempt within six months (Odds Ratio = 1.81, CI 1.08–3.02). The subscale “exposure to violence as an adult” was associated with an increased risk for repeat suicide attempt within six months (OR = 1.14, CI 1.01–1.29) (Table 3).
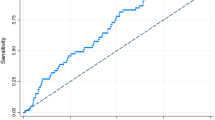
The significant subscales in the logistic regression analysis were tested further using ROC curves. The dichotomous variable “KIVS total score of 6 or more” generated a ROC curve with an Area Under the Curve (AUC) of 0.57 (p = 0.049) (Fig. 1). A result of 6 or more points on the KIVS predicted a repeat suicide attempt with a sensitivity of 62% and a specificity of 53%. A KIVS total score of 6 or more was also associated with an increased risk for a new attempt using a violent method (OR = 3.40, CI 1.22–9.49) (Table 4). The subscale “exposure to violence as an adult” could not significantly predict a new suicide attempt within six months when analysing its ROC curve (AUC = 0.57, p = 0.065) (ROC curve not shown).

ROC-curve for the KIVS subscale “KIVS total score of 6 or more” predicting fatal or non-fatal suicide attempt within six months, men and women combined.
Gender-specific analyses
Neither the total score of KIVS nor any of the subscales were significantly associated with repeat suicide attempt within six months in the gender-specific analysis. However, gender differences unfolded when analyzing the outcome repeat attempt using violent method. In women the dichotomous variable KIVS total score of 6 or more was associated with an almost fivefold increase in risk (Table 4). Also, higher results on the subscale “exposure to violence as an adult” increased the risk of repeat suicide attempt using a violent method within six months among women (OR = 1.38, CI 1.05–1.81, p = 0.020). No associations were observed in men.
The ROC curve for the dichotomous variable of KIVS total score of 6 or more used as a test to predict repeat suicide attempt using a violent method among women showed an AUC = 0.67 (p = 0.025) (Fig. 2A) and a sensitivity of 81% and a specificity of 52%.

ROC-curves for the subscales (A) “KIVS total score of 6 or more”, and (B) “Exposure to violence as an adult” predicting fatal or non-fatal suicide attempt with a violent method within six months, women only.
Using the subscale “exposure to violence as an adult” as a test to predict a new suicide attempt using a violent method within six months among women generated a ROC curve with an AUC of 0.68 (p = 0.016) with an optimal cut-off point at 3 generating a sensitivity of 75% and a specificity of 57% (Fig. 2B).
Discussion
To our knowledge, this is the first study to link a certain degree of reported interpersonal violence with an elevated short-term risk of repetition of suicidal behavior. Repetition has in itself been found to double the risk for eventual suicide15, making our finding relevant from a suicide prevention perspective. We found that scoring 6 or more on the Karolinska Interpersonal Violence Scale was associated with repeat suicide attempt within six months. To reach a score of 6 or more on the KIVS implicates that at least two of the subscales are involved, assuring that not only one single occasion of interpersonal violence explains the total score. It also means that more severe forms of interpersonal violence must have occurred. Still, a score of 6 or more can be reached in many different ways, since the scale captures a broad variety of experiences.
The overall predictive value of the scale should not be overstated based on our results. Both the sensitivity (62%) and the specificity (53%) to detect repeat attempts are unsatisfactory, although not far from the predictive properties of other suicide risk assessment tools previously evaluated in the literature16. Nevertheless, an aspect that makes our findings interesting is that the KIVS, contrary to most other suicide risk assessment tools, does not include any questions directly about psychiatric symptoms or suicidal ideation/behavior. It illuminates other relevant experiences of interpersonal violence that may have been previously overlooked in suicide risk assessments.
Experiences of interpersonal violence were common in the cohort. The mean total KIVS score of 6.0 was consistent with that reported in a long-term Swedish follow-up study of suicide attempters25. The latter study also included a healthy control group with a mean total score of 2.9, showing that suicide attempters experience interpersonal violence to a larger extent25. Findings from cross-sectional studies of alcohol dependent31 and borderline32 patients support the notion that information about interpersonal violence have relevance for prediction of suicidal behavior in different clinical samples.
We found that being a victim of violence as an adult was associated with repeated suicidal behavior. None of the other three subscales were in themselves significantly associated with the outcome. This is in contrast with the earlier longitudinal study25 where the subscales covering exposure to violence as a child and expression of violence as an adult were most strongly linked with suicide. This is probably due to differences in study design since the present study use a different outcome, including both non-fatal and fatal attempts, and a shorter follow-up time. The results may indicate that different kinds of experiences of interpersonal violence affect subsequent risk for attempted suicide and completed suicide differently. For an adult, to have been a victim of violence in childhood could be considered as a distal risk factor, whereas victimization in adulthood is more of an acute stressor associated with suicidal behavior in a shorter time perspective. Also, the more impulsive nature of suicide attempts than of completed suicide33 could be a reason that a proximal stressor, the experience of being exposed to violence more recently in adulthood, is of particular relevance to the outcome of suicide attempts in the present study.
The answer to our main research question is that information about interpersonal violence may contribute to the prediction of new suicide attempts in a short time perspective.
Our second research question concerned the prediction of violent reattempts. Having a total score of 6 or more on KIVS elevated the risk for a new violent attempt significantly and with a higher point estimate (OR = 3.4) than for repeat attempt regardless of method (OR = 1.8). This may indicate that the violent attempters as a group is closer to the suicide phenotype, previously shown to be associated with higher scores on the KIVS25.
The third research question, about gender differences, could not be unequivocally answered, since the confidence intervals of the risk estimates in the gender-stratified analyses were too broad to separate the odds ratios for men and women. However, a possible gender difference was observed when analyzing risk for violent reattempt. The finding that being a victim of violence as an adult could predict violent suicide attempts among female suicide attempters harmonize with previous research showing that domestic violence against women is associated with suicide attempts34. For men we found no significant association, but the number of men with violent reattempts was small, limiting the statistical power. Violent methods are associated with higher immediate lethality17 and elevated risk of later suicide12,13, probably to a certain extent because it indicates a stronger suicidal intention. In large epidemiological studies of suicide attempters, women tend to choose violent methods more seldom than men12,13, in contrast with our present result. An important methodological difference that partly may explain this is that we in our clinical sample excluded self-harmers without suicide intent, something that cannot be done in larger epidemiological studies based on data relying on ICD-10 codes, which do not differentiate between non-suicidal self-harm and suicide attempt. However, this distinction is relevant since the choice of method in a self-harm act most likely is linked with the intention of the act. Another possible reason for the observed gender difference is that interpersonal violence experienced by younger women may have a slightly different impact on their development of suicidal behavior than in men, perhaps rendering the latter more likely to use violent methods. In line with the interpersonal theory by Joiner35, the exposure of violence may have desensitized these women to experiencing physical pain, making them more capable of violent self-injurious behavior.
A recent Swedish population study showed a link between depression and violent crime36. The authors conclude that assessment of risk of violence, which to a large extent depends on information about previous experiences of interpersonal violence, should be considered routinely for certain subgroups of patients with depression, including those who have engaged in self-harm. The results from our present study support a similar notion that questions about interpersonal violence also could be relevant from a suicide risk assessment perspective, and for this reason should be used more often in certain clinical situations such as in the aftermath of a suicide attempt. However, despite the significant association with the outcome, the KIVS provides limited sensitivity and specificity in predicting repeat attempts on its own, and should only be considered as a complement to regular risk assessment.
Also, further research is needed to disentangle the associations and causal pathways between interpersonal violence and suicidal behavior, to enable even better prediction and tailor-made preventive interventions.
Strengths and limitations
The large sample size enabled sufficient power to analyze short-term risk for a repeat suicide attempt, and even to some extent, gender-specific analyses. However, the study sample was too small to also allow further division in subgroups according to age and diagnosis, hence these variables could only be used to describe the cohort. Also, the number of suicide deaths was too small to enable separate analyses. A larger sample size is needed to determine whether findings in the present study may also pertain to suicide mortality.
All participants included in the present study acknowledged suicidal intention at the index attempt, which makes our findings easier to interpret clinically compared with register-based studies dependent on ICD-codes that also include acts of deliberate self-harm without suicidal intention. In this study we rely on self-reported information about interpersonal violence. There is risk of recall bias when asking delicate questions shortly after a traumatic event such as a suicide attempt. Also, patients who were too aggressive to participate were not included, generating a selection bias towards a perhaps less aggressive patient population. These limitations should be considered when generalizing our results to other patient populations.
Information about the studied outcome was extracted from the patient’s electronic medical records. Suicide attempts that were not reported in the medical records are lacking. This introduces a bias that probably favors more severe forms of suicidal behavior with higher probability of being reported in medical records. This is important to remember when interpreting our results.
Finally and importantly, the significant findings reported in this study have p-values not far from 0.05. This in itself means that the validity of the results needs to be confirmed in future studies. Furthermore, for a clinician, the predictive value of this scale, as with all other scientifically evaluated suicide risk assessment tools, is unsatisfactory, and we can merely propose that aspects of interpersonal violence may be included in the clinical assessment of patients who have attempted suicide.
Conclusion
In this cohort study of 355 suicide attempters, self-reported history of interpersonal violence was associated with elevated risk for a new fatal or non-fatal attempt within a clinically relevant follow-up period of six months. Questions regarding interpersonal violence may help to inform clinical assessments in the aftermath of a suicide attempt.
Additional Information
How to cite this article: Haglund, A. et al. Interpersonal violence and the prediction of short-term risk of repeat suicide attempt. Sci. Rep. 6, 36892; doi: 10.1038/srep36892 (2016).
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Saxena, S., Krug, E. G., Chestnov, O. & World Health Organization. Department of Mental Health and Substance Abuse. Preventing suicide: a global imperative. (World Health Organization, 2014).
Rockville, M. (National Institute of Mental Health and the Research Prioritization Task Force, http://www.suicide-research-agenda.org, 2014, accessed 2016-06-13).
Tidemalm, D., Langstrom, N., Lichtenstein, P. & Runeson, B. Risk of suicide after suicide attempt according to coexisting psychiatric disorder: Swedish cohort study with long term follow-up. BMJ 337, a2205, doi: 10.1136/bmj.a2205 (2008).
Hawton, K. & van Heeringen, K. Suicide. Lancet 373, 1372–1381, doi: 10.1016/S0140-6736(09)60372-X (2009).
Foster, T., Gillespie, K., McClelland, R. & Patterson, C. Risk factors for suicide independent of DSM-III-R Axis I disorder. Case-control psychological autopsy study in Northern Ireland. Br J Psychiatry 175, 175–179 (1999).
Runeson, B. S., Beskow, J. & Waern, M. The suicidal process in suicides among young people. Acta Psychiatr Scand 93, 35–42 (1996).
Gairin, I., House, A. & Owens, D. Attendance at the accident and emergency department in the year before suicide: retrospective study. Br J Psychiatry 183, 28–33 (2003).
Canetto, S. S. & Sakinofsky, I. The gender paradox in suicide. Suicide Life Threat Behav 28, 1–23 (1998).
Nock, M. K. et al. Suicide and suicidal behavior. Epidemiol Rev 30, 133–154, doi: 10.1093/epirev/mxn002 (2008).
Hawton, K., Zahl, D. & Weatherall, R. Suicide following deliberate self-harm: long-term follow-up of patients who presented to a general hospital. Br J Psychiatry 182, 537–542 (2003).
Conwell, Y., Duberstein, P. R. & Caine, E. D. Risk factors for suicide in later life. Biol Psychiatry 52, 193–204 (2002).
Runeson, B., Tidemalm, D., Dahlin, M., Lichtenstein, P. & Langstrom, N. Method of attempted suicide as predictor of subsequent successful suicide: national long term cohort study. BMJ 341, c3222, doi: 10.1136/bmj.c3222 (2010).
Runeson, B., Haglund, A., Lichtenstein, P. & Tidemalm, D. Suicide risk after nonfatal self-harm: a national cohort study, 2000–2008. J Clin Psychiatry, doi: 10.4088/JCP.14m09453 (2015).
Carroll, R., Metcalfe, C. & Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: systematic review and meta-analysis. PLoS One 9, e89944, doi: 10.1371/journal.pone.0089944 (2014).
Zahl, D. L. & Hawton, K. Repetition of deliberate self-harm and subsequent suicide risk: long-term follow-up study of 11,583 patients. Br J Psychiatry 185, 70–75 (2004).
Bolton, J. M., Gunnell, D. & Turecki, G. Suicide risk assessment and intervention in people with mental illness. BMJ 351, h4978, doi: 10.1136/bmj.h4978 (2015).
Elnour, A. A. & Harrison, J. Lethality of suicide methods. Inj Prev 14, 39–45, doi: 10.1136/ip.2007.016246 (2008).
Dumais, A. et al. Is violent method of suicide a behavioral marker of lifetime aggression? Am J Psychiatry 162, 1375–1378, doi: 10.1176/appi.ajp.162.7.1375 (2005).
Brezo, J. et al. Predicting suicide attempts in young adults with histories of childhood abuse. Br J Psychiatry 193, 134–139, doi: 10.1192/bjp.bp.107.037994 (2008).
Klomek, A. B. et al. Childhood bullying as a risk for later depression and suicidal ideation among Finnish males. J Affect Disord 109, 47–55, doi: 10.1016/j.jad.2007.12.226 (2008).
Klomek, A. B. et al. Childhood bullying behaviors as a risk for suicide attempts and completed suicides: a population-based birth cohort study. J Am Acad Child Adolesc Psychiatry 48, 254–261, doi: 10.1097/CHI.0b013e318196b91f (2009).
Dufort, M., Stenbacka, M. & Gumpert, C. H. Physical domestic violence exposure is highly associated with suicidal attempts in both women and men. Results from the national public health survey in Sweden. Eur J Public Health, doi: 10.1093/eurpub/cku198 (2014).
Gvion, Y. & Apter, A. Aggression, impulsivity, and suicide behavior: a review of the literature. Arch Suicide Res 15, 93–112, doi: 10.1080/13811118.2011.565265 (2011).
Dumais, A. et al. Risk factors for suicide completion in major depression: a case-control study of impulsive and aggressive behaviors in men. Am J Psychiatry 162, doi: 10.1176/appi.ajp.162.11.2116 (2005).
Jokinen, J. et al. Karolinska Interpersonal Violence Scale predicts suicide in suicide attempters. J Clin Psychiatry 71, 1025–1032, doi: 10.4088/JCP.09m05944blu (2010).
Stefansson, J., Nordström, P., Runeson, B., Åsberg, M. & Jokinen, J. Combining the Suicide Intent Scale and the Karolinska Interpersonal Violence Scale in suicide risk assessments. BMC Psychiatry 15, 226, doi: 10.1186/s12888-015-0607-6 (2015).
Sheehan, D. V. et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 59, Suppl 20, 22-33;quiz 34–57 (1998).
Posner, K. et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry 168, 1266–1277, doi: 10.1176/appi.ajp.2011.10111704 (2011).
Asberg, M., Traskman, L. & Thoren, P. 5-HIAA in the cerebrospinal fluid. A biochemical suicide predictor? Arch Gen Psychiatry 33, 1193–1197 (1976).
IBM Corp. SPSS Statistics for Macintosh, Version 22.0 (Armonk, NY) URL http://www.ibm.com/ (2013).
Khemiri, L., Jokinen, J., Runeson, B. & Jayaram-Lindstrom, N. Suicide Risk Associated with Experience of Violence and Impulsivity in Alcohol Dependent Patients. Sci Rep 6, 19373, doi: 10.1038/srep19373 (2016).
Sinai, C. et al. Thyroid hormones and adult interpersonal violence among women with borderline personality disorder. Psychiatry Res 227, 253–257, doi: 10.1016/j.psychres.2015.03.025 (2015).
Klonsky, E. D., May, A. M. & Saffer, B. Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annual review of clinical psychology 12, 307–330, doi: 10.1146/annurev-clinpsy-021815-093204 (2016).
Devries, K. M. et al. Intimate partner violence and incident depressive symptoms and suicide attempts: a systematic review of longitudinal studies. PLoS Med 10, e1001439, doi: 10.1371/journal.pmed.1001439 (2013).
Van Orden, K. A. et al. The interpersonal theory of suicide. Psychological review 117, 575–600, doi: 10.1037/a0018697 (2010).
Fazel, S. et al. Depression and violence: a Swedish population study. Lancet Psychiatry 2, 224–232, doi: 10.1016/S2215-0366(14)00128-X (2015).
Acknowledgements
This study was supported by grants from the Swedish Research Council 521- 2011-299, K2009-61P-21304-04-4; K2009-61X-21305-01-1, and by the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet 20120528, and by financial support through regional agreement between Umeå University and Västerbotten County Council (ALF) on cooperation in the field of Medicine, Odontology and Health.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: A.H., H.L., E.S.R., M.W. and B.R. Contributed with data: M.W., E.S.R. and B.R. Performed the statistical analyses: A.H., H.L. and J.J. Analyzed the results: A.H., Å.L., H.L., E.S.R., J.J., M.W. and B.R. Wrote and reviewed the manuscript: A.H., Å.L., H.L., E.S.R., J.J., M.W. and B.R.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Haglund, A., Lindh, Å., Lysell, H. et al. Interpersonal violence and the prediction of short-term risk of repeat suicide attempt. Sci Rep 6, 36892 (2016). https://doi.org/10.1038/srep36892
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep36892
This article is cited by
-
Trajectories to Suicide Following Intimate Partner Violence Victimization: Using Structural Equation Modelling to Examine Suicide and PTSD in Female Emergency Department Users
Journal of Family Violence (2023)
-
Age-related injury patterns resulting from knife violence in an urban population
Scientific Reports (2022)
-
Cues for different diagnostic patterns of interpersonal violence in a psychiatric sample: an observational study
BMC Psychiatry (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
