
Abstract
Atypical and malignant meningiomas are rare. Our aim was to examine the treatment outcomes following surgical resection, and analyze associations between clinical characteristics and overall survival (OS) or relapse free survival (RFS). 102 patients with atypical or malignant meningiomas underwent microsurgical resection between June 2001 and November 2009 were analyzed retrospectively. We compared demographics, clinical characteristics, treatment, and complications. The five-year and ten-year overall survival rates were 93.5% and 83.4%, respectively. Three factors significantly reduced OS: Malignant meningiomas (p < 0.001), which also decreased RFS (p < 0.001); female patients (p = 0.049), and patients with Karnofsky Performance Status (KPS) < 70 at diagnosis (p = 0.009). Fifty two patients (51%) experienced tumor relapse. Total resection of tumors significantly impacted RFS (p = 0.013). Tumors located at parasagittal and posterior fossa area lead to higher relapse rate (p = 0.004). Subtotal resection without adjuvant radiotherapy lead to the worst local control of tumor (p = 0.030). An MIB-1 index <8% improved OS and RFS (p = 0.003). Total resection of atypical and malignant meningiomas provided better outcome and local control. Adjuvant radiation therapy is indicated for patients with malignant meningiomas, with incompletely excised tumors; or with tumors in the parasagittal or posterior fossa area. The MIB-1 index of the tumor is an independent prognostic factor of clinical outcome.
Similar content being viewed by others

Introduction
Meningiomas, one of the most common intracranial tumors, accounts for 13% to 26% of brain tumors and have an annual incidence of 6 per 100,000 people1. In 2000 and 2007, World Health Organization(WHO) graded meningiomas with histological standards. The standards are based on both of subjective and objective (mitotic index) criteria2: around 90% are benign (WHO grade I), 5–7% are atypical (WHO grade II), and only 1–3% are considered anaplastic or malignant (WHO grade III)3. This recent adoption of modern grading criteria and the rarity of the malignant subtype have limited the amount of available data on the clinical behavior, outcomes, and optimal treatment of meningiomas4.
Benign meningiomas contribute to relatively good prognosis, but atypical and malignant meningiomas show rapid progression and more invasion. Five-year progression- free survival and overall survival of approximately 50% and 60%, respectively was shown1,4,5,6. Gross total resection (GTR) is the optimal surgical principle for benign meningiomas, but the standard of care for atypical and malignant meningiomas has yet to be established7,8. The two high grade histopathology tumor types are more brain invasive, and radical surgical strategies can lead to high morbidity and poor overall outcome9. Previous literature shows that age less than 40 years, cranial base meningiomas, and male sex are associated with recurrence in benign meningiomas that have been subtotally excised, but such data are not available for atypical and anaplastic meningiomas1,10.
Both benign and malignant meningiomas have an equal propensity to bleed, whereas malignant tumors are not necessarily more vascular than benign tumors1. Pre-operative embolization of meningiomas helps reduce intra-operative tumor bleeding, which may decrease surgical time and make surgical resection easier11. The practice patterns of embolization prior to surgery vary widely12,13, and not all neurosurgeons consider embolization due to possible complications14.
It remains controversial about the role of adjuvant radiotherapy and stereotatic radiosurgery after surgical resection15,16,17,18,19. There is evidence supporting early addition of adjuvant radiotherapy after GTR to achieve better local tumor control15,20, but this is not universally recommended21,22.
To establish optimal treatment strategies, accurate evaluation of the prognostic factors in atypical and malignant meningiomas is essential. To define the correlation factor with atypical and malignant meningioma progression or recurrence, we retrospectively analyzed the clinical parameters and post-operative outcomes of patients with these tumors.
Results
Patient Demographics and Tumor Characteristics
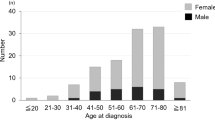
The group (45 male and 57 female patients) had a KPS of 74.31 ± 8.27 at initial evaluation and a mean age of 57 ± 16.7 years during surgery (Table 1). According to histopathological grade with 2007 criteria, the menigniomas were stratified into two groups: WHO grade II (n = 86) and WHO grade III (n = 16). Tumors were also divided into four categories according to the anatomic location: convexity (n = 33); parasagittal (n = 32); skull base (n = 29); and posterior fossa (n = 8). The MIB-1 proliferative index that measures Ki-67 expression was available for 87 tumor specimens and had an average score of 8.6% ± 6.1%.
Most patients (90/102; 88.2%) survived until the end of follow up: mean survival time was 160 ± 8.9 months (range 13–192 months). The five-year overall survival rate was 93.5% (95% confidence interval [CI], 90.9–96.1%) and ten-year OS rate was 83.4% (95%CI, 78.1–88.7%). Twelve patients didn’t survive at the endpoint. One died due to lung cancer. For other 11 patients, the cause of death directly or indirectly associated with progressive meningioma, which included brain stem compression in 5 patients, pneumonia and respiratory failure in 4 patients, and severe sepsis in 2 patients.
Univariate analysis indicated that the overall survival was significantly influenced by sex, KPS, WHO grade, and MIB-1 index. Multivariate analysis indicated that sex, KPS, and WHO grade remained significant prognostic factors (Table 2). Kaplan-Meier analysis illustrated that malignant tumors (HR = 7.6, p < 0.001, Fig. 1a), female patients (HR = 9.3, p = 0.009) and KPS < 70 (HR = 5.1, p = 0.009) contribute to decreased OS. The location or size of tumors, the extent of resection, and adjuvant radiotherapy did not influence the overall survival significantly.

Kaplan-Meier estimates of overall survival (a) and relapse free survival (b) for patients with WHO grade II and grade III meningiomas. (p < 0.001).
The disease relapsed during follow-up in 52 patients (51%). The average time to tumor relapse was 84.1 months (95% CI 77.3–90.9 months). The relapse free survival (RFS) rate at one, three and five years was 84.3%, 65.7% and 57.8%, respectively. Univariate analysis indicated that RFS was significantly influenced by WHO grade, tumor location, surgical extent, and MIB-1 index. Multivariate analysis indicated only WHO grade, surgical extent, and MIB-1 index remained significant factors (Table 2). No association was detected between adjuvant radiotherapy and duration of RFS. Tumor sizes were not associated with the completeness of tumor resection (p = 0.838) nor disease relapse (p = 0.883). Data analysis with Kaplan-Meier method made three inferences. First, a higher WHO grade of meningiomas was associated with a poorer RFS (HR = 3.5, p < 0.001, Fig. 1b). Second, tumor location affected prognosis: patients with tumors at convexity and skull base had better outcome, but patients with parasagittal and posterior fossa meningiomas experienced higher tumor relapse rate (HR = 2.2, p = 0.004, Fig. 2) Third, a comparison between GTR and STR revealed longer RFS occurred after complete resections (HR = 1.987, p = 0.013, Fig. 3).

Relapse free survival between different location of tumors (p = 0.004).

Kaplan-Meier analysis of relapse free survival as stratified by extent of resection.
(p = 0.013) Abbreviations: GTR, gross total resection; STR, subtotal resection.
We next divided patients into four subgroups to assess whether adjuvant radiotherapy in combination with surgical resection provided a RFS benefit for atypical and malignant meningioma patients: (1) GTR with adjuvant RT, (2) GTR without adjuvant RT, (3) STR with adjuvant RT, and (4) STR without adjuvant RT. Analysis showed a trend that patients who underwent GTR and RT had the lowest recurrent rate (41.8%), followed by those with GTR and without RT (53.6%), STR with RT (60.9%), while STR without RT had the highest recurrent rate (72.7%). Although patient groups who underwent GTR with versus without adjuvant RT did not show a significant difference by Kaplan-Meier survival analysis (p = 0.211), the patient groups who underwent STR showed a trend that adjuvant radiotherapy subgroup had better RFS (p = 0.053). The patient subgroup who received STR without RT had significantly shorter RFS than the other three subgroups (HR = 2.9, p = 0.008).
The tumor of 29 patients (28.4%) was embolized before surgery, and embolization induced no complications nor neurologic deficit. The mean size of tumors with embolization was 5.2 ± 1.9 cm, while the mean size of tumors without embolization was 5.3 ± 2.1 cm (p = 0.951). Embolization group had average intra-operative blood loss of 706 ± 217cc. Patients who didn’t receive embolization had average blood loss of 1043 ± 303cc. (p = 0.061). In addition, 23 of 29 patients with tumor embolization underwent GTR to tumors, which induced benefit to better RFS significantly. In other 73 patients not to have embolization, 46 had tumor total resection. The total resection rate was relatively higher in the patients receiving pre-operation embolization (79.3% vs 63.0%, p = 0.086, Table 3).
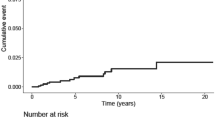
Forty-five of 52 patients (86.5%) who developed tumor relapse during follow up received salvage therapy. Thirty-two patients (61.5%) underwent treatment with repeat surgery and radiotherapy; 10 patients (19.2%) underwent repeat surgery alone; and 3 patients (5.8%) underwent radiotherapy or radiosurgery alone. Factors associated with the decision for the mode of salvage therapy were not uniformly available. Of the 42 patients undergoing second operation to relapse tumors, 36 survived at the end. On the other hand, 5 of 10 patients without repeat surgical treatment (no salvage treatment or radiotherapy/radiosurgery alone) survived at the end. Survival rate were 85.7% and 50%, respectively (p = 0.025). Kaplan-Meier analysis also demonstrated a survival benefit with repeat operation to relapse disease.(p = 0.066, Fig. 4).

Kaplan-Meier analysis to overall survival of patients with relapse tumors.
Repeat surgery associated with a better overall survival (p = 0.066).
Rate of complications
No deaths occurred during or following microsurgical tumor resection, within 30 days. Twenty five patients (24.5%) experienced at least one surgical, medical or neurological complication after their surgery. Three patients (2.9%) developed cardiac complications and pneumonia. Surgical complications (n = 16, 15.8%) included 6 wound infections or breakdown, 5 post-operative hematoma requiring evacuation, 3 cerebrospinal fluid leakage, and 2 hydrocephalus. On the other hand, 10 patients experienced significant neurological morbidity (9.8%) related to their tumor resection, such as cranial neuropathy and hemiparesis. Some patients had self-limiting symptoms like dizziness, headache, and skin irritation after radiotherapy, but there were no severe acute side effects.
Discussion
Atypical and malignant meningioma patients comprised 4.2% and 1.2% of the meningioma cohort in the USA23, similar to the meningioma cohort (n = 936) in Finland24: grade I 94.3%, grade II 4.7%, and grade III 1.0%24. In our study, 922 patients had newly diagnosed meningiomas at our institute, and patients with WHO grade II and III meningiomas accounted for 9.2% (n = 86) and 1.7% (n = 16), respectively. Kshettry et al. also reported that Black and Asian Pacific Islander races were both associated with the highest incidence of WHO II/III meningiomas23. To the best of our knowledge, the present study is one of the largest case series that examined the treatment outcomes for meningiomas with atypical and malignant histology of Asian populations.
In the current study, the five-year overall survival rate of the patients with grade II and grade III meningioma was 97.5% and 67.4%, while median survival time was 167 months and 72 months, respectively. Perr et al. reported that the median survival time for patients with grade II lesions ranged from 10 to 14 years and they showed 75% 5-year overall survival rate. The median survival time for patients with grade III lesions was 1.5 years, with a 5-year survival rate of 32%25. A review article reported a median 5-year overall survival of 67.5% (range 51–100%) in grade II patients and 55.6% (range 27–80.8%) in grade III patients4. The relative higher survival rate in the present cohort is probably because of the aggressive retreatment strategy, especially surgery for recurrent tumors. Most patients with tumor recurrence or progression (49/52; 94%) underwent salvage treatment (surgery, radiotherapy, or both). We performed 80 repeat surgeries in these patients, and one patient received eight surgical resections.
In the current series, patient sex was a prognostic factor to overall survival, since female patients had significantly poorer outcome than male patients (HR: 9.3, p = 0.009). In our study, patient age at diagnosis had no influence on overall survival. In contrast, D. Pasquier et al. indicated that an age of >60 years was a significant adverse prognostic factor, whereas sex did not correlate with overall survival26. Milosevic et al.27. reported that an age of less than 40 years was associated with a favorable outcome. In our opinion, patient’s physical condition, as aptly measured by KPS, is more important than age. Our finding of KPS as a prognostic factor supports this explanation: patients with KPS ≥ 70 had better overall survival than those with KPS < 70 (HR = 5.1, p = 0.009).
Because several classification criteria exist for grading histopathology severity of meningiomas in the past two decades, evaluating reported treatment results for these rare tumors has been difficult. In our series, we adapted the latest 2007 WHO revision classification scheme and showed that the WHO grade of meningioma definitely plays an important role in clinical outcome. Patients with WHO grade III meningioma had both poorer overall survival and relapse free survival rates than those with WHO grade II tumors, similar to articles by Palma et al.28. and Perry et al.25. The worst prognosis was attached to meningiomas with frank histological anaplasia, whether invasive or not1. Therefore, the 2007 revision identified brain invasion as the primary criterion for Grade II lesions, and a greater percentage of meningiomas have been classified as atypical over the last decade.
The location of atypical and malignant tumors significantly influences the RFS in the present study, in agreement with Kane et al.5. Dziuk et al. reported that the parasagittal-falcine lesions present with the highest recurrence rates through reviewed recurrent atypical and anaplastic tumors29. In our study, the RFS is decreased significantly in patients with parasagittal and posterior fossa tumors (HR = 2.2, p = 0.005). These tumors often were attached to or invade the sinus wall of the superior sagittal sinus or transverse sinus. This tumor location increases the difficulty of radical resection and may obscure residual tumor due to sinus enhancement, which may mislead the surgeon on the completeness of the tumor resection.
Embolization of meningioma prior to surgery has been performed for many years, although no dedicated studies assess its role in the treatment of atypical and malignant meningiomas. In our study, patients who underwent embolization had less average bleeding volumes during the operation. There was also a trend to a higher rate of GTR, which prolong RFS consequently. No patients presented complications following embolization, including contrast medium renal toxicity, stroke, carotid dissection, or acute deterioration caused by bleeding within a necrotic meningioma. The results suggested that atypical and malignant meningiomas respond positively to embolization before operation, especially those hypervascular tumors identified on image studies.
For benign meningioma, GTR is the standard surgical principle. Ayal et al. disclosed that the extent of resection is a powerful predictor of outcome for patients with atypical and malignant meningioma30. However, radical excision is complicated in some area like skull base because of many critical structures. Severe morbidity, even mortality may be the consequence of aggressive resection. In order to preserve neurological function, STR can be considered as an alternative surgical management. We previously showed that GTR increases progression free survival in patients with skull base atypical meningiomas31, consistent with previous findings by Yang et al.32, Goyal et al.7, and Zaher et al.33. Conversely, Rosenberg et al.34, Boskos et al.35, and Pasquier et al.26 found that the extent of resection was not a significant prognostic factor for OS or PFS in their RT-treated cohorts. In our study, GTR significantly prolonged RFS in atypical and malignant meningioma patients, in spite of no correlation with OS. Six patients (8.7%) who underwent GTR developed neurologic deficit like facial palsy or hemiparesis, while four patients (12.1%) with STR had facial palsy. The relatively low complication rate after GTR infers that extensive surgical strategy is able to prolong relapse free survival and cause no neurologic sequelae with modern microsurgical techniques.
The outcomes of patients who received adjuvant radiotherapy treatment following surgery for atypical meningioma are inconsistent. The latest systematic review revealed that adjuvant radiotherapy generally improves local control and OS in atypical and malignant meningiomas, although available data did not support this paradigm in the controversial subset of totally excised atypical meningiomas4. In our series, whether patient had adjuvant radiotherapy alone is not a prognostic factor to OS and RFS. In addition, adjuvant radiotherapy in patients who underwent GTR showed no significant association with RFS although GTR with adjuvant radiotherapy contributed to lower recurrent rate. However, radiation therapy was associated with decreased local recurrence among patients undergoing STR (but not GTR) by using a Kaplan-Meier analysis. These data suggest that adjuvant radiotherapy does not provide additional benefit for local tumor control in patients with complete tumor resection. Otherwise, STR combined with adjuvant radiotherapy reduced tumor progression with similar efficacy as GTR. Physicians should consider the difficulty of evaluating the extent of resection in posterior fossa and parasagittal tumors, and adjuvant radiotherapy can provide the benefits. We recommend adjuvant RT for all tumors that occupy these two locations.
The correlation between histological grading and Ki-67 antigen expression in meningioma is strong, and the antigen expression can be detected by the MIB-1 monoclonal antibody36. Although a poor prognosis may be associated with a high MIB-1 labeling index, significant overlap exists in the MIB-1 labeling ranges for benign, atypical, and anaplastic meningiomas1. It remains undetermined to the association of proliferation and clinical outcomes. Previous studies indicated that there is no correlation between two in all meningioma groups37,38. However, our analysis showed MIB-1 index is a significant prognostic factor for clinical outcome. We report that MIB-1 index >8% was significantly associated with worse OS and RFS in patients with atypical or malignant meningioma. The hazard ratio for OS and RFS are 19.31 (p = 0.005) and 2.89 (p = 0.001), respectively. This result agreed with a previous study that tumor proliferation elevation is correlated with decreased overall survival rate and higher tumor recurrent rate for both atypical and malignant meningiomas39.
Patients and Methods
The records for all patients who were treated for atypical (WHO grade II) and malignant (WHO grade III) meningiomas between June 2001 and November 2009 at Chung Gang Memorial Hospital were retrospectively reviewed. This study was approved by the Chung Gang Memorial Hospital institutional review board, with approval number as 101–4601B. All methods were performed in accordance with the relevant guidelines and regulations.
Each patient’s clinical information was recorded as following: gender; age at diagnosis; tumor location; receipt of pre-operative embolization; extent of tumor resection; tumor pathology; progression or recurrence details; use of postoperative adjuvant radiotherapy; and the length and outcome at follow up. Karnofsky Performance Status (KPS) was determined from clinical notes. Atypical (WHO grade II) and malignant (WHO grade III) meningiomas were diagnosed based on histopathology with the latest 2007 WHO criteria. Older specimens were classified using current criteria retrospectively. Because the goal of this study was to analyze the clinical behavior of de novo atypical and malignant meningiomas, we excluded patients with confounding neurosurgical histories and patients with tumor recurrence after being treated previously for meningiomas. A total of 102 patients were included in this study.
Preoperative Embolization
A neuro-radiologist performed a diagnostic cerebral angiography within three days of operation to assess for hypervascular tumor. Operative neurosurgeon discussed with neuro-radiologist before deciding whether to perform trans-arterial embolization (TAE). TAE procedure involved identifying the tumor’s main supplying artery, guiding a superselective cannulation into the feeding artery with a micro-catheter system, embolizing vessels with permanent particles, and checking for diminished contrast medium tumor stain.
Surgery and Adjuvant Radiotherapy
All patients underwent a surgical resection after diagnosis of atypical and malignant meningioma. The degree of resection was determined using Simpson’s classification and based on the intraoperative impression of the surgeon and the radiographic evidence postoperatively. In our analysis, GTR was equivalent to Simpson Grades 1–3; subtotal removal(STR) was equivalent to Simpson Grade 4. GTR was achieved in 69 patients (67.6%), while 33 patients (32.4%) underwent STR. Radiotherapy (54–60 Gy, delivered in 27–30 fractions) was performed on 42 out of 102 (41.2%) patients following surgical intervention within 6 months of surgery (before any tumor relapse signs with radiographic or clinical evidence).
Follow up evaluation
The mean follow-up time was 77.7 months (range: 5–192 months). We defined disease relapse as recurred tumors after GTR or enlarged residual tumor after STR. Gadolinium-enhanced MRI was used as radiological evidence in all cases assessment. Relapse free survival (RFS) was calculated from the day of GTR to the time of tumor recurrence, or from the day of STR to the time of tumor progression.
Statistical Analysis
Survival and tumor relapse analysis was performed using Kaplan-Meier analysis, and comparisons between groups were performed using log-rank tests. The Cox model was used for continuous variables. A p value < 0.05 was considered statistically significant. Statistically significant risk factors after univariate analysis were subsequently entered into the multivariate analysis to identify risk factors for overall survival and relapse free survival. SPSS software (version 19; SPSS Inc. IBM Corporation) was used to perform statistical analysis.
Limitations
The retrospective design of this study is susceptible to random bias. Although our series is one of the largest series that describes outcomes among patients with atypical and malignant meningiomas, the sample size was insufficiently powered to compare the relative impact of some variables in patients. Second, one single institute data are vulnerable to selection bias and dependent on the local surgical team. These findings may or may not reflect outcomes in meningiomas treated at other hospitals, as observed in the range of OS rates4. Finally, only the initial diagnosis of a tumor is included in our study, which may underestimate the percentage of WHO grade II and grade III meningiomas. Prior studies have demonstrated that around 14% to 29% of recurrent benign tumors will be classified as atypical or malignant meningiomas1,40.
Conclusion
The present retrospective case series using the latest WHO grading system confirmed that malignant meningiomas contributed to poorer overall survival and relapse free survival than atypical lesions. Tumor embolization prior to surgery may be helpful in hyper-vascular lesions and may provide benefit for prognosis without eliciting additional complications. Total excision is recommended for both groups of meningiomas, if no severe complications are expected consequently. Adjuvant radiotherapy following surgical resection is advisable, especially for incompletely excised tumors or tumors located in the parasagittal area or posterior fossa. In addition, higher MIB-1 index (>8%) contributed to worse clinical outcomes. Multicenter, prospective studies are necessary to clarify management and more relevant prognostic factors in atypical and malignant meningiomas.
Additional Information
How to cite this article: Wang, Y.-C. et al. Long Term Surgical Outcome and Prognostic Factors of Atypical and Malignant Meningiomas. Sci. Rep. 6, 35743; doi: 10.1038/srep35743 (2016).
References
Modha, A. & Gutin, P. H. Diagnosis and treatment of atypical and anaplastic meningiomas: a review. Neurosurgery 57, 538–550, discussion 538–550 (2005).
Fuller, G. N. & Scheithauer, B. W. The 2007 Revised World Health Organization (WHO) Classification of Tumours of the Central Nervous System: newly codified entities. Brain Pathol 17, 304–307 (2007).
Louis, D. N. et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114, 97–109 (2007).
Kaur, G. et al. Adjuvant radiotherapy for atypical and malignant meningiomas: a systematic review. Neuro-oncology 16, 628–636 (2014).
Kane, A. J. et al. Anatomic location is a risk factor for atypical and malignant meningiomas. Cancer 117, 1272–1278 (2011).
Pearson, B. E. et al. Hitting a moving target: evolution of a treatment paradigm for atypical meningiomas amid changing diagnostic criteria. Neurosurg Focus 24, E3 (2008).
Goyal, L. K. et al. Local control and overall survival in atypical meningioma: a retrospective study. International journal of radiation oncology, biology, physics 46, 57–61 (2000).
Jo, K. et al. Treatment of atypical meningioma. J Clin Neurosci 17, 1362–1366 (2010).
Scheitzach, J., Schebesch, K. M., Brawanski, A. & Proescholdt, M. A. Skull base meningiomas: neurological outcome after microsurgical resection. Journal of neuro-oncology 116, 381–386 (2014).
Perry, A., Stafford, S. L., Scheithauer, B. W., Suman, V. J. & Lohse, C. M. Meningioma grading: an analysis of histologic parameters. The American journal of surgical pathology 21, 1455–1465 (1997).
Manelfe, C., Lasjaunias, P. & Ruscalleda, J. Preoperative embolization of intracranial meningiomas. AJNR. American journal of neuroradiology 7, 963–972 (1986).
Shah, A. H. et al. The role of preoperative embolization for intracranial meningiomas. Journal of neurosurgery 119, 364–372 (2013).
Probst, E. N., Grzyska, U., Westphal, M. & Zeumer, H. Preoperative embolization of intracranial meningiomas with a fibrin glue preparation. AJNR. American journal of neuroradiology 20, 1695–1702 (1999).
Raper, D. M. et al. Preoperative embolization of intracranial meningiomas: efficacy, technical considerations, and complications. AJNR. American journal of neuroradiology 35, 1798–1804 (2014).
Aghi, M. K. et al. Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery 64, 56–60, discussion 60 (2009).
Combs, S. E., Schulz-Ertner, D., Debus, J., von Deimling, A. & Hartmann, C. Improved correlation of the neuropathologic classification according to adapted world health organization classification and outcome after radiotherapy in patients with atypical and anaplastic meningiomas. International journal of radiation oncology, biology, physics 81, 1415–1421 (2011).
Hug, E. B. et al. Management of atypical and malignant meningiomas: role of high-dose, 3D-conformal radiation therapy. Journal of neuro-oncology 48, 151–160 (2000).
Choi, C. Y. et al. Cyberknife stereotactic radiosurgery for treatment of atypical (WHO grade II) cranial meningiomas. Neurosurgery 67, 1180–1188 (2010).
El-Khatib, M. et al. Stereotactic LINAC radiosurgery for incompletely resected or recurrent atypical and anaplastic meningiomas. Acta Neurochir (Wien) 153, 1761–1767 (2011).
Komotar, R. J. et al. The role of radiotherapy following gross-total resection of atypical meningiomas. Journal of neurosurgery 117, 679–686 (2012).
Hanakita, S. et al. Role of gamma knife surgery for intracranial atypical (WHO grade II) meningiomas. Journal of neurosurgery 119, 1410–1414 (2013).
Lee, K. D. et al. Atypical meningiomas: is postoperative radiotherapy indicated? Neurosurg Focus 35, E15 (2013).
Kshettry, V. R. et al. Descriptive epidemiology of World Health Organization grades II and III intracranial meningiomas in the United States. Neuro-oncology 17, 1166–1173 (2015).
Kallio, M., Sankila, R., Hakulinen, T. & Jaaskelainen, J. Factors affecting operative and excess long-term mortality in 935 patients with intracranial meningioma. Neurosurgery 31, 2–12 (1992).
Perry, A., Scheithauer, B. W., Stafford, S. L., Lohse, C. M. & Wollan, P. C. “Malignancy” in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer 85, 2046–2056 (1999).
Pasquier, D. et al. Atypical and malignant meningioma: outcome and prognostic factors in 119 irradiated patients. A multicenter, retrospective study of the Rare Cancer Network. International journal of radiation oncology, biology, physics 71, 1388–1393 (2008).
Milosevic, M. F., Frost, P. J., Laperriere, N. J., Wong, C. S. & Simpson, W. J. Radiotherapy for atypical or malignant intracranial meningioma. International journal of radiation oncology, biology, physics 34, 817–822 (1996).
Palma, L., Celli, P., Franco, C., Cervoni, L. & Cantore, G. Long-term prognosis for atypical and malignant meningiomas: a study of 71 surgical cases. Journal of neurosurgery 86, 793–800 (1997).
Dziuk, T. W. et al. Malignant meningioma: an indication for initial aggressive surgery and adjuvant radiotherapy. Journal of neuro-oncology 37, 177–188 (1998).
Aizer, A. A. et al. Extent of resection and overall survival for patients with atypical and malignant meningioma. Cancer 121, 4376–4381 (2015).
Wang, Y. C. et al. Skull base atypical meningioma: long term surgical outcome and prognostic factors. Clinical neurology and neurosurgery 128, 112–116 (2015).
Yang, S. Y. et al. Atypical and anaplastic meningiomas: prognostic implications of clinicopathological features. J Neurol Neurosurg Psychiatry 79, 574–580 (2008).
Zaher, A., Abdelbari Mattar, M., Zayed, D. H., Ellatif, R. A. & Ashamallah, S. A. Atypical meningioma: a study of prognostic factors. World Neurosurg 80, 549–553 (2013).
Rosenberg, L. A. et al. Long-term experience with World Health Organization grade III (malignant) meningiomas at a single institution. International journal of radiation oncology, biology, physics 74, 427–432 (2009).
Boskos, C. et al. Combined proton and photon conformal radiotherapy for intracranial atypical and malignant meningioma. International journal of radiation oncology, biology, physics 75, 399–406 (2009).
Bruna, J., Brell, M., Ferrer, I., Gimenez-Bonafe, P. & Tortosa, A. Ki-67 proliferative index predicts clinical outcome in patients with atypical or anaplastic meningioma. Neuropathology 27, 114–120 (2007).
Nakasu, S., Li, D. H., Okabe, H., Nakajima, M. & Matsuda, M. Significance of MIB-1 staining indices in meningiomas: comparison of two counting methods. The American journal of surgical pathology 25, 472–478 (2001).
Torp, S. H., Lindboe, C. F., Granli, U. S., Moen, T. M. & Nordtomme, T. Comparative investigation of proliferation markers and their prognostic relevance in human meningiomas. Clin Neuropathol 20, 190–195 (2001).
Vranic, A., Popovic, M., Cor, A., Prestor, B. & Pizem, J. Mitotic count, brain invasion, and location are independent predictors of recurrence-free survival in primary atypical and malignant meningiomas: a study of 86 patients. Neurosurgery 67, 1124–1132 (2010).
Al-Mefty, O. et al. Malignant progression in meningioma: documentation of a series and analysis of cytogenetic findings. Journal of neurosurgery 101, 210–218 (2004).
Acknowledgements
This research was supported by the grants from Chang Gung Memorial Hospital, Taiwan (Nos CMRPG3D0243 and CIRPG3D0042).
Author information
Authors and Affiliations
Contributions
Y.-C.W., C.-C.C., P.-Y.C. conceived the study. C.-C.C., K.-C.W., C.-N.C., S.-T.L., C.-T.W., Y.-H.H., T.-K.L., P.-W.H. and Y.-C.H. collected and organized the data of neurosurgery. C.-K.T., C.-C.W. and Y.-L.C. integrated the data of radiotherapy and radiology. Y.-C.W. and P.-Y.C. analyzed the data and wrote the paper. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Wang, YC., Chuang, CC., Wei, KC. et al. Long Term Surgical Outcome and Prognostic Factors of Atypical and Malignant Meningiomas. Sci Rep 6, 35743 (2016). https://doi.org/10.1038/srep35743
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep35743
This article is cited by
-
Efficacy of radiotherapy and stereotactic radiosurgery as adjuvant or salvage treatment in atypical and anaplastic (WHO grade II and III) meningiomas: a systematic review and meta-analysis
Neurosurgical Review (2023)
-
NF2 mutations are associated with resistance to radiation therapy for grade 2 and grade 3 recurrent meningiomas
Journal of Neuro-Oncology (2023)
-
Infra-tentorial brain tumor subtypes in children and adults—surgical outcome in an ethnic population with a single regional tertiary center
Chinese Neurosurgical Journal (2022)
-
Landscape of genetic variants in sporadic meningiomas captured with clinical genomics
Acta Neurochirurgica (2022)
-
Outcomes of salvage radiation for recurrent world health organization grade II meningiomas: a retrospective cohort study
Journal of Neuro-Oncology (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
