
Abstract
Recent studies have linked certain single nucleotide polymorphisms in the leucine-rich repeat kinase 2 (LRRK2) gene with Parkinson’s disease (PD). The R1628P variant of LRRK2 may be a specific risk factor for PD in ethnic Han-Chinese populations. This study is to elucidate the epidemiological feature of R1628P in ethnic Han-Chinese population with PD. A comprehensive meta-analysis was performed to evaluate the precise association between R1628P variant and the risk for PD in ethnic Han-Chinese and subgroups stratified by gender, onset age, or family history. The analysis assessing the role of R1628P on the risk of PD in ethnic Han-Chinese supported a significant association, and the odds ratio was 1.86. We further estimate the specific prevalence in relevant ethnic Han-Chinese subgroups. After stratifying the eligible data by gender, onset age, or family history, significant associations were found in all male, female, early-onset, late-onset, familial and sporadic subgroups, and the odds ratio were 1.90, 1.94, 2.12, 1.75, 6.71 and 1.81 respectively. In conclusion, our meta-analysis suggests that R1628P variant of LRRK2 has a significant association with the risk of PD in ethnic Han-Chinese and subgroup population.
Similar content being viewed by others

Introduction
Parkinson’s disease (PD), characterized by the progressive and selective degeneration of substantia nigra dopaminergic neuron, is one of the most common neurodegenerative disorder in the population aged 65 years or older. Although PD was investigated intensely for ages, the pathogenesis of PD still remains indistinct. Genetic and environmental factors maybe play an interactional role in the etiology of PD. However, with the rapid growth of recent studies, genetic factors play a more and more important role in the progression of PD. Over the course of the past decades, some genes increase the risk of PD such as α-synuclein (SNCA), parkin (PARK2), PTEN-induced putative kinase 1 (PINK1), oncogene DJ-1 (DJ-1), leucine-rich repeat kinase 2(LRRK2) and ATPase type 13A2 (ATP13A2) have emerged from previous investigations1,2,3. LRRK2, also named PARK8, consists of 51 coding exons and encodes a lager peptide with 2527 amino acids. It has multiple independent structure domains that contain ARM, ANK (ankyrin repeat), LRR (leucine-rich repeat), Roc (Ras of complex proteins; GTPase), COR(C-terminal of ROC), MAPKKK (mitogen-activated kinase kinase kinase) and WD40 domains4.
Although hundreds of SNPs in LRRK2 are shown in PubMed database, only a few have been verified lead to autosomal dominant PD in the worldwide. The common variants of LRRK2, mainly distribute nearby the kinase domain, include A419V5, R1441C/G/H6, R1628P7, I2012T8, G2019S9, I2020T10, G2385R11 et al. It’s worth nothing that all confirmed pathogenic variants are various in diverse population and different region. The R1628P and G2385R of LRRK2 have been reported to be the most important single nucleotide polymorphism sites that increase the risk of PD in ethnic Han-Chinese populations7,11 while G2019S (c.6050G > A) is common in Europeans. In addition, G2019S variant was rarely among India8, but not detected in Chinese population10,12, Haplotype analysis suggested LRRK2 R1628P variant is more recent than G2385R variant, approximately 2,500 years and 4,000 years ago respectively13,14. Interesting, the R1628P variant of LRRK2 has been discovered as a genetic risk factor for PD in ethnic Han-Chinese population from Taiwan, Singapore, and Mainland China15,16. However, this variant was very rare or absent in Malay (2.3%), Korean (0.8%), Indian (not detected), Japanese (not detected) and Caucasian (0.1%) Parkinsonism5,17,18.
R1628P (c.4883G > C; rs33949390), within the COR domain, was found as the critical genetic risk factor for PD especially among ethnic Han-Chinese population in many previous studies7,11,13,19. However, the results about the association between the R1628P of LRRK2 and PD in ethnic Han-Chinese population were controversial. To clarify whether the R1628P variant was associated with the risk of PD in ethnic Han-Chinese population, we performed a comprehensive meta-analysis to clarify the R1628P variant of LRRK2 whether contributed to the susceptibility of PD, and depicted the epidemiological characteristics between R1628P and PD by subgroup analysis.
Results
Totally, 14 studies7,11,13,15,20,21,22,23,24,25,26,27,28,29 were included from across all the ethnic Han-Chinese population that mainly located in Mainland China, Singapore and Taiwan. Process of searching for and screening studies was showed in Figure S1. Then the 9528 cases and 8707 controls were categorized according to the studies’ available data (male/female, EOPD/LOPD, familial/sporadic). The detailed characteristics of studies which included in the meta-analysis were presented in Table S1 and the sorted data of every group was exhibited in the matching forest plot. Furthermore, The Begg’s test and Egger’s test were correspondingly shown as Figures S2–8 and the publication bias was displayed in Table S2.
Ethnic Han-Chinese population
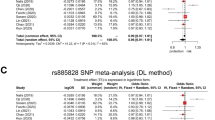
In all, the included studies (14 references) with 9528 patients and 8707 controls examined the association between the R1628P variant and PD among ethnic Han-Chinese population. The main results (Fig. 1) were performed the OR of R1628P that was 1.86 (95% CI: 1.60–2.16, Z = 8.07, P(Z)<10−5) and heterogeneity test for whole studies indicated no significant between-study heterogeneity (χ2 = 18.48, df = 13, P = 0.14 > 0.10, I2 = 30%). Furthermore, the Begg’s test and Egger’s test were also implied no significant heterogeneity (Figure S2). Thus, significant association between R1628P and PD was discovered by using fixed effect model in ethnic Han-Chinese population.

Forest plot of meta-analysis for R1628P in ethnic Han-Chinese population.
Male/Female
We next analysis the available studies7,11,25,26,28 to identify the gender whether influence the outcome of PD with R1628P in LRRK2. The association of R1628P with PD remained significant in male (Fig. 2A) and female (Fig. 2B), major outcomes are OR = 1.90 (95% CI: 1.11–3.26, Z = 2.33, P(Z) = 0.02. Heterogeneity: χ2 = 11.21, df = 4, P = 0.02, I2 = 64%) and OR = 1.94 (95% CI: 1.40–2.69, Z = 3.96, P(Z) < 10−4. Heterogeneity: χ2 = 5.14, df = 4, P = 0.27, I2 = 22%), respectively.

Forest plot of meta-analysis for R1628P in (A) Male and (B) Female ethnic Han-Chinese population.
Early-onset PD (EOPD)/Late-onset PD (LOPD)
We have got together 5 studies7,11,25,26,28 from ethnic Han-Chinese population to analysis the age of onset that influenced the susceptibility of PD that occur R1628P. In this stratified analysis, the OR with EOPD (OR = 2.12, 95% CI: 1.42–3.17, Z = 3.69, P(Z) = 0.0002, Fig. 3A) was mildly higher than that with LOPD (OR = 1.75, 95% CI: 1.05–2.93, Z = 2.15, P(Z) = 0.03, Fig. 3B). The R1628P variant with EOPD and LOPD were both significantly risk factor for PD.

Forest plot of meta-analysis for R1628P in ethnic Han-Chinese population of (A) EOPD and (B) LOPD.
Familial/Sporadic
Only 2 studies7,22 in ethnic Han-Chinese with familial PD and 11 studies7,11,15,20,21,23,24,25,26,27,28 in ethnic Han-Chinese with sporadic PD were analyzed to evaluate the overall level for association between familial (Fig. 4A) or sporadic (Fig. 4B) PD and R1628P variant. The pooled OR of these analysis respectively were 6.71 (95% CI: 0.57–79.02, Z = 1.51, P(Z) = 0.13 > 0.05. Heterogeneity: τ2 = 2.16, χ2 = 2.48, df = 1, P = 0.12 > 0.10, I2 = 60%) with 82 cases and 602 controls, 1.81 (95% CI: 1.53–2.15, Z = 6.83, P(Z) <10−5. Heterogeneity: χ2 = 14.41, df = 10, P = 0.15 > 0.10, I2 = 31%) with 7443 cases and 6661 controls.

Forest plot of meta-analysis for R1628P in ethnic Han-Chinese population of (A) familial and (B) sporadic PD.
Discussion
In the current study, we performed a comprehensive meta-analysis to clarify the epidemiological characteristics between R1628P variant and PD among ethnic Han Chinese population, and the specific prevalence in relevant ethnic Han Chinese subgroups, stratified by gender, onset age, or family history. A total of 14 eligible studies were included in the meta-analysis involving 9528 cases and 8707 controls. The literature selection process was showed in Figure S1. The main study characteristics of this meta-analysis were summarized in Table S1 respectively. The Odds Ratio (OR) of the R1628P allele and genotype contrasts in ethnic Han-Chinese population was 1.86 (95% CI: 1.60–2.16) using fixed effects model (Fig. 1). In the male and female subgroup, the OR is 1.90 (95% CI: 1.11–3.26) (Fig. 2A), and 1.94 (95% CI: 1.40–2.69) (Fig. 2B) respectively. In the stratified analysis according to onset age, the allele frequency in patients with early-onset PD (EOPD) or late-onset PD (LOPD) were significantly higher than that in controls with ORs of 2.12 (95% CI: 1.42–3.17) (Fig. 3A) and 1.75 (95% CI: 1.05–2.93) (Fig. 3B). When stratified by family history, the pooled OR was 6.71 (95% CI: 0.57–79.02) (Fig. 4A) in familial PD subgroup, and 1.81 (95% CI: 1.53–2.15) (Fig. 4B) in the sporadic PD subgroup. Publication bias analysis for all studies implied no significant heterogeneity and bias except LOPD (Table S2).
As our previously published study30, we have suggested that LRRK2 R1628P variant could robustly increase the binding affinity of LRRK2 with Cyclin-dependent kinase 5 (Cdk5), a multifaceted kinase in neurodegenerative diseases. Interestingly, R1628P variant turned its adjacent amino acid residue S1627 on LRRK2 protein to a novel phosphorylation site of Cdk5, which could be defined as a typical type II ( + ) phosphorylation-related single nucleotide polymorphism31. Importantly, we showed that the phosphorylation of S1627 by Cdk5 could activate the LRRK2 kinase, and consequently cause neuronal death. Combined with this meta-analysis study, our findings not only indicated the epidemiological characters of R1628P variant of LRRK2 in ethnic Han-Chinese population, but also elucidated the molecular mechanism underlying genotype-environment interaction-related LRRK2 R1628P variant in neuronal death in LRRK2-linked PD and provide a novel therapeutic target for drug design or genetic modulation.
Two limitations should be mentioned in our meta-analysis results. Firstly, all the included studies focused on pathogenic LRRK2 R1628P variant were performed by clinical-based case-control studies. Although case-control studies are relatively simple to conduct and do not require a long follow-up period, the community-based cohort studies provide the best information about the causation of disease. Secondly, in the meta-analysis, between-study heterogeneity was tested by the χ2-based Q-statistic, I2 index and Z score; random effect model was performed if I2 index is more than 50%. Only two studies of familial PD were included in this analysis, and the I2 index of between-study heterogeneity was more than 50%. The reliability of OR in familial PD subgroup was relatively low, and larger well-designed studies should be encouraged to elucidate the potential pathogenesis in familial PD with R1628P variant. Nevertheless, given over one billion population base of ethnic Han-Chinese, the carriers of R1628P variant are approximate 40–50 million, and precise elucidation of distribution patterns and molecular pathology of R1628P variant is still tremendously profitable to the personalized medical intervention of PD in ethnic Han-Chinese population.
Methods
Literature search
We searched PubMed, Web of Science, Medline up to January 1th 2016 for all English language publications, CNKI (China National Knowledge Infrastructure) and CQVIP database for all Chinese language studies by using the following search terms: [(LRRK2 OR “leucine-rich repeat kinase 2” OR PARK8) AND (R1628P OR rs33949390 OR “c.4883G > C”) AND (“PD”)]. Studies using overlapping samples were excluded. In addition, case reports, reviews and editorials were not included.
Selection criteria
Only those studies assessing the association between LRRK2 R1628P variants and PD were included. For inclusion, eligible studies had to meet all of the following criteria: (1) be a case control or cohort study; (2) be published in a peer-reviewed journal; (3) have original data being independent from other studies, if the authors come from the same affiliation or an author has at least two publications, the corresponding authors were contacted to confirm whether the data was published repeatedly; (4) the subjects of control group has no history of mental disorders. For exclusion, the criteria as follows: (1) articles without case-control studies such as retrospective studies, reviews, and case reports; (2) other disease such as Alzheimer’s disease, Huntington’s disease; (3) studies have no sufficient data to calculate the odds ratio (OR) with its 95% confidence interval and p value.
Data extraction
All the studies were screening by two independent reviewers. The disagreement of some studies was resolved through evaluating the records by the Newcastle-Ottawa Scale (NOS, Cochrane reviewers’ handbook) and discussion. The following features were collected form all the including studies: first author, year of publication, ethnicity, location, genotyping method, numbers of case and control group and Hardy-Weinberg Equilibrium (Table S1). And collecting the detailed data of each study such as early-onset PD (EOPD) as age at onset <50 years, and late-onset PD (LOPD) as ≥ 50 years, male/female or familial/sporadic if the data was available or calculative.
Statistical analysis
In all analysis, odds ratio (OR) with its 95% confidence interval (CI) was used to assess the strength of association between the LRRK2 R1628P variants and PD risk. Between-study heterogeneity was tested by the χ2-based Q-statistic and quantified by I2 as a measure of the proportion of variance between the study-specific estimates that is attributable to between-study difference rather than random variation. Z score was conducted to test the overall effect and the significance set at P ≤ 0.05 (two-tailed test). The heterogeneity is considered statistically significant if PQ ≤ 0.10, we used the DerSimonian and Laird random effect model (D-L REM); otherwise, the Mantel-Haenszel fixed effect model (FEM) was used. All the forest plots and Begg’s funnel plot were display using Review Manager Software 5.2 (The Cochrane Collaboration). Sensitivity analysis was performed by leaving one out method to assess the stability of the results. Publication bias in each meta-analysis was detected by Begg’s funnel plots and Begg’s test (Stata v12.0).
In addition, subgroup analysis was performed according to gender, onset age and family history for all studies. In the analysis of the onset age of PD for R1628P, we defined EOPD/LOPD (cutoff point: 50 years) according to the commonly used standard. 95% CIs were constructed using Woolf’s method. The Z test was used to determine the significance of the pooled OR.
Additional Information
How to cite this article: Zhang, P. et al. Association of LRRK2 R1628P variant with Parkinson’s disease in Ethnic Han-Chinese and subgroup population. Sci. Rep. 6, 35171; doi: 10.1038/srep35171 (2016).
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Klein, C. & Ziegler, A. From GWAS to clinical utility in Parkinson’s disease. Lancet 377, 613–614, doi: 10.1016/S0140-6736(11)60062-7 (2011).
Li, N. N. et al. GWAS-linked GAK locus in Parkinson’s disease in Han Chinese and meta-analysis. Human genetics 131, 1089–1093, doi: 10.1007/s00439-011-1133-3 (2012).
Rhodes, S. L., Sinsheimer, J. S., Bordelon, Y., Bronstein, J. M. & Ritz, B. Replication of GWAS associations for GAK and MAPT in Parkinson’s disease. Annals of human genetics 75, 195–200, doi: 10.1111/j.1469-1809.2010.00616.x (2011).
Soto-Ortolaza, A. I. et al. GWAS risk factors in Parkinson’s disease: LRRK2 coding variation and genetic interaction with PARK16. American journal of neurodegenerative disease 2, 287–299 (2013).
Ross, O. A. et al. Association of LRRK2 exonic variants with susceptibility to Parkinson’s disease: a case-control study. The Lancet. Neurology 10, 898–908, doi: 10.1016/S1474-4422(11)70175-2 (2011).
de Ynigo-Mojado, L., Martin-Ruiz, I. & Sutherland, J. D. Efficient allele-specific targeting of LRRK2 R1441 mutations mediated by RNAi. PloS one 6, e21352, doi: 10.1371/journal.pone.0021352 (2011).
Fu, X. et al. LRRK2 G2385R and LRRK2 R1628P increase risk of Parkinson’s disease in a Han Chinese population from Southern Mainland China. Parkinsonism & related disorders 19, 397–398, doi: 10.1016/j.parkreldis.2012.08.007 (2013).
Tomiyama, H. et al. Clinicogenetic study of mutations in LRRK2 exon 41 in Parkinson’s disease patients from 18 countries. Movement disorders : official journal of the Movement Disorder Society 21, 1102–1108, doi: 10.1002/mds.20886 (2006).
Clark, L. N. et al. Frequency of LRRK2 mutations in early- and late-onset Parkinson disease. Neurology 67, 1786–1791, doi: 10.1212/01.wnl.0000244345.49809.36 (2006).
Lu, C. S. et al. The LRRK2 I2012T, G2019S, and I2020T mutations are rare in Taiwanese patients with sporadic Parkinson’s disease. Parkinsonism & related disorders 11, 521–522, doi: 10.1016/j.parkreldis.2005.09.003 (2005).
Cai, J. et al. Association between G2385R and R1628P polymorphism of LRRK2 gene and sporadic Parkinson’s disease in a Han-Chinese population in south-eastern China. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 34, 2001–2006, doi: 10.1007/s10072-013-1436-3 (2013).
Fung, H. C. et al. Lack of G2019S LRRK2 mutation in a cohort of Taiwanese with sporadic Parkinson’s disease. Movement disorders : official journal of the Movement Disorder Society 21, 880–881, doi: 10.1002/mds.20814 (2006).
Ross, O. A. et al. Analysis of Lrrk2 R1628P as a risk factor for Parkinson’s disease. Annals of neurology 64, 88–92, doi: 10.1002/ana.21405 (2008).
Farrer, M. J. et al. Lrrk2 G2385R is an ancestral risk factor for Parkinson’s disease in Asia. Parkinsonism & related disorders 13, 89–92, doi: 10.1016/j.parkreldis.2006.12.001 (2007).
Wu, Y. R. et al. Genetic variants ofLRRK2 in Taiwanese Parkinson’s disease. PloS one 8, e82001, doi: 10.1371/journal.pone.0082001 (2013).
Kumar, P. M. et al. Differential effect of caffeine intake in subjects with genetic susceptibility to Parkinson’s Disease. Scientific reports 5, 15492, doi: 10.1038/srep15492 (2015).
Tan, E. K. et al. Lrrk2 R1628P in non-Chinese Asian races. Annals of neurology 64, 472–473, doi: 10.1002/ana.21467 (2008).
Kim, J. M. et al. The LRRK2 G2385R variant is a risk factor for sporadic Parkinson’s disease in the Korean population. Parkinsonism & related disorders 16, 85–88, doi: 10.1016/j.parkreldis.2009.10.004 (2010).
Wang, X., Zhang, X., Xue, L. & Xie, A. The association between the LRRK2 R1628P variant and the risk of Parkinson’s disease in Asian: a meta-analysis. Neuroscience letters 623, 22–27, doi: 10.1016/j.neulet.2016.04.056 (2016).
Lu, C. S. et al. The LRRK2 Arg1628Pro variant is a risk factor for Parkinson’s disease in the Chinese population. Neurogenetics 9, 271–276, doi: 10.1007/s10048-008-0140-6 (2008).
Tan, E. K. et al. LRRK2 R1628P increases risk of Parkinson’s disease: replication evidence. Human genetics 124, 287–288, doi: 10.1007/s00439-008-0544-2 (2008).
Wang, L. et al. A novel LRRK2 mutation in a mainland Chinese patient with familial Parkinson’s disease. Neuroscience letters 468, 198–201, doi: 10.1016/j.neulet.2009.10.080 (2010).
Wang, C. et al. Penetrance of LRRK2 G2385R and R1628P is modified by common PD-associated genetic variants. Parkinsonism & related disorders 18, 958–963, doi: 10.1016/j.parkreldis.2012.05.003 (2012).
Wu-Chou, Y. H. et al. Genetic variants of SNCA and LRRK2 genes are associated with sporadic PD susceptibility: a replication study in a Taiwanese cohort. Parkinsonism & related disorders 19, 251–255, doi: 10.1016/j.parkreldis.2012.10.019 (2013).
Yu, L. et al. LRRK2 R1628P contributes to Parkinson’s disease susceptibility in Chinese Han populations from mainland China. Brain research 1296, 113–116, doi: 10.1016/j.brainres.2009.08.047 (2009).
Zhang, Z. et al. LRRK2 R1628P variant is a risk factor of Parkinson’s disease among Han-Chinese from mainland China. Movement disorders : official journal of the Movement Disorder Society 24, 1902–1905, doi: 10.1002/mds.22371 (2009).
Zhou, Y. et al. Association of Parkinson’s disease with six single nucleotide polymorphisms located in four PARK genes in the northern Han Chinese population. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 19, 1011–1015, doi: 10.1016/j.jocn.2011.09.028 (2012).
Wang, L. Polygenic determinants of Parkinson’s disease and the establishment of autosomal dominant Parkinson’s Disease genetic diagnosis platform. Thesis (2011).
Paing, S., Carson, A. J., Zhao, Y., Prakash, K. M. & Tan, E. K. Interaction Between Caffeine Intake and LRRK2 Genetic Variants in Parkinson’s Disease. Annals of the Academy of Medicine, S4–S4 (2013).
Shu, Y. et al. Parkinson-Related LRRK2 Mutation R1628P Enables Cdk5 Phosphorylation of LRRK2 and Upregulates Its Kinase Activity. PloS one 11, e0149739, doi: 10.1371/journal.pone.0149739 (2016).
Ren, J. et al. PhosSNP for systematic analysis of genetic polymorphisms that influence protein phosphorylation. Molecular & cellular proteomics : MCP 9, 623–634, doi: 10.1074/mcp.M900273-MCP200 (2010).
Acknowledgements
This work was supported financially by National Natural Science Foundation of China (Nos 31371384, 31571044 to B.T. and No. 31600821 to P.Z.), Program for New Century Excellent Talents in University (No. NCET-10-0415 to B.T.), and China Postdoctoral Scientific Foundation (No. 2015M582226 to P.Z.).
Author information
Authors and Affiliations
Contributions
All authors contributed significantly to this work. P.Z. and B.T. designed the research study; F.H., F.J., Q.Z. and L.C. collected and P.Z., Q.W. and J.Y. analyzed the data. P.Z. and B.T. wrote the paper and prepared all the figures and tables. Additionally, all authors have approved the final draft.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhang, P., Wang, Q., Jiao, F. et al. Association of LRRK2 R1628P variant with Parkinson’s disease in Ethnic Han-Chinese and subgroup population. Sci Rep 6, 35171 (2016). https://doi.org/10.1038/srep35171
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep35171
This article is cited by
-
SNCA but not DNM3 and GAK modifies age at onset of LRRK2-related Parkinson’s disease in Chinese population
Journal of Neurology (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
