
Abstract
Breast cancer is the most common cancer in women. However, it remains unproven whether psychological factors have an influence on breast cancer incidence. In our earlier study, subjects possessing two personality traits, decisiveness and “ikigai” (a Japanese word meaning something that makes one’s life worth living), showed a significantly lower risk of developing breast cancer, although no psychological factors have been convincingly demonstrated to have an influence on breast cancer development in other studies. Therefore, we conducted this follow-up analysis to confirm the association between breast cancer incidence and psychological traits, using the final dataset of a large-scale prospective cohort study in Japan. We identified 209 cases of incident breast cancer out of a maximum 21-year follow-up of 29,098 Japanese women. Cox proportional hazard regression analysis, adjusted for the same potential confounders used in our previous study, did not reveal any significant relationships between breast cancer incidence and four psychological traits: having “ikigai”, decisiveness, ease of anger arousal and perceived stress. Our finding is consistent with previous studies and suggests that the psychological traits are unlikely to be an important risk factor for breast cancer.
Similar content being viewed by others


Introduction
Breast cancer is the most common cancer in women worldwide1, as well as in Japan2. A number of breast cancer risk factors have been established, including age at menarche and menopause, obesity, height, regular exercise, nutrition and family history of breast cancer3,4,5,6,7. In contrast, it remains unproven whether psychological factors have an influence on breast cancer incidence, though many cohort studies and systematic reviews have examined various psychological factors on this topic, including life events8,9,10, personality traits11,12,13,14,15,16,17, coping style14,15,18, perceived stress19,20 and depression21,22,23, over the past 30 years.
Two potential mechanisms are proposed to explain how these psychological factors work to increase cancer risk. The first is via altering the immune and endocrine systems and the second is via altering behaviors such as sleep, excecise, diet, smoking, alchohol consumption, drug use and poor adherence to medical regimens24,25. Studies evaluating relevance of psychological factors to carcinogenesis have most often examined the role of personality and stress as risk factors in cancer. Of the cancer sites that have been studied from this perspective, breast cancer is one that has received a great deal of attention26. Therefore, we focused on a possible contribution of personality traits and perceived stress to breast cancer development in the present study. In our earlier study, two psychological traits, “having something to live for” and “perceiving oneself as quick to judge”, showed a significantly lower risk of developing breast cancer. The other two traits, “ease of anger arousal” and “perceived stress”, did not show an association with breast cancer incidence12. Precisely, to indicate “something to live for”, we used the Japanese word, “ikigai” in the survey. Although “ikigai” has not been well defined in the scientific literature, this term is used to refers to 1) a specific experience that creates a sense of worth and happiness, 2) the resultant cognitive evaluation that finds one’s life meaning because of the experience and 3) the sense of fulfillment and joy that is derived from the cognitive evaluation27. Thus, we used “ikigai” to represent this construct throughout the manuscript. Notably, this construct, “ikigai” was shown to be associated with mortality in another study using the same cohort in the present study28.
Recently, an elaborate meta-analysis using pooled data from six cohort studies revealed that personality was not associated with an increased risk of all cancers and site-specific cancers including breast cancer11. This meta-analysis was conducted on this topic comprehensively, using a general personality framework called the five-factor model, which is accepted in modern personality psychology29. As for perceived stress, the meta-analysis showed that stress-related psychosocial factors were not associated with an increased risk of breast cancer incidence19.
One limitation of these studies was the relatively short follow-up period (e.g., mean follow-up of 5.4 years in the former meta-analysis and follow-up of 7–9 years in our previous study). Empirical studies demonstrated that it may take approximately 14 years for breast cancer to grow from the first tumor cell into a detectable lump and, thus, studies with these time frames are likely to underestimate associations with breast cancer incidence30,31. In fact, a meta-analysis found that cohort studies with a longer follow-up showed a stronger association between depression and breast cancer incidence23. Therefore, we conducted a maximum of 21 year follow-up analysis to confirm the association between breast cancer incidence and psychological traits using the final dataset of a large-scale prospective cohort study, the Japan Collaborative Cohort (JACC) Study32.
Methods
Study population
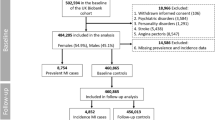
A baseline survey of the JACC Study was conducted in 45 areas throughout Japan. A total of 110,585 subjects (46,395 men and 64,190 women) aged 40–79 were enrolled between 1988 and 1990. The details of the study procedure were described elsewhere32.
This study excluded 23 study areas where information on cancer incidence at follow-up or psychological traits at baseline were not available. Furthermore, 247 subjects were excluded because of positive histories of breast cancer. Another 9,268 subjects were excluded because all of their data on psychological traits at baseline were missing. Thus, a total of 29,098 women were included in this study.
Informed consent was obtained individually from each participant, except in a few study areas where informed consent was obtained at the group level after the purpose of the study and confidentiality of the data had been explained to community leaders. The JACC Study begun before the ethical guideline was first established by Japanese government in 2002 and the Japanese ethical guideline allows such established epidemiological studies to continue without obtaining additional personal informed consents33,34,35. This study was approved by the ethics board at Nagoya University School of Medicine, where the central office of JACC Study was located28.
Baseline Measuement
At baseline, we used a self-administered questionnaire to obtain information on demographics. medical history, tabacco and alcohol use, psychical activity, psychological traits and other lifestyle factors. Psychological traits were measured using four questions at balseline: having “ikigai” (do you have “ikigai”, something to live for?), decisiveness (do you make decisions quickly?), ease of anger (are you easily angered?) and perceived stress (do you experience stress during your daily life?), with three- or four-point Likert-type response options (Table 1).
Potential confounders were also measured using the questionnaire at baseline; they are detailed in the statistical analysis section below.
Outcome ascertainment
Follow-up was conducted from enrollment until the end of 2009 in all areas, except three areas where follow-up was terminated at the end of 1999. During this period, population registries in the municipalities were used to ascertain the residential and vital status of the subjects. In Japan, registration of death is required by Family Registration Law and theoretically provides complete mortality data. The cause and date of death of subjects were annually or biannually confirmed by death certificates in each area. The date of move-out of cohort members from the study area was also annually or biannually verified by the investigator in cooperation with the local governmental office.
We ascertained the incidence of cancer by linking to records of population-based cancer registries, supplemented by a systematic review of death certificates. In some study areas, medical records in major local hospitals were also reviewed36.The cancer incidence data were coded according to the 10th Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). We defined breast cancer as C50.0 to C50.9 and do not classify breast cancer based on histopathology or molecular subtypes37.
Statistical analysis
According to psychological traits responses, the baseline subject characteristics were summarized as percentage for categorical data and mean for continuous data with corresponding 95% confidence intervals (95% CI). Psychological trait variables were treated as ordinal variables for all analyses. and Spearman’s correlation coefficients among psychological traits were estimated with 95% CI. The person-years of follow-up were calculated from the baseline to the following events: diagnosis of breast cancer, death from any causes, emigration outside the study area, or the end of follow-up (the latter three events were treated as censored).
The hazard rations (HR) with the 95% CI for breast cancer incidence were estimated using Cox proportional hazards regression models. For estimating HR, we used age (using 10-year age groups) as an independent variable. We also used the following potential confounding variables used in the previous study12: age (using 10-year age groups); area (Hokkaido, Tohoku, Kanto, Chubu, Kinki, Chugoku, or Kyushu); educational level (attended school until the age of ≤15, 16–18, ≥19 years); family history of breast cancer in mother or sisters (yes or no); age at menarche (≤13, 14–15, 16–17 or ≥18 years); age at menopause (premenopausal at baseline, ≤44, 45–49 or ≥50 years); age at time of first birth (≤24, 25–29 or ≥30 years); number of times of giving birth or parity (0, 1, 2, 3 or ≥4); use of exogenous female hormones (yes or no); alcohol consumption (never drink, ex-drinker, or current drinker consuming <15 or ≥15 g of ethanol daily); consumption of green leafy vegetables (≤2 times/week, 3–4 times/week or almost every day); daily walking habits (seldom or never, or <30, 30–59 or ≥60 min/day); exercise (seldom or never, 1–2, 3–4 or ≥5 h/week); sedentary work (yes or no); height (<150.0, 150.0–159.9 or ≥160.0 cm); and baseline body-mass index (BMI; <20.0, 20.0–24.9, 25.0–29.9 or ≥30.0 kg/m2). In the Cox regression analysis, missing values for each covariate were treated as an additional category in the variable. The proportional hazards assumption was checked by visual inspection of the log-log Kaplan–Meier curves.
All p-values were two-sided and the significance level was set to 0.05. All analyses were performed using SAS version 9.3 (SAS institute Inc., Cary, NC, USA).
Results
Correlations are moderate among the four psychological traits as shown in Table 2, where the absolute values of Spearman’s correlation coefficients range from 0.03 to 0.32. Therefore, we examined each psychological trait separately for association with breast cancer incidence.
Baseline characteristics of the study population are summarized in Table 1 according to each psychological trait response. For each response regarding psychological traits, no change was shown in some of the characteristics, such as age at menarche, menopause and first birth, as well as parity and height, evidenced by overlapping 95% CI of these variables for each response. The other characteristics showed a contrast between having “ikigai” or decisiveness and ease of anger or perceived stress. This general pattern was observed in the following variables: daily consumer of green leafly vegetables, walking and exercise. Furthermore, use of exogenous female hormone was nearly aligned with this pattern of contrast, although exceptions occurred in the other variables. Of these exceptional variables, age, education, sedentary work and BMI were almost identically distributed among all psychological traits.
During a maximum 21-year follow-up (a mean follow-up of 12.8 years and 372,156 person-years), 209 cases of incident breast cancer were ascertained. As shown in Table 3, in the Cox regression analysis adjusted for sex, none of the psychological traits were significantly related to the risk of breast cancer. This finding remained basically unchanged after adjustment for the other potential confounders used in our previous study12. In the previous study, psychological traits responses were dichotomized for Cox regression analyses. Just to compare with the results from that study, therefore, we dichotomized the psychological traits responses for Cox regression. Again, none of the psychological traits were significantly related to the risk of breast cancer (Supplementary Table 1).
Discussion
Our large-scale prospective cohort study with 19–21 years of follow-up did not reveal any significant relationships between breast cancer incidence and the four psychological traits: having “ikigai”, decisiveness, ease of anger arousal and perceived stress.
In the previous study using the first 7–9 years follow-up data of the same cohort, two psychological traits. having “ikigai” and decisiveness, had a nominally significant association with breast cancer incidence12. However, this association disappeared after another 12 years of follow-up, even though three or four-point Likert-type responses were dichotomized in the same way as in the previous study (Supplementary Table 1). This inconsistency might have occurred because the previous study conducted statistical tests for four items, which led to type I error inflation. That is, the effects of psychological traits on the development of breast cancer are so negligible that the present study cannot detect them, but the previous study might have spuriously detected the effect due to multiple testing. Alternately, the inconsistent results might have occurred owing to different follow-up duration between our earlier and present studies. Because personality traits and perceived stress continue to change over time38,39,40, the longer follow-up duration, the weaker the effect of these traits on breast cancer incidence. Therefore, the present study with a longer follow-up might miss the effect of psychological traits that could be detected in the earlier study.
A clinically detectable tumor contains at least 109 cells and the doubling time for primary breast cancer tumors is estimated to be 105–270 days30,41; thus, it should take 8.6–13.9 years to grow from the first tumor cell to a detectable tumor. Therefore, to allow for a sufficient incubation period of breast cancer, we focused on previous cohort studies with more than 13 years of follow-up that examined the association between breast cancer incidence and any personality traits. To our knowledge, there are three such studies and all of them revealed no significant increase of breast cancer risk by any personality traits examined13,16,17. Considering these findings together with the results of the present study, the overall findings are largely reassuring that the psychological traits do not have a substantial role in the etiology of breast cancer.
The construct “ikigai” indicates the source of value in one’s life or the things that make one’s life worthwhile. This construct is noteworthy because it was repeatedly shown to be associated with mortality in another study using the same cohort in the current28 and other studies42,43,44. In these studies, the increase in mortality was attributed to an increase in the mortality from cardiovascular disease and external causes, but not to the mortality from cancer28,42,43. The latter finding is in agreement with the present study. This study had some limitations. The most important limitation concerns the measures of the four constructs examined here. We used only one item to measure each construct. Compared to a multiple-item measure, single-item measures might be more influenced by random measurement error, which could attenuate the true association between breast cancer incidence and each item and, thus, decrease the power to detecting the association45. This may be one of the reasons why we failed to obtain any significant results. Furthermore, these single-item measures were not shown to be valid, although they have face validity. That is, we are not confident in what these items measure in fact. Especially, the definition of “ikigai” has not been agreed upon in the scientific literature and its construct validity still needs to be established. Another measurement problem is that the four psychological traits were measured only at baseline. This approach cannot address the influence of the traits over time and thus a repeated measures design could uncover its influence on breast cancer incidence that would otherwise be missed. Finally, for identification of breast cancer in the present study, population-based cancer registries were not available in four out of 24 study areas; instead, medical records in local hospitals were reviewed in the four areas. The unsystematic identification of cancer cases in the small portion of study areas could cause a systematic error.
Therefore, future studies should follow-up for a period long enough to grasp the whole picture of breast cancer development, using well-validated questionnaires to measure psychological traits.
Conclusion
This large-scale prospective cohort study failed to find any significant association between the four psychological traits examined and breast cancer incidence in Japan. The fact that the psychological traits are unlikely to be an important risk factor for breast cancer may be a comfort to women who are otherwise concerned about the risk of personality traits leading to breast cancer.
Additional Information
How to cite this article: Sawada, T. et al. The influence of personality and perceived stress on the development of breast cancer: 20-year follow-up of 29,098 Japanese women. Sci. Rep. 6, 32559; doi: 10.1038/srep32559 (2016).
References
Torre, L. A. et al. Global cancer statistics, 2012. CA. Cancer J. Clin. 65, 87–108 (2015).
Inari, H. et al. A comparison of clinicopathological characteristics and long-term survival outcomes between symptomatic and screen-detected breast cancer in Japanese women. Breast Cancer Tokyo Jpn. (2016).
Tyrer, J., Duffy, S. W. & Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat. Med. 23, 1111–1130 (2004).
Curtis, C. et al. The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups. Nature 486, 346–352 (2012).
Hulka, B. S. & Moorman, P. G. Breast cancer: hormones and other risk factors. Maturitas 38, 103–113 discussion 113–116 (2001).
van den Brandt, P. A. et al. Pooled analysis of prospective cohort studies on height, weight and breast cancer risk. Am. J. Epidemiol. 152, 514–527 (2000).
Santen, R. J. et al. Critical assessment of new risk factors for breast cancer: considerations for development of an improved risk prediction model. Endocr. Relat. Cancer 14, 169–187 (2007).
Duijts, S. F. A., Zeegers, M. P. A. & Borne, B. V. The association between stressful life events and breast cancer risk: a meta-analysis. Int. J. Cancer 107, 1023–1029 (2003).
Petticrew, M., Bell, R. & Hunter, D. Influence of psychological coping on survival and recurrence in people with cancer: systematic review. BMJ 325, 1066 (2002).
Michael, Y. L. et al. Influence of stressors on breast cancer incidence in the Women’s Health Initiative. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 28, 137–146 (2009).
Jokela, M. et al. Is personality associated with cancer incidence and mortality?An individual-participant meta-analysis of 2156 incident cancer cases among 42 843 men and women. Br. J. Cancer 110, 1820–1824 (2014).
Wakai, K. et al. Psychological attitudes and risk of breast cancer in Japan: a prospective study. Cancer Causes Control CCC 18, 259–267 (2007).
Bleiker, E. M. A., Hendriks, J. H. C. L., Otten, J. D. M., Verbeek, A. L. M. & van der Ploeg, H. M. Personality factors and breast cancer risk: a 13-year follow-up. J. Natl. Cancer Inst. 100, 213–218 (2008).
Butow, P. N. et al. Epidemiological evidence for a relationship between life events, coping style and personality factors in the development of breast cancer. J. Psychosom. Res. 49, 169–181 (2000).
Aro, A. R. et al. Psychological risk factors of incidence of breast cancer: a prospective cohort study in Finland. Psychol. Med. 35, 1515–1521 (2005).
Nakaya, N. et al. Personality traits and cancer risk and survival based on Finnish and Swedish registry data. Am. J. Epidemiol. 172, 377–385 (2010).
Lillberg, K., Verkasalo, P. K., Kaprio, J., Helenius, H. & Koskenvuo, M. Personality characteristics and the risk of breast cancer:A prospective cohort study. Int. J. Cancer 100, 361–366 (2002).
Svensson, T. et al. Coping strategies and cancer incidence and mortality: The Japan Public Health Center-based prospective study. Cancer Epidemiol. 40, 126–133 (2016).
Chida, Y., Hamer, M., Wardle, J. & Steptoe, A. Do stress-related psychosocial factors contribute to cancer incidence and survival?Nat. Clin. Pract. Oncol. 5, 466–475 (2008).
Helgesson, O., Cabrera, C., Lapidus, L., Bengtsson, C. & Lissner, L. Self-reported stress levels predict subsequent breast cancer in a cohort of Swedish women. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. ECP 12, 377–381 (2003).
Oerlemans, M. E., van den Akker, M., Schuurman, A. G., Kellen, E. & Buntinx, F. A meta-analysis on depression and subsequent cancer risk. Clin. Pract. Epidemiol. Ment. Health CP EMH 3, 29 (2007).
Liang, J.-A. et al. The analysis of depression and subsequent cancer risk in Taiwan. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 20, 473–475 (2011).
Pössel, P., Adams, E. & Valentine, J. C. Depression as a risk factor for breast cancer: investigating methodological limitations in the literature. Cancer Causes Control CCC 23, 1223–1229 (2012).
Cohen, S. & Rodriquez, M. S. Pathways linking affective disturbances and physical disorders. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 14, 374–380 (1995).
Spiegel, D. & Kato, P. M. Psychosocial influences on cancer incidence and progression. Harv. Rev. Psychiatry 4, 10–26 (1996).
McKenna, M. C., Zevon, M. A., Corn, B. & Rounds, J. Psychosocial factors and the development of breast cancer: a meta-analysis. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 18, 520–531 (1999).
Mathews, G. What Makes Life Worth Living?: How Japanese and Americans Make Sense of Their Worlds. (University of California Press, 1996).
Tanno, K. et al. Associations of ikigai as a positive psychological factor with all-cause mortality and cause-specific mortality among middle-aged and elderly Japanese people: findings from the Japan Collaborative Cohort Study. J. Psychosom. Res. 67, 67–75 (2009).
McCrae, R. R. & Costa, P. T. Validation of the five-factor model of personality across instruments and observers. J. Pers. Soc. Psychol. 52, 81–90 (1987).
Friberg, S. & Mattson, S. On the growth rates of human malignant tumors: implications for medical decision making. J. Surg. Oncol. 65, 284–297 (1997).
Spratt, J. S., Meyer, J. S. & Spratt, J. A. Rates of growth of human neoplasms: Part II. J. Surg. Oncol. 61, 68–83 (1996).
Tamakoshi, A. et al. Cohort profile of the Japan Collaborative Cohort Study at final follow-up. J. Epidemiol. Jpn. Epidemiol. Assoc. 23, 227–232 (2013).
Tamakoshi, A. Informed consent in epidemiologic research before the implementation of ethical guidelines. J. Epidemiol. Jpn. Epidemiol. Assoc. 14, 177–181 (2004).
Japanese Ministry of Education, Culture, Sports, Science and Technology & Ministry of Health, Labor and Welfare. Ethical Guidelines for Medical and Health Research Involving Human Subjects (2016).
Nakayama, T., Sakai, M. & Slingsby, B. T. Japan’s ethical guidelines for epidemiologic research: a history of their development. J. Epidemiol. Jpn. Epidemiol. Assoc. 15, 107–112 (2005).
Mori, M. et al. Survey for incidence of cancer as a measure of outcome in the JACC study. J. Epidemiol. Jpn. Epidemiol. Assoc. 15 Suppl 1, S80–85 (2005).
Viale, G. The current state of breast cancer classification. Ann. Oncol. 23, x207–x210 (2012).
Mroczek, D. K. & Spiro, A. Modeling intraindividual change in personality traits: findings from the normative aging study. J. Gerontol. B. Psychol. Sci. Soc. Sci. 58, P153–165 (2003).
Roberts, B. W., Walton, K. E. & Viechtbauer, W. Patterns of mean-level change in personality traits across the life course: a meta-analysis of longitudinal studies. Psychol. Bull. 132, 1–25 (2006).
Sliwinski, M. J., Almeida, D. M., Smyth, J. & Stawski, R. S. Intraindividual change and variability in daily stress processes: findings from two measurement-burst diary studies. Psychol. Aging 24, 828–840 (2009).
Weedon-Fekjær, H., Lindqvist, B. H., Vatten, L. J., Aalen, O. O. & Tretli, S. Breast cancer tumor growth estimated through mammography screening data. Breast Cancer Res. BCR 10, R41 (2008).
Sone, T. et al. Sense of life worth living (ikigai) and mortality in Japan: Ohsaki Study. Psychosom. Med. 70, 709–715 (2008).
Koizumi, M., Ito, H., Kaneko, Y. & Motohashi, Y. Effect of having a sense of purpose in life on the risk of death from cardiovascular diseases. J. Epidemiol. Jpn. Epidemiol. Assoc. 18, 191–196 (2008).
Tomioka, K., Kurumatani, N. & Hosoi, H. Relationship of Having Hobbies and a Purpose in Life With Mortality, Activities of Daily Living and Instrumental Activities of Daily Living Among Community-Dwelling Elderly Adults. J. Epidemiol. Jpn. Epidemiol. Assoc. 26, 361–370 (2016).
Nestor, P. G. & Schutt, R. K. Research Methods in Psychology: Investigating Human Behavior (SAGE Publications, 2014).
Acknowledgements
This work was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Science, Sports and Culture of Japan; Grants-in-Aid for Scientific Research on Priority Areas of Cancer; and Grants-in-Aid for Scientific Research on Priority Areas of Cancer Epidemiology from the Japanese Ministry of Education, Culture, Sports, Science and Technology (Nos 61010076, 62010074, 63010074, 1010068, 2151065, 3151064, 4151063, 5151069, 6279102, 11181101, 17015022, 18014011, 20014026 and 20390156). N.K is a board member of Clinical Study Support, Inc. (Nagaya, Japan). T.S is an employee of the Clinical Study Support, Inc. Clinical Study Support, Inc. had no role regarding this study. We express our appreciation to Drs. Kunio Aoki and Yoshiyuki Ohno, Professors Emeritus of the Nagoya University School of Medicine and former chairpersons of the JACC Study. We are also greatly indebted to Dr. Haruo Sugano, former Director of the Cancer Institute, Tokyo, who greatly contributed to the initiation of the JACC Study; Dr. Tomoyuki Kitagawa, Director Emeritus of the Cancer Institute of the Japanese Foundation for Cancer Research and former chairman of the Grant-in-Aid for Scientific Research on the Priority Area’Cancer’; and Dr. Kazao Tajima of the Aichi Cancer Center, who was the previous chairman of the Grant-in Aid for Scientific Research on Priority Areas of Cancer Epidemiology, for their warm encouragement and support of this study. The present members of the JACC Study Group are as follows: Dr. Akiko Tamakoshi (present chairperson of the study group), Hokkaido University Graduate School of Medicine; Drs. Mitsuru Mori and Fumio Sakauchi, Sapporo Medical University School of Medicine; Dr. Yutaka Motohashi, Akita University School of Medicine; Dr. Ichiro Tsuji, Tohoku University Graduate School of Medicine; Dr. Yosikazu Nakamura, Jichi Medical School; Dr. Hiroyasu Iso, Osaka University School of Medicine; Dr. Haruo Mikami, Chiba Cancer Center; Dr. Michiko Kurosawa, Juntendo University School of Medicine; Dr. Yoshiharu Hoshiyama, Yokohama Soei University; Dr. Naohito Tanabe, University of Niigata Prefecture; Dr. Koji Tamakoshi, Nagoya University Graduate School of Health Science; Dr. Kenji Wakai, Nagoya University Graduate School of Medicine; Dr. Shinkan Tokudome, National Institute of Health and Nutrition; Dr. Koji Suzuki, Fujita Health University School of Health Sciences; Dr. Shuji Hashimoto, Fujita Health University School of Medicine; Dr. Shogo Kikuchi, Aichi Medical University School of Medicine; Dr. Yasuhiko Wada, Faculty of Nutrition, University of Kochi; Dr. Takashi Kawamura, Kyoto University Center for Student Health; Dr. Yoshiyuki Watanabe, Kyoto Prefectural University of Medicine Graduate School of Medical Science; Dr. Kotaro Ozasa, Radiation Effects Research Foundation; Dr. Tsuneharu Miki, Kyoto Prefectural University of Medicine Graduate School of Medical Science; Dr. Chigusa Date, School of Human Science and Environment, University of Hyogo; Dr. Kiyomi Sakata, Iwate Medical University; Dr. Yoichi Kurozawa,Tottori University Faculty of Medicine; Drs. Takesumi Yoshimura and Yoshihisa Fujino, University of Occupational and Environmental Health; Dr. Akira Shibata, Kurume University; Dr. Naoyuki Okamoto, Kanagawa Cancer Center; and Dr. Hideo Shio, Moriyama Municipal Hospital.
Author information
Authors and Affiliations
Contributions
A.T. and S.K. designed the study. T.S. had the original idea for this study and conduced the analysis. T.S. and T.N. wrote the draft of the manuscript. Y.L., M.K., A.T. and S.K. supervised the study. M.M. and K.T. critically revised the article. All authors reviewed the manuscript and approved the final version.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Sawada, T., Nishiyama, T., Kikuchi, N. et al. The influence of personality and perceived stress on the development of breast cancer: 20-year follow-up of 29,098 Japanese women. Sci Rep 6, 32559 (2016). https://doi.org/10.1038/srep32559
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep32559
This article is cited by
-
ROK study-C (Rainbow of KIBOU study-colorectum): a colorectal cancer survivor cohort study on food, nutrition, physical activity, psychosocial factors and its influences on colorectal cancer recurrence, survival and quality of life in Japan
BMC Cancer (2018)
-
Cancer screening in Koreans: a focus group approach
BMC Public Health (2018)
-
Perceived stress level and risk of cancer incidence in a Japanese population: the Japan Public Health Center (JPHC)-based Prospective Study
Scientific Reports (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
