
Abstract
Few studies have investigated the chronic obstructive pulmonary disease (COPD) mortality fraction attributable to air pollution and modification by individual characteristics of air pollution effects. We applied distributed lag non-linear models to assess the associations between air pollution and COPD mortality in 2007–2011 in Guangzhou, China and the total COPD mortality fraction attributable to air pollution was calculated as well. We found that an increase of 10 μg/m3 in particulate matter with an aerodynamic diameter of 10 μm or less (PM10), sulfur dioxide (SO2) and nitrogen dioxide (NO2) was associated with a 1.58% (95% confidence interval (CI): 0.12–3.06%), 3.45% (95% CI: 1.30–5.66%) and 2.35% (95% CI: 0.42–4.32%) increase of COPD mortality over a lag of 0–15 days, respectively. Greater air pollution effects were observed in the elderly, males and residents with low educational attainment. The results showed 10.91% (95% CI: 1.02–9.58%), 12.71% (95% CI: 5.03–19.85%) and 13.38% (95% CI: 2.67–22.84%) COPD mortality was attributable to current PM10, SO2 and NO2 exposure, respectively. In conclusion, the associations between air pollution and COPD mortality differed by individual characteristics. There were remarkable COPD mortality burdens attributable to air pollution in Guangzhou.
Similar content being viewed by others


Introduction
Worldwide, chronic obstructive pulmonary disease (COPD) affects 329 million people1. COPD has become the third-leading cause of death2, resulting in 2.9 million deaths globally in 20133. The number is expected to rise due to an increasing number of smokers and an aging population in many countries4.
An Official Public Policy Statement by the American Thoracic Society indicates that the exposure to ambient air pollution, in public health terms, likely contributes tremendously to the growing global burden of COPD5. Regarding the relationships between air pollution and COPD mortality, Zanobetti et al.6 found that particles were correlated with mortality of COPD patients in 34 US cities in 1985–1999, with a hazard ratio of 1.22 (95% confidence interval (CI): 1.17–1.27) for an increase of 10 μg/m3 in particulate matter with an aerodynamic diameter of 10 μm or less (PM10). A longitudinal study7 investigated the associations of long-term exposure to elevated traffic-related air pollution with the risk of COPD mortality in metropolitan Vancouver, Canada and exposure-response trends for these associations were observed. A few time-series studies8,9,10,11,12 analyzed the short-term effects of air pollution on COPD mortality, which commonly assessed the effects within a week; however, our prior study13 indicated that the associations between the Air Pollution Index (API) and mortality lasted for 15 days. Accordingly, examining the relationships between specific air pollutants and COPD mortality within several days may not reveal the complete picture of the associations. Broader time windows are required to explore the time courses of the associations. Few studies assessed the potential modification of individual characteristics on the short-term effects of air pollution on COPD mortality. Further investigations are needed to strengthen our understanding of ambient air pollution-associated COPD mortality.
Regarding the associations between air pollution and COPD mortality, most previous studies used ratio measures, such as relative risk (RR) and odds ratio (OR), in the analysis. Compared with these indices, the attributable deaths (AD) and attributable fraction (AF) provide more information on the excess burden due to air pollution exposure, which are more suitable for estimating potential benefits from interventions aimed at reducing air pollution. AF, compared with RR and OR, has more public health consideration because it directly provides the proportion of people who may die due to air pollution exposure among all deaths. Norman et al.14 calculated the COPD deaths attributable to urban particulate matters in South Africa in 2000. Compared to AD, AF was not associated with population size or the total number of deaths and therefore can be used to compare the results from different regions. The estimate of AF due to the exposure to ambient air pollutants, including gaseous pollutants, can provide more comprehensive information on the COPD mortality burden of air pollution.
More than 90% of global COPD deaths occur in low- and middle-income countries15. In China, rapid demographic changes in the past few decades, such as an increasing number of Chinese living in the COPD age range, make COPD an inevitable public health challenge in the foreseeable future. Guangzhou is the largest city in southern China where the burden of COPD is heavy, with 8 persons dying due to COPD per day in 2007–20088. Meng et al.8 provided the RR estimates for the association between air pollution and mortality using two-year data (2007–2008). The present study further assessed the burden of COPD mortality due to exposure to ambient air pollution using AF and examined the potential effect modification of air pollution by individual characteristics in Guangzhou, China, in 2007–2011.
Results
There were 10,095 COPD deaths in 2007–2011 in Guangzhou, accounting for 8.4% of all registered deaths. 5.2% of them were <65 years of age. 60.1% were males and 73.2% were residents with low educational attainment (Table 1).
Over the 1,826 days of the study, an average of 6 COPD deaths (range: 0 to 22) occurred per day and the mean daily concentration of PM10, SO2 and NO2 was 72.6 μg/m3, 40.0 μg/m3 and 60.7 μg/m3, respectively (Table 2). Of the total days, 4.76%, 8.05% and 1.10% of days did not achieve the air quality target of the Chinese Ministry of Environmental Protection 2012 (150 μg/m3, 80 μg/m3 and 150 μg/m3, respectively) and 67.9% and 73.9% of days did not achieve the target of WHO Air Quality Guidelines for PM10 and SO2 (50 μg/m3 and 20 μg/m3, respectively).
The distributed lag surface reveals that COPD mortality risk was positively associated with air pollutant concentrations, with the strongest single-day association on the current day for all three air pollutants (Fig. 1). The harvesting effects were observed for PM10 and NO2 on lag 2–7 days (Fig. 2). An increase of 10 μg/m3 in the concentration of PM10, SO2 and NO2 was associated with a cumulative 1.58% (95% CI: 0.12–3.06%), 3.45% (95% CI: 1.30–5.66%) and 2.35% (95% CI: 0.42–4.32%) increase, respectively, in COPD mortality across lag 0–15 days (Table 3). The effect estimates for the current day’s air pollutant concentrations are provided in the Supplementary Table 2.

3-D plot of percentage change in COPD mortality associated with 10 μg/m3 increases in air pollutants along ambient air pollutant concentrations and lag days.

The percentage change in COPD mortality associated with 10 μg/m3 increases in ambient air pollutant concentrations along lag 0–15 days.
Greater PM10, SO2 and NO2 effects were observed for the elderly and males. Additionally, residents with low educational attainment were more susceptible to the air pollution effects (Table 3).
Based on the estimates of RR, we calculated that 10.91% (95% CI: 1.02–19.58%), 12.71% (95% CI: 5.03–19.85%) and 13.38% (95% CI: 2.67–22.84%) COPD mortality were attributable to current PM10, SO2 and NO2 exposures, respectively. If the concentrations of PM10, SO2 and NO2 attained the levels of Chinese national ambient air quality standards (NAAQS), a reduction of 0.23% (95% CI: 0.02–0.44%), 0.66% (95% CI: 0.25–1.07%) and 0.05% (95% CI: 0.01–0.08%) in COPD mortality would be achieved, respectively. If the air pollution decreased to half of the NAAQS levels, the reduction in COPD mortality for PM10, SO2 and NO2 were approximately 10, 5 and 30 times as much as that for the attainment of NAAQS. The corresponding reductions were 4.31% (95% CI: 0.38–7.94%) and 7.15% (95% CI: 2.82–11.24%) if the concentrations of PM10 and SO2 attained the WHO targets, respectively (Table 4). Because there is no guideline for 24-hour concentrations of NO2 recommended by the WHO, the estimate for NO2 could not be calculated herein.
Results were robust when we used different models to assess the effects of air pollutants (see Supplementary Table S3).
Discussion
As a time-series study, this study examined the associations between daily variation in air pollution levels and daily changes in COPD mortality. Those traditional risk factors (e.g., smoking) that were time-independent or did not change on a daily basis were controlled for by design. Our study confirmed that ambient air pollution was associated with COPD mortality in Guangzhou, China. Stronger air pollution effects were observed in the elderly and males. Additionally, residents with low educational attainment were more sensitive to the air pollution effects. The COPD mortality burden attributable to SO2 was particularly high (Table 3, Table 4).
Some studies8,9,10,11,12 examined the associations between air pollution and COPD in different cities. Supplementary Table S4 shows the results of these studies, which indicated that the associations differed by study location. There are several possible reasons for the observed geographical differences. First, different geographical and meteorological patterns of these locations influence the transport and diffusion of air pollutants and chemical reactions between pollutants. Thus, the components of the pollution mixture the residents were exposed to varied by study location. Next, the ability to pay for a suitable medical treatment for COPD may be an alternative explanation for the disparity in the effects of air pollution. COPD patients who could not receive appropriate treatment because of poverty and low health care utilization may be more vulnerable to air pollution effects. Moreover, different parameters used to control for the effects of temperature may also influence the effect estimates of air pollutants. The present study controlled for the potential effects of the current day and previous 14 days’ temperatures because some studies have confirmed that temperature effects were much larger than those of air pollution and lasted for almost two weeks16. However, previous studies commonly controlled for the confounding effects of temperature within shorter days, which may overestimate the air pollution effects. Finally, the lag selected for the effects of air pollutants may explain the different effect estimates.
Examining the effect modification of individual characteristics will help identify vulnerable subgroups that are targeted subpopulations for the setting of air quality standards and development of intervention programs. Our study further confirmed that old people were more vulnerable to exposure to air pollutants. Old people, especially those with COPD, should reduce physical exertion, particularly outdoors when the level of air pollutant exceeds the air quality standard.
Although some studies reported stronger air pollution effects among women than among men17, the present study showed that males with COPD were more sensitive to air pollution effects. A 20-year prospective California Adventists Health Study18 showed similar gender differences in which generally significantly reduced lung function related to air pollution (PM10, SO4 and ozone) was observed in males, particularly males with parental respiratory illness, but not in females. Possible explanations for gender differences in air pollution effects include confounding or modification effects by smoking behaviors, job-related chemical exposures and distinct exposure and responses to psychosocial stressors17.
We found that COPD patients with low educational attainment were more susceptible to air pollution exposure. This finding is plausible. First, most COPD patients with low educational attainment suffer from financial crisis; thus, they often live in places of low quality that offer little protection from indoor infiltration of air pollution. Additionally, the antioxidant properties of certain nutrients, such as vitamin C, beta carotene, selenium and copper, may modulate an individual’s susceptibility to oxidative damage and it was suggested that a diet rich in omega-3 fatty acids may inhibit arachidonic acid production, thereby protecting against bronchial constriction19. Additionally, a diet rich in fruit and vegetables was found to reduce the risk of COPD20. However, COPD patients with low educational attainment commonly have limited access to fresh and nutritious food, resulting in reduced intake of antioxidant polyunsaturated fatty acids and vitamins that may protect against adverse consequences of COPD and particle exposure21. Moreover, owing to a lack of relevant education, they may pay less attention to the sanitary conditions of their houses, which exposes them to various risk factors, such as viruses and bacteria. Because increased exposure to viral infections may increase their susceptibility, they tend to have a higher prevalence of diseases that predispose to or can be exacerbated by air pollution. Finally, COPD is a burdensome disease, so COPD patients with low educational attainment commonly receive inferior medical treatment, which means that if they are severely ill, they are more likely to die.
Some biological plausibility has been proposed for the associations between air pollution and COPD mortality. COPD patients commonly have a systemic deficit in their antioxidant defences22. The exposure to air pollutants may produce additive oxidative stress as a response to the inflammation of the lungs. Specifically, the exposure to NO2 might increase the release of inflammatory mediators from bronchial epithelial cells23 and enhance the recruitment of macrophages and T lymphocytes to the airway24. In addition, Dadvand et al.25. showed positive associations between short-term exposures to NO2 and C-reactive protein and fibrinogen, with a suggestive association with other inflammatory biomarkers. SO2 may produce an immediate irritant effect on the respiratory mucosa because of its high water-solubility in the upper respiratory tract26. Moreover, in a rat model, urban air particles induced the expression of genes involved in airway wall fibrosis27. Further, air pollution exposure may negatively affect the development of lung function early in life5. Additional research is needed to confirm the causal effects of ambient air pollution.
Driscoll et al.28 assessed the global burden of COPD mortality due to occupational airborne exposures in the year 2000. They found that the AF varied from 9% in some areas of the US with high child and adult mortality to 16% in areas of Europe with low child mortality but high adult mortality and areas of the Western Pacific with very low mortality for both children and adults. Norman et al.29 showed that 23.2% of COPD mortality in South African children and adults in 2000 was attributable to household use of solid fuels. Norman et al.14 found that in 2000 there were 466 COPD deaths attributable to urban ambient air pollution (PM10 and PM2.5) in South Africa. The present study revealed that 10.91%, 12.71% and 13.38% of COPD mortality was attributable to ambient PM10, SO2 and NO2 in Guangzhou, respectively. Notably, we found that more benefits could be achieved from the continuous reduction of air pollution, even if air quality attained Chinese national standards or WHO targets, suggesting that the current standards may not adequately protect people.
Compared to PM10 and NO2, SO2 posed a heavier burden of COPD mortality because of its higher RR and more days with a high SO2 level. Although the municipal government introduced regulation to control SO2 emissions in 2005, the consumption of coal in Guangzhou is still high, accounting for approximately 70% of total energy consumption. Given the high public health burden of SO2 pollution, the government should continue taking some effective measures to control it.
The present study has some limitations. First, we presented only the associations between COPD mortality and three criteria pollutants. Ozone and PM2.5 linked to COPD were not considered in this study because the data were not available during the study period. Next, the average air pollutant concentrations collected from seven monitoring stations were used as the average exposure level of air pollution, resulting in measurement error, which may underestimate the air pollution effects. Finally, we considered only the situation in central Guangzhou; no information was provided for rural areas.
In conclusion, ambient air pollution has a significant impact on COPD mortality. Among COPD patients, old people, males and residents with low educational attainment were vulnerable groups in relation to air pollution effects. More attention should be paid to these subpopulations. Our findings indicated that COPD mortality in Guangzhou may decrease by 4.31% and 7.15% if the level of PM10 and SO2 is reduced to the target values of WHO guidelines, respectively. Public efforts to prevent COPD should include the reduction of ambient air pollution.
Methods
Data
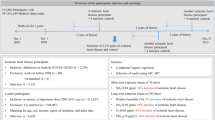
Guangzhou is the largest southern city in China. According to the sixth national population census in 2010, there were over 12.7 million permanent residents in Guangzhou, among which 60.8% lived at six urban central districts. We obtained individual data for all registered deaths due to an underlying cause of COPD (the International Classification of Diseases, the tenth version [ICD-10]: J40-J44 and J47) at six urban central districts in Guangzhou between January 1, 2007 and December 31, 2011, from Guangzhou Centre for Disease Control and Prevention. Age group (<65 years and ≥65 years), gender and educational attainment (low educational attainment was defined as illiterate or primary school, high educational attainment as middle school or above) were analyzed as potential effect modifiers for air pollution effects.
The Guangzhou Bureau of Environmental Protection provided daily data for three criteria ambient air pollutants—PM10, sulfur dioxide (SO2) and nitrogen dioxide (NO2)—from seven fixed-site air monitoring stations, with various types of sites located in five different central districts. Detailed descriptions of monitoring stations were described in our previous studies30,31. The average daily air pollutant concentrations in the entire territory of Guangzhou were computed using the centering method32. Daily meteorological data on mean temperature, relative humidity and atmospheric pressure were obtained from the China Meteorological Data Sharing Service System.
Statistical methods
We used quasi-Poisson regression models combined with distributed lag non-linear models (DLNMs) to analyze the associations between air pollution and COPD mortality. The model is expressed as follows:

where t is the calendar day of observation; Yt is the observed daily death counts on day t, following the quasi-Poisson distribution allowing for over-dispersion. The daily number of COPD deaths was 6, on average. Because only 28 days (1.26%) had a zero count, the zero-inflated Poisson regression was not required. In the present study, we tried different ways to control for the long-term trend, seasonality and effect of temperature. The partial autocorrelation function (PACF), Akaike information criterion (AIC) and generalized cross validation (GCV) were used to select the best model. Details are shown in the Supplementary Material. The PACF for each model was provided in Supplementary Figs S1–S3 and the sum of absolute PACF over 30 days, AIC and GCV for each model is shown in Supplementary Table S1. In the final model, we used dummy variables indicating the year (YEARt) to control for the long-term trend of COPD mortality. Trigonometric functions were used to control for the seasonality of COPD mortality and the seasonality was assumed to vary by year. γ1 and γ2 are coefficients for  and
and  , respectively. γ3 is the vector of coefficients for
, respectively. γ3 is the vector of coefficients for  . ns(.) is a natural cubic spline. TEMPt014 represents the 15-day moving average temperature on day t. DOWt are dummy variables indicating the day of the week on day t and η is the vector of coefficients. Holidayt is an indicator variable that is “1” if day t was a holiday and υ is the coefficient. A 3 df ns was used to smooth the mean relative humidity (RHt) and atmospheric pressure (PREt). APt,l are matrices obtained by applying the DLNM to air pollutant concentrations. We used a linear function for air pollutant concentrations with the maximum lag of 15 days13. The df for lag was specified to be 413. β is the vector of coefficients for APt,l and l is lag days for air pollutant concentrations.
. ns(.) is a natural cubic spline. TEMPt014 represents the 15-day moving average temperature on day t. DOWt are dummy variables indicating the day of the week on day t and η is the vector of coefficients. Holidayt is an indicator variable that is “1” if day t was a holiday and υ is the coefficient. A 3 df ns was used to smooth the mean relative humidity (RHt) and atmospheric pressure (PREt). APt,l are matrices obtained by applying the DLNM to air pollutant concentrations. We used a linear function for air pollutant concentrations with the maximum lag of 15 days13. The df for lag was specified to be 413. β is the vector of coefficients for APt,l and l is lag days for air pollutant concentrations.
We plotted 3-D graphics to show the COPD mortality risk along the air pollutant concentrations and lag days. The associations were presented as the percentage change in COPD mortality associated with a 10 μg/m3 increase in air pollutant concentrations. Further, we performed subgroup analyses by age group, gender and educational attainment.
To estimate the COPD mortality risk attributable to air pollution, the levels set by the Chinese national ambient air quality standards (NAAQS)33 and WHO air quality guidelines34 were considered as the references, respectively; that is, the percentage reduction in COPD mortality if the air quality level attained NAAQS or WHO targets. In addition, we also calculated the AFs using 50%, 20% and 0% of the levels set by NAAQS as references. The overall cumulative RR corresponding to each day’s air pollutant concentration was used to compute the AF and AD35:


where the AFx,t and ADx,t are attributable fraction and attributable deaths at day t, respectively; βx represents the risk associated with the exposure to air pollutants at level x (i.e.,  ; Ref is the air quality guideline;
; Ref is the air quality guideline;  is the coefficient for DLNM of air pollutant concentration). L is the maximum lag for the air pollution effects (i.e., 15). nt is the observed number of COPD deaths at day t.
is the coefficient for DLNM of air pollutant concentration). L is the maximum lag for the air pollution effects (i.e., 15). nt is the observed number of COPD deaths at day t.
The total AD due to air pollution was given by the sum of the contributions from all the days of the series under study and its ratio with the total number of observed deaths provided the total AF. Their empirical confidence intervals were obtained by Monte Carlo simulations assuming a multivariate normal distribution of the best linear unbiased predictions of coefficients.
Results of better models judged by the three criteria mentioned above are shown as sensitivity analyses. All analyses were performed using R software (version 3.2.0; R Foundation for Statistical Computing, Vienna, Austria).
Additional Information
How to cite this article: Li, L. et al. The burden of COPD mortality due to ambient air pollution in Guangzhou, China. Sci. Rep. 6, 25900; doi: 10.1038/srep25900 (2016).
References
Vos, T. et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2163–96 (2012).
Burney, P. G., Patel, J., Newson, R., Minelli, C. & Naghavi, M. Global and regional trends in COPD mortality, 1990–2010. Eur Respir J 45, 1239–47 (2015).
Global, regional and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385, 117–71 (2015).
Mathers, C. D. & Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 3, e442 (2006).
Eisner, M. D. et al. An official American Thoracic Society public policy statement: Novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 182, 693–718 (2010).
Zanobetti, A., Bind, M. A. & Schwartz, J. Particulate air pollution and survival in a COPD cohort. Environ Health 7, 48 (2008).
Gan, W. Q., FitzGerald, J. M., Carlsten, C., Sadatsafavi, M. & Brauer, M. Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am J Respir Crit Care Med 187, 721–7 (2013).
Meng, X., Wang, C., Cao, D., Wong, C. & Kan, H. Short-term effect of ambient air pollution on COPD mortality in four Chinese cities. Atmos Environ 77, 149–154 (2013).
Romieu, I. et al. Multicity study of air pollution and mortality in Latin America (the ESCALA study). Res Rep Health Eff Inst, 5–86 (2012).
Zeka, A., Zanobetti, A. & Schwartz, J. Short term effects of particulate matter on cause specific mortality: effects of lags and modification by city characteristics. Occup Environ Med 62, 718–25 (2005).
Fischer, P., Hoek, G., Brunekreef, B., Verhoeff, A. & van Wijnen, J. Air pollution and mortality in The Netherlands: are the elderly more at risk? Eur Respir J Suppl 40, 34s–38s (2003).
Wong, T. W., Tam, W. S., Yu, T. S. & Wong, A. H. Associations between daily mortalities from respiratory and cardiovascular diseases and air pollution in Hong Kong, China. Occup Environ Med 59, 30–5 (2002).
Li, L. et al. Can the Air Pollution Index be used to communicate the health risks of air pollution? Environ Pollut 205, 153–160 (2015).
Norman, R., Cairncross, E., Witi, J. & Bradshaw, D. Estimating the burden of disease attributable to urban outdoor air pollution in South Africa in 2000. S Afr Med J 97, 782–90 (2007).
World Health Organization, Chronic obstructive pulmonary disease (COPD). (2015) Available at: http://www.who.int/mediacentre/factsheets/fs315/en/. (Accessed: 29th January 2016).
Yang, J., Ou, C. Q., Ding, Y., Zhou, Y. X. & Chen, P. Y. Daily temperature and mortality: a study of distributed lag non-linear effect and effect modification in Guangzhou. Environ Health 11, 63 (2012).
Clougherty, J. E. A growing role for gender analysis in air pollution epidemiology. Environ Health Perspect 118, 167–76 (2010).
Abbey, D. E. et al. Long-term particulate and other air pollutants and lung function in nonsmokers. Am J Respir Crit Care Med 158, 289–98 (1998).
Finkelstein, M. M. et al. Relation between income, air pollution and mortality: a cohort study. CMAJ 169, 397–402 (2003).
Watson, L. et al. The association between diet and chronic obstructive pulmonary disease in subjects selected from general practice. Eur Respir J 20, 313–8 (2002).
Romieu, I. et al. Omega-3 fatty acid prevents heart rate variability reductions associated with particulate matter. Am J Respir Crit Care Med 172, 1534–40 (2005).
Mannino, D. M. & Buist, A. S. Global burden of COPD: risk factors, prevalence and future trends. Lancet 370, 765–73 (2007).
Bayram, H., Sapsford, R. J., Abdelaziz, M. M. & Khair, O. A. Effect of ozone and nitrogen dioxide on the release of proinflammatory mediators from bronchial epithelial cells of nonatopic nonasthmatic subjects and atopic asthmatic patients in vitro. J Allergy Clin Immunol 107, 287–94 (2001).
Blomberg, A. et al. The inflammatory effects of 2 ppm NO2 on the airways of healthy subjects. Am J Respir Crit Care Med 156, 418–24 (1997).
Dadvand, P. et al. Air pollution and biomarkers of systemic inflammation and tissue repair in COPD patients. Eur Respir J 44, 603–13 (2014).
Ko, F. W. et al. Temporal relationship between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Hong Kong. Thorax 62, 780–5 (2007).
Dai, J., Xie, C., Vincent, R. & Churg, A. Air pollution particles produce airway wall remodeling in rat tracheal explants. Am J Respir Cell Mol Biol 29, 352–8 (2003).
Driscoll, T. et al. The global burden of non-malignant respiratory disease due to occupational airborne exposures. Am J Ind Med 48, 432–45 (2005).
Norman, R., Barnes, B., Mathee, A. & Bradshaw, D. Estimating the burden of disease attributable to indoor air pollution from household use of solid fuels in South Africa in 2000. S Afr Med J 97, 764–71 (2007).
Li, L. et al. Spatial and temporal analysis of Air Pollution Index and its timescale-dependent relationship with meteorological factors in Guangzhou, China, 2001–2011. Environ Pollut 190, 75–81 (2014).
Ou, C. Q. et al. Excess winter mortality and cold temperatures in a subtropical city, Guangzhou, China. PLoS One 8, e77150 (2013).
Wong, C. M., Ma, S., Hedley, A. J. & Lam, T. H. Effect of air pollution on daily mortality in Hong Kong. Environ Health Perspect 109, 335–40 (2001).
Olivares, E. & Wagner, V. (2014) Available at: http://transportpolicy.net/index.php?title=China:_Air_Quality_Standards (Accessed: 29th January 2016).
World Health Organization, Ambient (outdoor) air quality and health. (2014) Available at: http://www.who.int/mediacentre/factsheets/fs313/en/ (Accessed: 29th January 2016).
Gasparrini, A. & Leone, M. Attributable risk from distributed lag models. BMC Med Res Methodol 14, 55 (2014).
Acknowledgements
We thank the Guangzhou Centre for Disease Control and Prevention and the China Meteorological Data Sharing Service System for providing mortality and meteorological data, respectively. This research was funded by the National Nature Science Foundation of China (81573249) and the Technology Planning Project of Guangdong Province, China (2013B021800041). J.Y. was supported by National Basic Research Program of China (973 Program)(Grant No.2012CB955504).
Author information
Authors and Affiliations
Contributions
C.Q., L.L., Y.F. and P.Y. initiated the study and collected the data. L.L. and J.Y. performed statistical analyses. L.L. and C.Q. drafted the manuscript. All authors read and approved the final manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Li, L., Yang, J., Song, YF. et al. The burden of COPD mortality due to ambient air pollution in Guangzhou, China. Sci Rep 6, 25900 (2016). https://doi.org/10.1038/srep25900
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep25900
This article is cited by
-
Spatio-Temporal Variability and Health Risk Assessment of Benzo[a]pyrene in Different Population Through Ambient Air Exposure in Delhi, India
Exposure and Health (2022)
-
The effect of consecutive ambient air pollution on the hospital admission from chronic obstructive pulmonary disease in the Chengdu region, China
Air Quality, Atmosphere & Health (2021)
-
Can Global Policy Impact Local Environmental Justice? Using CASPER to Assess Perceived Health Effects of an Incinerator
Human Ecology (2020)
-
Diabetes mortality burden attributable to short-term effect of PM10 in China
Environmental Science and Pollution Research (2020)
-
Short-term exposure to ambient air pollution and acute myocardial infarction attack risk
Journal of Public Health (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
