
Abstract
Hemophilia B (HB) is an X-linked recessive bleeding disorder caused by mutations in the coagulation factor IX (FIX) gene. Genotyping patients with HB is essential for genetic counseling and provides useful information for patient management. In this study, the F9 gene from 23 patients with HB was analyzed by direct sequencing. Nineteen point mutations were identified, including a novel missense variant (c.520G > C, p.Val174Leu) in a patient with severe HB and a previously unreported homozygous missense mutation (c.571C > T, p.Arg191Cys) in a female patient with mild HB. Two large F9 gene deletions with defined breakpoints (g.10413_11363del, g.12163_23369del) were identified in two patients with severe HB using a primer walking strategy followed by sequencing. The flanking regions of the two breakpoints revealed recombination-associated elements (repetitive elements, non-B conformation forming motifs) with a 5-bp microhomology in the breakpoint junction of g.12163_23369del. These findings imply that non-homologous end joining and microhomology-mediated break-induced replication are the putative mechanisms for the deletions of the F9 gene. Because the g.12163_23369del deletion caused exons to be absent without a frameshift mutation occurring, a smaller FIX protein was observed in western blot analyses.
Similar content being viewed by others

Introduction
The human coagulation factor IX (FIX) gene, mapped at chromosome Xq27.1-q27.2, is approximately 32.7 kilobases (kb) in length. This gene contains eight exons encoding a 2.8 kb mRNA, 1.4 kb of which is translated to synthesize the vitamin K-dependent human FIX protein1,2. Heterogeneous mutations in the F9 gene lead to deficiency or dysfunction of Factor IX and result in an X-linked inherited bleeding disorder known as hemophilia B (HB), which primarily affects approximately 1 in 25,000 male live births3 and very rarely affects females. Based on the activity level of FIX, HB is classified as severe (<1% of normal), moderate (1–5% of normal), or mild (5–40% of normal)4. The mutations associated with mild, moderate and severe phenotypes are distributed evenly throughout the F9 gene5. Currently, more than 1000 unique variants in the F9 gene have been identified worldwide, among which 73% are point mutations, 16.3% are deletions and the remainder are insertions, duplications, or combinations of insertions and deletions (indels)6.
Large deletions (>50 bp) in the F9 gene, 90% of which are associated with the severe phenotype, occur in approximately 5% of patients with severe HB and significantly increased risks for developing inhibitors5,7,8. Although approximately 100 types of large deletions of the F9 gene have been reported, only 19 have defined breakpoints9,10,11. It has been proposed that the underlying mechanisms may be non-allelic homologous recombination (NAHR), non-homologous end joining (NHEJ) or microhomology-mediated break-induced recombination (MMBIR) events10. In this paper, we identified a homozygous point mutation in a female patient with mild HB. We also discovered a novel point variant and characterized the breakpoints of two suspected large deletions of the F9 gene from a cohort of 23 patients with HB, which enabled us to explore the underlying mechanisms involved in these deletions and their roles in HB.
Materials and Methods
Subjects
This study was approved by the Ethics Committee of Union Hospital at Huazhong University of Science and Technology and the methods were applied in accordance with the approved guidelines. Written informed consent was obtained from all of the participants and their respective family members. A cohort of 23 unrelated patients with HB (22 males and a 3-year-old female) were enrolled in this study. Family members of one patient (CD) were also included to confirm the carrier state of his mother (CDM) and to determine the carrier status of his sister (CDS). Peripheral blood samples obtained from the subjects were centrifuged at 1600 × g for 20 min at 4 °C. The plasma samples were aliquoted and stored in polypropylene tubes at −80 °C and genomic DNA was extracted from the cell pellet according to the protocol provided by the manufacturer (Bioteke, Beijing, China) and as previously described11. The activity of FIX and other coagulation factors was assayed using a STA-R automated coagulation analyzer (Diagnostica Stago Inc., Asnieres, France) and commercial reagents from Stago according to the manufacturers’ recommendations.
Genetic analysis and sequencing
All exons, 5’- and 3’-untranslated regions (UTRs), exon-intron junction regions and the promoter of F9 were amplified by polymerase chain reaction (PCR). We used the primers and PCR conditions as previously reported by Hinks et al.12 The PCR products were analyzed by direct DNA sequencing using an ABI PRISM 3730XL DNA sequencer (Applied Biosystems, Carlsbad, CA, USA). Large deletions were suspected in two patients with severe HB due to partial exons repeatedly failing to be amplified from the F9 sequences. Specifically, exon 2 and exon 3 did not amplify from the F9 sequence of the first patient (LXF), whereas exon 4 and exon 5 did not amplify in the other patient (CD). The deletions were validated by long-range PCR (LR-PCR) using Long PCR Enzyme Mix (Life Technologies, Grand Island, NY, USA) according to the manufacturer’s two-step cycling protocol (Table S1).
To identify the junctions of the deletions, sequential primers were designed at the interval of approximately 0.5–1 kb to amplify the sequences (fragment by fragment and the ends of the adjacent fragments were overlapping) on both sides of the breakpoints (from exon 1 to exon 4 in patient LXF and from exon 3 to exon 6 in patient CD) to narrow down the regions containing the breakpoints. The PCR products were electrophoresed on 1% agarose gel stained with GELVIEW (Bioteke, Beijing, China) for 85 min. Two pairs of sequencing primers were designed to sequence through the breakpoint (Table S1).
The nomenclature of the F9 mutations was based on cDNA reference sequence NM_000133.3 and protein reference sequence NP_000124.1 in accordance with the recommendations of the Human Genome Variation Society (HGVS; http://www.hgvs.org/mutnomen/) guidelines.
Bioinformatics analysis
The conservation of amino acids affected by the novel missense mutations of F9 was analyzed by multiple sequence alignment (HomoloGene; http://www.ncbi.nlm.nih.gov/sites/entrez) in orthologous FIX sequences from human, chimpanzee, Rhesus monkey, dog, mouse and Norway rat. The possible pathogenicity of a newly identified missense mutation was evaluated using the following in silico bioinformatics tools: PolyPhen-2 (http://genetics.bwh.harvard.edu/pph2/), MutationTaster (http://www.mutationtaster.org/) and Sorting Intolerant From Tolerant (SIFT; http://sift.jcvi.org)13,14,15. To evaluate and score the potential splice site gain or loss in mutations, the following online software tools were applied: SplicePort (http://spliceport.cbcb.umd.edu), ASSP (http://wangcomputing.com/assp/index.html) and BDGP (www.fruitfly.org/seq_tools/splice.html). To investigate the presence of certain sequence features surrounding the breakpoint regions (300 bp down- and upstream from the breakpoint junction), a series of bioinformatics analyses were performed to determine the presence of repeat sequences, sequence motifs associated with DNA breakage and sequences leading to non-B DNA conformations that predispose carriers to genomic rearrangements, as previously described10,16.
Western blotting, ELISA and thrombin generation assays
To evaluate the influence of the large deletions on plasma factor IX protein and blood coagulation, western blotting, ELISA and a thrombin generation test were performed using plasma samples from patient LXF and patient CD and from CDM and CDS. CDS served as a control because she had no identified mutations and normal factor IX activity. Plasma samples, 15 μl, from LXF, CD, CDM and CDS were electrophoresed on 10% polyacrylamide gels with SDS and were blotted onto a polyvinylidene difluoride membrane. The primary antibody was mouse monoclonal antibody (Santa Cruz Biotechnology, Dallas, TX, USA) specific for an epitope mapping between amino acids 301 and 339 within an internal region of FIX of human origin. GAPDH served as the control. The blots were analyzed using the ECL system.
Quantification of plasma FIX levels was performed using a ZYMUTEST FIX ELISA kit (Hyphen BioMed, Andresy, France), according to the manufacturer’s protocol.
The thrombin generation in platelet poor plasma (PPP) was measured using a calibrated automated thrombogram (Thrombinoscope BV, Maastricht, the Netherlands), according to the manufacturer’s instructions. Briefly, 80-μL plasma samples were mixed with 20 μL PPP reagent (5 pM tissue factor, 4 μM phospholipids) in a 96-well plate. Coagulation was initiated by adding 100 mM calcium chloride (20 μL) in a custom BSA buffer containing 2.5 mM fluorogenic substrate (Z-Gly-Gly-Arg-AMC). As a result of splitting by thrombin, the fluorescent AMC (7-amino-4-methylcoumarin) was released and measured using a 390-nm excitation and a 460-nm emission filter set in an Ascent Fluoroscan. Fluorescence was recorded for 60 min.
Results and Discussion
FIX activity and mutation profile
DNA sequencing has been increasingly performed and applied to assess genetic disorders because the process has become less expensive and more convenient. Routine causative mutation screening by direct sequencing in patients with HB is essential for genetic counseling and prenatal diagnosis. A total of 23 patients with HB and family members of patient CD (n = 2) were genotyped by direct sequencing in the current study. Of these patients, 8 suffered from severe HB, 11 suffered from moderate HB and 3 suffered from mild HB. The severity of one patient with HB was unknown because his factor IX activity was not detected. Factor IX activity of patient CD’s family members was 47% (CDM) and 87% (CDS) of normal. Nineteen unique point mutations in the F9 gene were identified, including a novel missense variant (c.520G > C, p.Val174Leu) from a patient with severe HB and a previously unreported homozygous point mutation (c.571C > T, p.Arg191Cys) that was identified from the F9 gene sequence of a 3-year-old female patient with mild HB (Table 1, Fig. 1). In one patient with mild HB, we failed to identify any F9 gene variants. The reason may be that potential variations could exist in introns or promoter regions that our sequencing did not cover. As previously described, another likelihood is that the patient might possess somatic mosaicisms and that the DNA extracted for genotyping was derived from normal blood cells17. Large deletions were suspected in two patients with severe HB because the partial exons of the F9 gene repeatedly failed to be amplified (Table 1). Consistent with the factor IX mutation database5,6, 76.2% of the mutations identified in the current study were missense mutations and 8.7% were gross deletions (>50 bp). No inhibiting antibodies to the factor IX protein were detected in any of the patients with HB in our study.

Crystal structure of factor (F) IXa and locations of the missense mutations.
Ribbon view of the human FIXa structure to show the locations of the missense mutations. The domain orientation is taken from the porcine FIXa crystal structure (PDB ID: 1PFX). The alpha helix is colored in red, the beta strand in cyan, the band in grey and turn in green.
Novel F9 missense variants
Of the 19 point mutations in our study, one missense variant (c.520G > C, p.Val174Leu) was novel and associated with severe HB and one homozygous (c.571C > T, p.Arg191Cys) missense variant associated with mild HB was previously unreported. Both of the variants could not be found in 1000 Genomes Browser (http://www.ncbi.nlm.nih.gov/variation/tools/1000genomes/), indicating that there was an extremely small likelihood that the variants were prevalent HB-neutral single nucleotide polymorphisms. The amino acid p.Val174 affected by missense mutations is located in the linker region of Factor IX and is highly conserved in chimpanzee, Rhesus monkey, dog, mouse, Norway rat, chicken and frog. Different point mutations at the same site (c.520G > A, p.Val174Met and c.520G > T, p.Val174Leu) have been reported6. The three subjects affected by the mutations at this site had moderate to severe disease; thus indicating that mutations at this site have detrimental consequences.
Because the full-length F9 transcript has been shown to be difficult to obtain from peripheral lymphocytes18 and in silico analysis had been demonstrated to be valuable in achieving accurate predictions19, it would be informative to analyze the mutations affecting splice sites using web tools. Therefore, considering the nucleotide substitution (c.520G > C) at the 3’-end of exon 5, the impact of this variant on the splice site was analyzed using three bioinformatics tools. The score values obtained from the mutated sequences were low, suggesting that the splice donor site could be altered by the variant, resulting in abnormal alternative splicing and a frameshift in the FIX protein product. Hence, this could likely be the underlying mechanism that might explain why the patient affected by the variant c.520G > C suffered severe HB. But, as the online prediction tools are not very reliable, the exact mechanism remains to be clarified.
Although identifying the base substitution c.571C > T in the F9 gene was not novel8, the homozygous mutation of c.571C > T identified from the 3-year-old female patient with HB was previously unreported. The probability that the amino acid change (p.Arg191Cys) is deleterious was high at 1.000 based on the PolyPhen-2 and SIFT analyses, indicating that the mutation causes the Factor IX protein dysfunction and is harmful to the patient. These results might imply that the patient has severe HB. However, the activity level of FIX in her plasma sample was 19.5% of normal. The discrepancy between what was expected and what the activity level actually was may be explained by the activation process of FIX. The FIX protein is activated by either factor VIIa/tissue factor (FVIIa/TF) or Factor XIa (FXIa) through a process that requires the removal of the activation peptide20,21, which is accomplished through two proteolytic cleavages: first, an Arg191-Ala192 bond between the light chain and the activation peptide (AP) is cleaved, generating an inactive two-chain intermediate held together by a disulfide bond. Second, an Arg226-Val227 bond between the AP and catalytic domain is cleaved, thus releasing the AP and producing the final product, FIXa22. The mutation p.Arg191Cys disables the activation peptide from being cleaved from the light chain of FIX, which may influence the normal structure of the enzyme and the binding affinity of FIX with its substrate. However, because the Arg226-Val227 bond could be cleaved, the catalytic domain was not influenced. Consequently, the abnormal factor IX protein in the plasma sample of the young female patient still had some catalytic activity. Owing to the unreliability of PolyPhen-2 and SIFT and the effects of the variant was unproven without expression studies, additional research on the effect of the variant is warranted.
Characterization of the large deletions of the F9 gene
In our study, the large F9 gene deletions identified in two patients with severe HB (patient CD and LXF) were confirmed using long-range PCR; each of the fragments amplified from the hemophilic subjects’ and CDM’s (CDM, mother of the patient CD) genomic DNA samples was shorter than that of the control (Fig. 2). Considering that the factor IX activity of the asymptomatic CDM was 47% of normal, it was interesting that only a shorter fragment was amplified from her F9 sequence, which indicated that CDM could be a heterozygous carrier and that the shorter fragment could be prior to amplify. The size of the fragment amplified from CDS (sister of patient CD) was as large as predicted, suggesting that CDS was normal. The flanking regions surrounding the junctions were narrowed. Sequential primers were used to amplify the fragments on both sides of the breakpoints toward the junctions. The breakpoints were finally defined by direct sequencing using two pairs of sequencing primers. The large deletion mutations were g.10413_11363del and g.12163_23369del. The extents of the deletions of the two patients were 953 bp and 11,207 bp, respectively.

Identification of the breakpoints from two patients with severe hemophilia B.
Figure 2a,b represent patients CD and LXF, respectively. Lanes 1, 2, 3, 4 and 5 represent the DNA sequences amplified from CD, CDM, CDS, LXF and normal control, respectively. M1and M2 are DL15000 DNA Marker (Solarbio, Beijing, China) and 1 kb DNA Ladder (Solarbio, Beijing, China), respectively. The reference sequence used for the DNA sequence alignment is NCBI NC_000023.11.
The flanking sequences surrounding the junctions were analyzed using online bioinformatics tools. The repetitive elements were enriched at only one flanking side of the breakpoint junction of the two large deletion mutations. The 5’ flanking region of the breakpoint junction was mapped within a DNA/TcMar-Tigger repeat in patient LXF. The breakpoint of patient CD resided in the LINE/L1 repeat and nonrepeat sequences, respectively and was associated with a 5-bp microhomology (Table S2). In silico analysis showed that the breakpoint-flanking regions contained multiple noncanonical DNA structures and were not enriched with GC content or palindromes. Direct repeats, potentially leading to slipped hairpin structures, were found in both patients. Mirror repeats, potentially leading to triplex structures and inverted repeats, leading to a cruciform structure, were only identified in the flanking regions of patient LXF. Neither G-rich sequences for forming G-quadruplex structures nor left-handed Z-DNA forming regions were found in the breakpoint regions of the patients (Table S2).
The deletions of the chromosomal segments (copy number variants, CNVs), an underlying factor in many diseases, are not randomly distributed in the human genome but tend to be clustered in regions of the complex genomic architecture23. The potential mechanisms mediating the recombination of deletions in the F9 gene had been described by Wu et al.10 Consistent with the findings in a previous study10,16, the deletion with a 5-bp microhomology at the breakpoint junction in the F9 gene of patient CD can be explained by both NHEJ and MMBIR mechanisms. In patient LXF, there was no microhomology in the junction. The deletion might be mediated by the NHEJ mechanism. Naturally occurring repetitive DNA sequences can adopt non-B DNA structures and can often co-localize with chromosomal breakpoint “hot-spots”24,25. The genes harboring repetitive DNA sequences and non-B DNA structure-forming sequences increase the risk of genetic instability and are associated with large deletions of the F9 gene.
Western blotting, ELISA and thrombin generation test
The 5’-end and 3’-end of deletions in patient LXF were in intron 1 and exon 2 of the F9 gene, respectively, which suggested that the normal intron 1 acceptor splice site was absent from the F9 gene. The junctions were also analyzed using bioinformatics tools. The score value for patient LXF was below the software detection thresholds, indicating that there was no new splice site forming at the junction, resulting in a frameshift mutation. No splice site was affected in patient CD. The deletions of exon 4 and exon 5 predicted an in-frame shortened protein with loss of all EGF1 and EGF2 domain residues. The results from the western blots confirmed that only a normal-sized factor IX species was presented in the plasma sample of LXF as a result of prophylactic therapy. The plasma sample from CD, however, showed a normal-sized factor IX species from his prophylactic therapy and a smaller species corresponding to his hemophilic factor IX, which was predicted to be ~9 kd lower in molecular weight. The plasma sample from CDM also showed both a normal-sized factor IX species and a ~9 kd smaller species, indicating that both of the normal and truncated factor IX existed in the plasma sample of CDM (Fig. 3). Our results also suggested that the frameshift mutation in LXF might introduce a premature stop codon, leading to an abnormal polypeptide chain translated, which could degrade quickly or could not conjugate with the primary antibody used in this study. The deletions of exon 4 and exon 5 in patient CD and in CDM were also confirmed using western blots, resulting in an in-frame shortened protein without all EGF1 and EGF2 domain residues. FIXa interacts with FVIIa/TF using the EGF1 domain and it binds to platelets and assembles with the FX activating complex using the EGF2 domain26,27. Therefore, the FIX protein without EGF1 and EGF2 domain in carriers could not function normally, causing severe HB of male carriers.

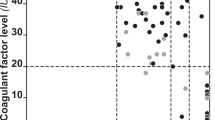
Thrombin generation test and western blotting.
Compared with the control, the plasma factor IX antigen of the patients was severely reduced. The FIX antigen levels of LXF, CD and CDM were reduced to 1.64%, 0.78% and 54.81% level of control, respectively. Because prophylactic infusions of the factor IX concentrate were used in both hemophilic patients, we thought that it would be more meaningful to compare the plasma factor IX antigen level and the ability of the thrombin generation between CDM and CDS. The FIX antigen level of CDM was reduced to 54.81% of the control; however, the endogenous thrombin potential of CDM was equal to that of CDS. The ability of the thrombin generation was significantly different between the patients with HB and the normal control. The main parameters, including the lag time, the area under the curve (ETP) and the peak of the patients, were much lower than those of the control (Fig. 2).
In conclusion, 22 different mutations of the F9 DNA sequence were identified from 23 unrelated patients with HB in this study, 4 of which were novel, including two large F9 gene deletions. Furthermore, we pinpointed and characterized the large deletions, implicating NHEJ and MMBIR as the underlying recombination mechanisms mediating their formation. This study revealed the role of genetic variations in human disorders and highlighted the role that genomic instability may play in predisposition to the formation of pathogenic imbalances.
Additional Information
How to cite this article: Wang, Q.-Y. et al. A genetic analysis of 23 Chinese patients with hemophilia B. Sci. Rep. 6, 25024; doi: 10.1038/srep25024 (2016).
References
Anson, D. S. et al. The gene structure of human anti-haemophilic factor IX. The EMBO journal 3, 1053–1060 (1984).
Yoshitake, S., Schach, B. G., Foster, D. C., Davie, E. W. & Kurachi, K. Nucleotide sequence of the gene for human factor IX (antihemophilic factor B). Biochemistry 24, 3736–3750 (1985).
Bolton-Maggs, P. H. & Pasi, K. J. Haemophilias A and B. Lancet 361, 1801–1809, 10.1016/S0140-6736(03)13405-8 (2003).
White, G. C. 2nd et al. Definitions in hemophilia. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thrombosis and haemostasis 85, 560 (2001).
Li, T., Miller, C. H., Payne, A. B. & Craig Hooper, W. The CDC Hemophilia B mutation project mutation list: a new online resource. Molecular genetics & genomic medicine 1, 238–245, 10.1002/mgg3.30 (2013).
Rallapalli, P. M., Kemball-Cook, G., Tuddenham, E. G., Gomez, K. & Perkins, S. J. An interactive mutation database for human coagulation factor IX provides novel insights into the phenotypes and genetics of hemophilia B. Journal of thrombosis and haemostasis : JTH 11, 1329–1340, 10.1111/jth.12276 (2013).
Hsu, T. C., Nakaya, S. M. & Thompson, A. R. Severe haemophilia B due to a 6 kb factor IX gene deletion including exon 4: non-homologous recombination associated with a shortened transcript from whole blood. Thrombosis and haemostasis 97, 176–180 (2007).
Radic, C. P. et al. Assessment of the F9 genotype-specific FIX inhibitor risks and characterisation of 10 novel severe F9 defects in the first molecular series of Argentinian patients with haemophilia B. Thrombosis and haemostasis 109, 24–33, 10.1160/TH12-05-0302 (2013).
Hewitt, J. et al. Molecular characterization of a 4,409,480 bp deletion of the human X chromosome in a patient with haemophilia B. Haemophilia : the official journal of the World Federation of Hemophilia 20, e230–234, 10.1111/hae.12395 (2014).
Wu, X. et al. Characterisation of large F9 deletions in seven unrelated patients with severe haemophilia B. Thrombosis and haemostasis 112, 459–465, 10.1160/TH13-12-1060 (2014).
Tang, L. et al. Common genetic risk factors for venous thrombosis in the Chinese population. American journal of human genetics 92, 177–187, 10.1016/j.ajhg.2012.12.013 (2013).
Hinks, J. L. et al. A rapid method for haemophilia B mutation detection using conformation sensitive gel electrophoresis. British journal of haematology 104, 915–918 (1999).
Adzhubei, I. A. et al. A method and server for predicting damaging missense mutations. Nature methods 7, 248–249, 10.1038/nmeth0410-248 (2010).
Kumar, P., Henikoff, S. & Ng, P. C. Predicting the effects of coding non-synonymous variants on protein function using the SIFT algorithm. Nature protocols 4, 1073–1081, 10.1038/nprot.2009.86 (2009).
Schwarz, J. M., Rodelsperger, C., Schuelke, M. & Seelow, D. MutationTaster evaluates disease-causing potential of sequence alterations. Nature methods 7, 575–576, 10.1038/nmeth0810-575 (2010).
You, G. L. et al. Characterization of large deletions in the F8 gene using multiple competitive amplification and the genome walking technique. Journal of thrombosis and haemostasis : JTH 11, 1103–1110, 10.1111/jth.12205 (2013).
Li, T. et al. Mutation analysis of a cohort of US patients with hemophilia B. American journal of hematology 89, 375–379, 10.1002/ajh.23645 (2014).
Cutler, J. A., Mitchell, M. J. & Savidge, G. F. More on: unusual expression of the F9 gene in peripheral lymphocytes hinders investigation of F9 mRNA in hemophilia B patients. Journal of thrombosis and haemostasis : JTH 2, 1021, 10.1111/j.1538-7836.2004.00724.x (2004).
Hartmann, L., Theiss, S., Niederacher, D. & Schaal, H. Diagnostics of pathogenic splicing mutations: does bioinformatics cover all bases? Frontiers in bioscience : a journal and virtual library 13, 3252–3272 (2008).
Osterud, B. & Rapaport, S. I. Activation of factor IX by the reaction product of tissue factor and factor VII: additional pathway for initiating blood coagulation. Proceedings of the National Academy of Sciences of the United States of America 74, 5260–5264 (1977).
Di Scipio, R. G., Kurachi, K. & Davie, E. W. Activation of human factor IX (Christmas factor). The Journal of clinical investigation 61, 1528–1538, 10.1172/JCI109073 (1978).
Gailani, D. Activation of factor IX by factor XIa. Trends in cardiovascular medicine 10, 198–204 (2000).
Hastings, P. J., Lupski, J. R., Rosenberg, S. M. & Ira, G. Mechanisms of change in gene copy number. Nature reviews. Genetics 10, 551–564, 10.1038/nrg2593 (2009).
Wang, G. & Vasquez, K. M. Non-B DNA structure-induced genetic instability. Mutation research 598, 103–119, 10.1016/j.mrfmmm.2006.01.019 (2006).
Zhao, J., Bacolla, A., Wang, G. & Vasquez, K. M. Non-B DNA structure-induced genetic instability and evolution. Cellular and molecular life sciences : CMLS 67, 43–62, 10.1007/s00018-009-0131-2 (2010).
Wilkinson, F. H., Ahmad, S. S. & Walsh, P. N. The factor IXa second epidermal growth factor (EGF2) domain mediates platelet binding and assembly of the factor X activating complex. The Journal of biological chemistry 277, 5734–5741, 10.1074/jbc.M107753200 (2002).
Zhong, D., Bajaj, M. S., Schmidt, A. E. & Bajaj, S. P. The N-terminal epidermal growth factor-like domain in factor IX and factor X represents an important recognition motif for binding to tissue factor. The Journal of biological chemistry 277, 3622–3631, 10.1074/jbc.M111202200 (2002).
Acknowledgements
This study was supported by grants from the National Natural Sciences Foundation of China (No. 81370622 and No. 81400099).
Author information
Authors and Affiliations
Contributions
Q.-Y.W. performed and analyzed the experiments, collected the samples and wrote the manuscript; B.H. and H.L. performed and analyzed experiments and collected the samples; L.T. designed, performed and analyzed the experiments and wrote and edited the manuscript; W.Z., Y.-Y.W. and Z.-P.C. performed, analyzed and interpreted the experiments; and Y.H. designed the experiments and interpreted the data, wrote and edited the manuscript and supervised the study. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Wang, QY., Hu, B., Liu, H. et al. A genetic analysis of 23 Chinese patients with hemophilia B. Sci Rep 6, 25024 (2016). https://doi.org/10.1038/srep25024
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep25024
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
