
Abstract
Previous studies have examined the role of three NOS3 gene polymorphisms [G894T, T-786C and the variable number of tandem repeats 4b/a (VNTR 4b/a)] in the susceptibility to preeclampsia with inconclusive findings. We therefore conducted an updated meta-analysis by including more studies. The most appropriate genetic model was chosen for each polymorphism by using a well-established method. Pooled results indicated that, compared with the GT + GG genotype, the TT genotype of G894T was associated with an increased risk of preeclampsia (odds ratio (OR) = 1.46; 95% confidence interval (CI) = 1.21–1.77, P < 0.001; I2 = 40.2%). The CC genotype of T-786C was also associated with a higher risk of preeclampsia (OR = 1.30; 95% CI = 1.07–1.58, P = 0.034; I2 = 46.9%) than the CT + TT genotype. No association was found for VNTR 4b/a. Stratified analysis indicated that the increased risk was evident for high-quality studies both for G894T and T-786C and for studies conducted among Caucasians and Africans for T-786C. However, the increased risk for T-786C among Africans needs further confirmation due to the high probability of false-positive reports. Our results suggested that G894T and T-786C polymorphisms, but not VNTR 4b/a, were associated with an increased risk of preeclampsia.
Similar content being viewed by others

Introduction
Preeclampsia is a clinical syndrome characterized by new-onset of hypertension and proteinuria after 20 weeks of gestation1. It afflicts 3–5% of pregnancies and is a major cause of maternal and prenatal morbidity and mortality worldwide2,3. Essential in the pathogenesis of preeclampsia is endothelial dysfunction due to impaired trophoblast invasion and spiral artery remodeling, resulting in abnormal implantation and placental hypo-perfusion3. Although some dietary, environmental and genetic factors of preeclampsia have been identified, its mechanism is still not well understood; therefore, its prevention remains a challenge.
As a potent vasodilator, circulating nitric oxide (NO) plays a crucial role in endothelial function regulation, blood pressure control and cardiovascular homeostasis and NO is essential for a predisposition to preeclampsia4. NO has been shown in vitro and in vivo to modulate placental circulations and the inhibition of NO production has caused preeclampsia-like syndromes in pregnant rats5. Endothelial nitric oxide synthase (eNOS) is an enzyme which synthesizes NO constitutively via catalyzing the conversion of l-arginine to l-citrulline4. Because endothelial NO availability is largely regulated by its synthesis by eNOS, the gene that encodes eNOS, NOS3, is considered as a candidate gene for preeclampsia6.
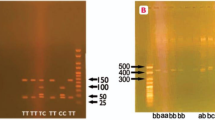
The NOS3 gene is located on chromosome 7q35–36, with a length of 4.4 kb7. The gene comprises 26 exons that encode an mRNA of 4,052 nucleotides7. Because the genomic sequence of NOS3 is highly polymorphic, it was of interest to explore which variant(s) in NOS3 might have a functional potential to affect the bioavailability of eNOS and, thus, affect the risk of preeclampsia7. Three NOS3 polymorphisms have been extensively studied: G894T (a guanine/thymine substitution at position 894 on exon 7 leading to a change from glutamate to aspartate at position 298; rs1799983)8; T-786C mutation (a thymine/cytosine substitution at position 786 in the 5’-flanking region of promoter; rs2070744)9; and a variable number of tandem repeats (VNTR) 4b/a polymorphism [the a* -deletion allele with 27 bp VNTR in intron 4]10.
In 2013, two meta-analyses on the associations between these three polymorphisms and preeclampsia risk were published but with inconsistent results11,12. Since the publication of these meta-analyses, eleven new studies have been published13,14,15,16,17,18,19,20,21,22,23. We have therefore performed an updated systematic review and meta-analysis, adding the recently published studies to further clarify the role of these three SNPs in susceptibility to preeclampsia and to address the limitations of the previous meta-analyses by using more sophisticated methods.
Results
Study characteristics
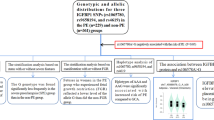
A total of 791 articles were retrieved by a literature search (Fig. 1). Of the publications that were considered to be possibly relevant for the analysis, the following were excluded: two duplicate publications24,25, one study26 that included controls with hypertension in pregnancy, one study with unreliable data27, three studies28,29,30 with controls not in the Hardy-Weinberg equilibrium (HWE) and one study with insufficient data to calculate HWE31. Finally, 41case-control studies, including 5,211 cases and 8,779 controls, were used to evaluate the associations of NOS3 polymorphisms (G894T, T-786C and VNTR 4b/a) with the risk for preeclampsia (Table 1). Thirty articles (3,503 cases and 6,843 controls) were appropriate for combined analysis for G894T, 15 studies (2,232 cases and 3,068 controls) for T-786C and 17 studies (2,091 cases and 2,638 controls) for VNTR 4b/a.

Flow chart of study selection in the meta-analysis.
Table 1 shows the characteristics of included studies. Total sample sizes ranged from 77 to 2,114 (median 255). Twenty-four studies were conducted among Caucasians, 10 among Asians, two among Africans and the remaining five among mixed Caucasians and Africans. The mean age at study was 27.7 years for the cases and 27.6 years for the controls and the mean GAD were 35.7 weeks for cases and 39.2 weeks were controls. The quality scores for all of the included studies ranged from five to 14 with a median of eight. Controls in all of the included studies were population-based and were in HWE (Supplementary Table 1).
Quantitative synthesis
For SNP G894T, OR1 (GG vs. TT) was 1.48 (P < 0.001); OR2 (GT vs. TT) was 1.11 (P = 0.037); and OR3 (GG vs. GT) was 1.44 (P < 0.001), respectively, suggesting that there is a strong recessive association (TT vs. GT + GG) for the putative susceptibility allele T with preeclampsia. The pooled OR and 95% CI for the association between G894T polymorphism and preeclampsia risk was 1.46 (1.21, 1.77) (P < 0.001) with moderate between-study heterogeneity (I2 = 40.2%; Cochran Q = 41.83) (Table 2, Fig. 2). Stratified analysis by the quality scores of included studies revealed a statistically significantly increased risk of preeclampsia only in high-quality studies with scores of 9 to 15 (OR = 1.59, 95% CI = 1.27–2.00; P < 0.001).

Forest plots of associations between nitric oxide synthase 3 polymorphisms and the risk of preeclampsia (A: TT vs. GT + GG for G894T polymorphism; B: CC vs. CT + TT for T-786C polymorphism).
For SNPT-786C, OR1 (TT vs. CC) was 1.36 (P = 0.003); OR2 (CT vs. CC) was 1.06 (P = 0.392); and OR3 (TT vs. CT) was 1.26 (P = 0.029), respectively, also suggesting that there is a recessive association (CC vs. CT + TT) of the putative susceptibility allele C with preeclampsia. The overall fixed OR was significant (OR = 1.30; 95% CI = 1.07–1.58, P = 0.008), with moderate between-study heterogeneity (I2 = 46.9%; Cochran Q = 26.32). In the stratified analysis by ethnicity, the pooled estimate showed a significantly increased risk in the studies conducted among Caucasians (OR = 1.41; 95% CI = 1.11–1.79, P = 0.005) and among Africans (OR = 2.44; 95% CI = 1.26–4.71, P = 0.008). Similar to SNP G894T, when stratified by quality scores, an increased risk was observed only in high-quality studies with scores of 9 to 15 (OR = 1.47; 95% CI = 1.14–1.89, P = 0.003) (Table 2, Fig. 2).
For the VNTR 4b/a, OR1 (bb vs. aa) was 1.24(P = 0.193); OR2 (ab vs. aa) was 1.00 (P = 0.975); and OR3 (bb vs. ab) was1.07 (P = 0.690), respectively, suggesting that there is no association between the VNTR 4b/a polymorphism and preeclampsia risk. No more models were fitted for VNTR 4b/a.
Sensitivity analysis and diagnosis of bias
The sensitivity analyses indicated that no single study could change the pooled ORs obviously for both G894Tand T-786C (Table 2). However, after excluding one study by Serrano et al.32 or Hakli et al.33 the heterogeneity for G894T was significantly reduced, with I2decreasing from 40.2% to 36.0% or 24.9%.
Both Egger’s and Begg’s test revealed no significant publication bias and the P values were 0.634 and 0.508 for G894T and 0.141and 0.276 for T-786C. The funnel plots also indicated no evidence of publication bias both for G894T and T-786C (Fig. 3).

Funnel plots of associations between nitric oxide synthase 3 polymorphisms and the risk of preeclampsia (A: TT vs. GT + GG for G894T polymorphism; B: CC vs. CT + TT for T-786C polymorphism).
The false-positive report probability (FPRP) values for significant findings at different prior probability levels are shown in Table 3. For a prior probability of 0.1, assuming that the OR for a specific genotype was 0.67/1.50 (protection/risk), with a statistical power of 0.710, the FPRP value was 0.009 for G894T with an increased risk of preeclampsia, under the recessive genetic model. A positive association was also observed in the high-quality studies for G894T. Similarly, T-786C was also significantly associated with a preeclampsia risk under the recessive genetic model, with the statistical power of 0.590 and the FPRP value of 0.011 and positive associations were found in the subgroup of Caucasians and high-quality studies. However, we did not find an association between T-786C and preeclampsia risk in the subgroup of Africans due to limited statistical power.
Discussion
In this meta-analysis, we examined the associations between the three NOS3 gene polymorphisms (G894T, T-786C and VNTR 4b/a) and the preeclampsia risk. Our results provide evidence of a significantly increased risk for preeclampsia for G894T and T-786C polymorphisms, under the recessive genetic model. No association was found between VNTR 4b/a and preeclampsia risk. In addition, stratification analysis showed that the association was more evident for high-quality studies both for G894T and T-786C and among mixed Caucasian and African populations for T-786C. However, the results for Africans for T-786C need further confirmation due to the high probability of false-positive reports.
Recently, two meta-analyses were published focusing on NOS3 G894T, T-786C and VNTR 4b/a polymorphisms and the preeclampsia risk11,12. The meta-analysis by Qi et al.12 included 26 studies of 2,863 cases and 5,726 controls for G894T, 13 studies of 1,799 cases and 5,853 controls for T-786C and 15 studies of 1,666 cases and 4,331 controls for T-786C. In the meta-analysis by Qi et al.12, an increased risk of preeclampsia was observed for G894T in the recessive model (OR = 1.43; 95% CI = 1.13–1.82, P = 0.003) with significant between-study heterogeneity (I2 = 50.0%), but no association was observed for T-786C and VNTR 4b/a. Another meta-analysis by Dai et al.11 included 22 studies of 2,265 cases and 3,709 controls for G894T, 11 studies of 1,538 cases and 2,085 controls for T-786C and 11 studies of 1,266 cases and 1,643 controls for VNTR 4b/a polymorphisms. The results found that T-786C polymorphism was associated with an increased preeclampsia risk in the dominant model (OR = 1.17, 95% CI = 1.02 − 1.35; I2 = 44.2%) and that VNTR 4b/a was associated with a high risk in the recessive model (OR = 1.46, 95% CI = 1.01–2.10; I2 = 30.6%). However, no association was observed for G894T (OR = 1.25, 95% CI = 0.96–1.63; I2 = 47.0%).
Our study, with the largest sample size, found a significantly increased risk of preeclampsia for G894T and T-786C polymorphisms, but not for VNTR 4b/a, which were partially consistent with the previous meta-analyses. In addition to the larger number of studies included leading to an increased statistical power, the following reasons could also explain the discrepancy. Firstly, the two previous meta-analyses did not exclude studies with controls not in HWE from the pooled analysis and this may introduce potential selection bias in their findings. Not excluding studies with HWE-violation may result in the overestimation of the statistical significance of some postulated gene-disease associations and it also seemed to modestly increase the between-study heterogeneity in some instances, thus distorting the findings34. In the current meta-analysis, seven studies for G894T14,17,28,29,30,31,35, two studies for T-786C32,36 and four studies for VNTR 4b/a14,18,21,37 deviated from HWE. After adding these studies into the pooled analyses, the overall risk and between-study heterogeneity were not significantly changed except for a significant reduction of heterogeneity for G894T (from 52.5% to 38.8%). However, no significant change was found for T-786C. Secondly, some extracted data in the previous meta-analysis (e.g., revealed in Dai et al.11 Table 1), were not accurate. In addition, studies with unreliable datasets (Tempfer et al.27), with controls having hypertension in pregnancy (Sandrim et al.26) and with duplicate publication24,25 were included in the previous meta-analyses11,27, which may also explain the different results found between our study and the previous meta-analyses.
The evidence that NOS3 G894T and T-786C polymorphisms increase the risk of preeclampsia is biologically plausible. The NOS3 gene is responsible for encoding eNOS, a critical enzyme synthesizing NO through the conversion of L-arginine to L-citrulline in the vascular endothelium, by using molecular oxygen4. Circulating NO, the biologically active free radical, plays critical roles in vascular homeostasis38. Endogenously synthesized NO promotes tissue perfusion by the relaxation of vascular smooth muscle. It may also protect against foam cell formation and media hypertrophy39. A reduced production of NO in women with preeclampsia compared with normal pregnant women was observed40. The chronic inhibition of NO synthesis in pregnant rats led to preeclampsia-like syndromes, such as sustained hypertension, proteinuria, thrombocytopenia and intrauterine growth retardation5. NOS3 G894T polymorphism is located in exon 7 leading to a change from glutamate to aspartate at position 298. This variation was found to be susceptible to cleavage by proteases in endothelial cells and vascular tissue, thus leading to reduced vascular NO synthesis41. G894T has been suggested to reduce eNOS mRNA expression, its activity and NO levels among patients with preeclampsia compared with healthy controls29,31. The T-786C SNP is located in the 5′-flanking region of promoter9. Carriers with the C allele had a significantly reduced luciferase reporter activity and decreased eNOS transcription and endothelial production of NO9, thereby leading to an increased preeclampsia risk.
In the stratified analysis by ethnicity for T-786C, a significantly increased risk of preeclampsia was found in studies conducted among Caucasians and Africans. The significant finding for Caucasians was probably due to the larger sample size in this subgroup. For Africans, the calculation of the FPRP values suggested that the possibility of false-positive reports could not be completely ruled out and this still needs further confirmation. Stratified analyses also found significant results for high-quality studies both for G894T and T-786C polymorphisms, which may suggest an underestimation of the overall effects for these two polymorphisms because of suboptimal studies.
One strength of our meta-analysis is a thorough literature search and review to identify as many studies as possible which are relevant to this topic. To the best of our knowledge, this meta-analysis included the largest number of original investigations in this area, thereby giving it the most sufficient study power. In addition, efforts were made to assess publication biases through Egger’s and Begg’s regression asymmetry test and funnel plot and to pinpoint the potential sources of heterogeneity via stratified and sensitivity analyses. In addition, we used an a priori method to determine the most appropriate genetic model and calculated the FPRP to rule out the potential false-positive reports.
Several limitations of the present study also need to be taken into consideration. Firstly, moderate heterogeneity was found for G894T (40.2%) and T-786C (46.9%). For G894T, after excluding one of the studies32 from the overall analysis, the heterogeneity reduced to 24.9%, but with the result not being significantly changed. However, both subgroup and sensitivity analysis did not find out the source of the heterogeneity for T-786C and this needs further investigation. Secondly, some studies included a category of mixed ethnicity for their study population. These populations could not be included in the ethnicity-specific analysis. Thirdly, some subgroup analysis, e.g., the pooled sample sizes for the subgroup analyses among Asians and Africans for both G894T and T-786C were relatively small (<1,000 for cases) and this may have attenuated the statistical power. Thus, more studies with larger sample sizes are needed to confirm the associations observed in these subgroup analyses. Finally, due to missing information about disease status (e.g., early or late onset; mild or severe disease status), we cannot further explore the associations between NOS3 polymorphisms and preeclampsia risk by disease status and this may also have influenced the interpretation.
In conclusion, this meta-analysis demonstrates that G894T and T-786C polymorphisms, but not VNTR 4b/a, in the NOS3 gene are associated with an increased risk of preeclampsia. The risk is more evident in high-quality studies both for polymorphisms and in studies conducted among Caucasians for T-786C. The risk for the T-786C polymorphism among Africans needs to be further confirmed. More high-quality studies should be conducted to establish the evidence of the associations between the NO synthase 3 gene polymorphisms and the preeclampsia risk for specific ethnic groups and by disease status.
Materials and Methods
Literature search strategies
We followed the standard criteria in the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines to conduct and report this systematic review42. A systematic literature search of PubMed, Embase, Web of Science and China National Knowledge Infrastructure (CNKI, http://www.cnki.net) up to 24 November 2015 was performed. The following search terms were used: (“pregnancy induced hypertension” or pre-eclampsia or preeclampsia or pre eclampsia) and (“nitric oxide synthase” or eNOS or NOS3) and (polymorphism* or allele* or variant* or mutation* or gene or genetic or genotype). No language restriction was applied; non-English articles were translated if necessary. We also scanned the reference lists of retrieved studies and review articles (including meta-analyses) to identify all of the relevant studies on this topic that might have been missed in database searches. Related articles generated by Google Scholar (http://scholar.google.com) and PubMed were also retrieved.
Inclusion and exclusion criteria
Two reviewers (ZFF and ZS) identified articles eligible for further review by independently performing an initial screen of identified titles and abstracts independently. Studies were considered for inclusion if they met the following criteria: (1) they were a case–control study (including nested case-control studies); (2) they used preeclampsia as an end point; (3) they included only apparently healthy controls (i.e., people without known hypertension in pregnancy); (4) they included at least one of the three polymorphisms: G894T, T-786C and VNTR 4b/a; and (5) they provided SNP genotype data and odds ratios (ORs) and corresponding 95% CIs. Studies were excluded if genotype frequency data in the controls demonstrated a departure from HWE. For the studies with overlapping data, only the most relevant articles with the largest dataset were included in the final analysis. Articles were retained when either of the two reviewers believed that they should be retained.
Data extraction and quality assessment
Data were extracted by using a pilot-tested data extraction form. The following data were extracted: article title, the first author’s name, year of publication, country of the study performed, ethnicity of the study population (Caucasian, Asian, African, etc.), number of cases and controls, mean age and gestational age at delivery (GAD) of cases and controls, inclusion and exclusion criteria of the study population, source of controls, preeclampsia diagnosis criteria, genotyping method and the numbers of cases and controls with different genotypes. The ORs and corresponding 95% CIs, after controlling for the minimal and the maximal adjusted number of covariates, were also abstracted.
The quality of each investigation was assessed by quality assessment criteria derived from a previously published meta-analysis of molecular association studies43. The quality scores of the studies ranged from 0 to 15, with 9 to 15 points indicating a high-quality study and 0 to 8 points indicating a low-quality one. The two reviewers (ZFF and ZS) independently extracted data and assessed the quality of each study and any discrepancy was resolved through discussion between the two reviewers until a consensus was reached.
Statistical analysis
The departure of frequencies from expectation under HWE was assessed by chi-square goodness-of-fit tests in controls for each study. The strength of association between the three polymorphisms and preeclampsia risk was assessed by calculating ORs with the corresponding 95% CIs. We used the method proposed by Thakkinstian et al.38 to define the appropriate genetic model for each polymorphism. Briefly, three ORs were calculated for each polymorphism (G894T: OR1: TT vs. GG, OR2: GT vs. GG, OR3: TT vs. GT; T-786C: OR1: CC vs. TT, OR2: CT vs. TT, OR3: CC vs. CT; and VNTR 4b/a: OR1: aa vs. bb, OR2: ab vs. bb, OR3: aa vs. ab, respectively). Then, the most appropriate genetic model was determined by the above pair-wise differences: If OR1 = OR3 ≠ 1 and OR2 = 1, then a recessive model is suggested; If OR1 = OR2 ≠ 1 and OR3 = 1, then a dominant model is suggested; If OR2 = 1/OR3 ≠ 1 and OR1 = 1, then a complete overdominant model is suggested; If OR1 > OR2 > 1 and OR1 > OR3 > 1 (or OR1 < OR2 < 1 and OR1 < OR3 < 1), then a co-dominant model is suggested.
We used the Chi square-based Q-test to assess between-study heterogeneity. The heterogeneity was also quantified with I2 statistics. If no significant heterogeneity was found between the studies, the pooled OR was calculated by using the fixed effects model (the Mantel–Haenszel method)44. Otherwise, the random effects model (the DerSimonian and Laird method) was applied45. The FPRP was calculated to evaluate the significant findings, as described previously46. 0.2 was set as an FPRP threshold and assigned a prior probability of 0.1 to detect an OR of 0.67/1.50 (protective/risk effects) for an association with the genotypes under investigation47. An FPRP value <0.2 was considered as a noteworthy finding. We also performed subgroup analysis according to ethnicity and quality scores, respectively. Sensitivity analysis was used to assess the effect of a single study on the summary results48. Egger’s and Begg’s regression asymmetry test and funnel plot were used to detect publication bias39,49. Statistical analysis was performed with Stata Version 11.0 (College Station, TX, USA) and a two-sided P < 0.05 was considered statistically significant.
Additional Information
How to cite this article: Zeng, F. et al. Associations between nitric oxide synthase 3 gene polymorphisms and preeclampsia risk: a meta-analysis. Sci. Rep. 6, 23407; doi: 10.1038/srep23407 (2016).
References
Schoofs, K. et al. The importance of repeated measurements of the sFlt-1/PlGF ratio for the prediction of preeclampsia and intrauterine growth restriction. J Perinat Med 42, 61–68 (2014).
MacKay, A. P., Berg, C. J. & Atrash, H. K. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet Gynecol 97, 533–538 (2001).
Steegers, E. A., von Dadelszen, P., Duvekot, J. J. & Pijnenborg, R. Pre-eclampsia. Lancet 376, 631–644 (2010).
Moncada, S. & Higgs, A. The L-arginine-nitric oxide pathway. N Engl J Med 329, 2002–2012 (1993).
Molnar, M., Suto, T., Toth, T. & Hertelendy, F. Prolonged blockade of nitric oxide synthesis in gravid rats produces sustained hypertension, proteinuria, thrombocytopenia and intrauterine growth retardation. Am J Obstet Gynecol 170, 1458–1466 (1994).
Hingorani, A. D. Polymorphisms in endothelial nitric oxide synthase and atherogenesis: John French Lecture 2000. Atherosclerosis 154, 521–527 (2001).
Marsden, P. A. et al. Structure and chromosomal localization of the human constitutive endothelial nitric oxide synthase gene. J Biol Chem 268, 17478–17488 (1993).
Hingorani, A. D. et al. A common variant of the endothelial nitric oxide synthase (Glu298–>Asp) is a major risk factor for coronary artery disease in the UK. Circulation 100, 1515–1520 (1999).
Nakayama, M. et al. T-786–>C mutation in the 5’-flanking region of the endothelial nitric oxide synthase gene is associated with coronary spasm. Circulation 99, 2864–2870 (1999).
Zhang, M. X. et al. Biogenesis of short intronic repeat 27-nucleotide small RNA from endothelial nitric-oxide synthase gene. J Biol Chem 283, 14685–14693 (2008).
Dai, B., Liu, T., Zhang, B., Zhang, X. & Wang, Z. The polymorphism for endothelial nitric oxide synthase gene, the level of nitric oxide and the risk for pre-eclampsia: a meta-analysis. Gene 519, 187–193 (2013).
Qi, H. P. et al. Endothelial nitric oxide synthase gene polymorphisms and risk of preeclampsia. Am J Perinatol 30, 795–804 (2013).
Wacholder, S., Chanock, S., Garcia-Closas, M., El Ghormli, L. & Rothman, N. Assessing the probability that a positive report is false: an approach for molecular epidemiology studies. J Natl Cancer Inst 96, 434–442 (2004).
Leonardo, D. P. et al. Association of Nitric Oxide Synthase and Matrix Metalloprotease Single Nucleotide Polymorphisms with Preeclampsia and Its Complications. PLoS One 10, e0136693 (2015).
Ben Ali Gannoun, M. et al. Association of common eNOS/NOS3 polymorphisms with preeclampsia in Tunisian Arabs. Gene 15, 303–307 (2015).
Sakar, M. N. et al. Association of endothelial nitric oxide synthase gene G894T polymorphism and serum nitric oxide levels in patients with preeclampsia and gestational hypertension. J Matern Fetal Neonatal Med, 1–6 (2014).
Groten, T. et al. eNOSI4 and EPHX1 polymorphisms affect maternal susceptibility to preeclampsia: analysis of five polymorphisms predisposing to cardiovascular disease in 279 Caucasian and 241 African women. Arch Gynecol Obstet 289, 581–593 (2014).
Chen, Y., Wang, D., Zhou, M., Chen, X. & Chen, J. Polymorphisms of the endothelial nitric oxide synthase gene in preeclampsia in a Han Chinese population. Gynecol Obstet Invest 77, 150–155 (2014).
Alpoim, P. N. et al. Polymorphisms in endothelial nitric oxide synthase gene in early and late severe preeclampsia. Nitric Oxide 42, 19–23 (2014).
Rahimi, Z., Malek-Khosravi, S., Jalilvand, F. & Parsian, A. MTHFR C677T and eNOS G894T variants in preeclamptic women: Contribution to lipid peroxidation and oxidative stress. Clin Biochem 46, 143–147 (2013).
Rahimi, Z., Aghaei, A., Rahimi, Z. & Vaisi-Raygani, A. Endothelial Nitric Oxide Synthase (eNOS) 4a/b and G894T Polymorphisms and Susceptibility to Preeclampsia. J Reprod Infertil 14, 184–189 (2013).
Coral-Vazquez, R. M. et al. Analysis of polymorphisms and haplotypes in genes associated with vascular tone, hypertension and oxidative stress in Mexican-Mestizo women with severe preeclampsia. Clin Biochem 46, 627–632 (2013).
Perlik, M. et al. Genetic variants of endothelial nitric synthase in gestational hypertension and preeclampsia. Ginekol Pol 83, 652–659 (2012).
Lykke, J. A. et al. Vascular associated gene variants in patients with preeclampsia: results from the Danish National Birth Cohort. Acta Obstet Gynecol Scand 91, 1053–1060 (2012).
Sharma, D., Singh, A., Trivedi, S. S. & Bhattacharjee, J. Intergenotypic variation of nitric oxide and inflammatory markers in preeclampsia: a pilot study in a North Indian population. Hum Immunol 72, 436–439 (2011).
Sharma, D., Trivedi, S. S. & Bhattacharjee, J. 2014Oxidative stress and eNOS (Glu298Asp) gene polymorphism in preeclampsia in Indian population. Mol Cell Biochem 353, 189–193 (2011).
Sandrim, V. C. et al. eNOS haplotypes affect the responsiveness to antihypertensive therapy in preeclampsia but not in gestational hypertension. Pharmacogenomics J 10, 40–45 (2010).
Tempfer, C. B. et al. Polymorphisms of thrombophilic and vasoactive genes and severe preeclampsia: a pilot study. J Soc Gynecol Investig 11, 227–231 (2004).
Sharma, D., Trivedi, S. S. & Bhattacharjee, J. Intergenotypic variation of endothelial dysfunction and inflammatory markers in eclampsia. Hypertens Pregnancy 32, 11–19 (2013).
Sharma, D. et al. Endothelial nitric oxide synthase (eNOS) gene Glu298Asp polymorphism and expression in North Indian preeclamptic women. Pregnancy Hypertens 4, 65–69 (2014).
El-Sherbiny, W. S., Nasr, A. S. & Soliman, A. Endothelial nitric oxide synthase (eNOS) (Glu298Asp) and urotensin II (UTS2 S89N) gene polymorphisms in preeclampsia: prediction and correlation with severity in Egyptian females. Hypertens Pregnancy 32, 292–303 (2013).
Kim, Y. J. et al. Reduced L-arginine level and decreased placental eNOS activity in preeclampsia. Placenta 27, 438–444 (2006).
Serrano, N. C. et al. Endothelial NO synthase genotype and risk of preeclampsia: a multicenter case-control study. Hypertension 44, 702–707 (2004).
Hakli, T. et al. Endothelial nitric oxide synthase polymorphism in preeclampsia. J Soc Gynecol Investig 10, 154–157 (2003).
Trikalinos, T. A., Salanti, G., Khoury, M. J. & Ioannidis, J. P. Impact of violations and deviations in Hardy-Weinberg equilibrium on postulated gene-disease associations. Am JEpidemiol 163, 300–309 (2006).
Chen, L. K. et al. Polymorphisms in the endothelial nitric oxide synthase gene may be protective against preeclampsia in a Chinese population. Reprod Sci 14, 175–181 (2007).
Salimi, S., Naghavi, A., Mokhtari, M., Noora, M. & Yaghmaei, M. Lack of relationship between endothelial nitric oxide synthase gene 4b/a and T-786C polymorphisms with preeclampsia in southeast of Iran. Arch Gynecol Obstet 285, 405–409 (2012).
Diaz-Olguin, L. et al. Endothelial nitric oxide synthase haplotypes are associated with preeclampsia in Maya mestizo women. Dis Markers 31, 83–89 (2011).
Thakkinstian, A., McElduff, P., D’Este, C., Duffy, D. & Attia, J. A method for meta-analysis of molecular association studies. Stat Med 24, 1291–1306 (2005).
Begg, C. B. & Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 50, 1088–1101 (1994).
Davidge, S. T., Stranko, C. P. & Roberts, J. M. Urine but not plasma nitric oxide metabolites are decreased in women with preeclampsia. Am J Obstet Gynecol 174, 1008–1013 (1996).
Tesauro, M. et al. Intracellular processing of endothelial nitric oxide synthase isoforms associated with differences in severity of cardiopulmonary diseases: cleavage of proteins with aspartate vs. glutamate at position 298. Proc Natl Acad Sci USA 97, 2832–2835 (2000).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283, 2008–2012 (2000).
Thakkinstian, A. et al. Systematic review and meta-analysis of the association between complement component 3 and age-related macular degeneration: a HuGE review and meta-analysis. Am J Epidemiol 173, 1365–1379 (2011).
Mantel, N. & Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22, 719–748 (1959).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin Trials 7, 177–188 (1986).
He, J. et al. Genetic variations of mTORC1 genes and risk of gastric cancer in an Eastern Chinese population. Mol Carcinog 52 Suppl 1, E70–79 (2013).
Tobias, A. Assessing the influence of a single study in the meta-anyalysis estimate. Stata Tech Bull 8, 15–17 (1999).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Acknowledgements
This study was supported by the Hong Kong Research Grants Council General Research Fund (No. 473711).
Author information
Authors and Affiliations
Contributions
S.X. and L.K. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: S.X. and L.K.; Acquisition, analysis and interpretation of data: Z.F. and Z.S.; Drafting of the manuscript: Z.F. and Z.S.; Critical revision of the manuscript for important intellectual content: S.X., L.K., W.M.C., Y.Z. and T.J.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zeng, F., Zhu, S., Wong, MS. et al. Associations between nitric oxide synthase 3 gene polymorphisms and preeclampsia risk: a meta-analysis. Sci Rep 6, 23407 (2016). https://doi.org/10.1038/srep23407
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep23407
This article is cited by
-
Association Between Endothelial Nitric Oxide Synthase (eNOS) −786 T/C and 27-bp VNTR 4b/a Polymorphisms and Preeclampsia Development
Reproductive Sciences (2021)
-
Hepatic dysfunction and thrombocytopenia induced by excess sFlt1 in mice lacking endothelial nitric oxide synthase
Scientific Reports (2018)
-
Endothelial nitric oxide synthase gene G894T polymorphism and risk assessment for pregnancy-induced hypertension: evidence from 11 700 subjects
Hypertension Research (2016)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
