
Abstract
Amnestic mild cognitive impairment (aMCI) is a sub-clinical condition characterized by memory deficits that are not severe enough to affect daily functioning. Here we investigated two potential biomarkers found in the cerebrospinal fluid of AD patients, APLP1-derived Aβ-like peptides 28 (APL1β28) and clusterin plasma levels, in terms of their relationship to cognitive function, as reflected in the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA) and the Cognitive Assessment Screening Instrument (CASI) in aMCI patients. Forty-seven aMCI patients and thirty-five age- and gender-matched healthy adult controls were recruited for this study. Using the ELISA method, we found that the mean concentrations of both APL1β28 and clusterin were not significantly different between the control and aMCI groups. The APL1β28 levels were positively correlated with clusterin and that both were negatively correlated with the MMSE scores of the aMCI patients. Clusterin levels were negatively correlated with the MoCA and CASI scores of the aMCI patients. Using multivariate analysis, the correlation between clusterin and MMSE/MoCA/CASI was independent of other AD risk factors including age, education, sex, body mass index and ApoE genotype. The data presented here demonstrate that plasma clusterin levels reflect cognitive function in aMCI patients.
Similar content being viewed by others

Introduction
Amnestic mild cognitive impairment (aMCI), which affects 5–6% of people older than 65, is a syndrome attributed to people with noticeable impairments in memory function but whose other cognitive functions are normal1,2,3,4,5,6,7,8. Similar to other forms of mild cognitive impairment (MCI) such as non-memory (nmMCI) and multi-domain (mMCI) subtypes, aMCI patients retain normal daily activities. It is estimated that, annually, 7% of MCI cases convert to Alzheimer’s disease (AD) and other dementia subtypes9,10, chronic diseases in which the progression of brain changes and cognitive impairments usually appear 10–20 years before the clinical diagnosis. Similar to AD and other forms of MCI, the exact causes of aMCI are not clearly understood, though age and family history are shown to be risk factors. There currently is no cure for dementia, including AD and most clinical trials targeting AD patients in the dementia phases have not shown promising effects. As a result, there have been mounting efforts to identify disease-related changes in the pre-dementia phase, such as in aMCI, for early diagnosis and intervention.
At this time, the diagnosis of aMCI depends mainly on a comprehensive medical evaluation that includes neuropsychological testing and assessment of the patient’s history11,12,13,14,15,16,17,18,19. Biomarkers, including imaging and biochemical substances in the body fluids, assist the disease diagnosis and allow for the monitoring of the pathogenesis. For example, magnetic resonance imaging (MRI) has shown atrophy in the medial temporal lobe, including the hippocampus and entorhinal cortex, in MCI (including aMCI) and AD populations5,20,21,22,23 and carbon 11-labeled PiB (Pittsburgh compound B) PET has demonstrated increased brain amyloid burden in aMCI and AD patients23,24,25,26,27,28,29,30,31,32,33. In addition to imaging methods13,32,33,34,35, body fluid biomarkers are attracting more attention due to their direct relevance to the biology of dementia36,37,38,39. Low concentrations of Aβ42 and high concentrations of total and phosphorylated tau have been detected in the CSF of MCI and AD populations from mono-center and multi-center longitudinal studies40,41,42,43,44,45,46,47,48,49,50. Diagnostic sensitivity to CSF Aβ42 and Tau in MCI patients due to AD is about 50–90% and the specificity is 80–100%40,41,42,43,44,50. Moreover, compared to MRI and CSF biomarkers, the use of plasma biomarkers as a diagnostic tool is relatively low-cost and non-invasive. Based on CSF biomarker studies and on MRI, brain atrophy and Aβ deposits in the patient’s brain suggest that Aβ and proteins implicated in Aβ metabolism are potential monitors for AD and MCI pathogenesis37,38,51,52,53,54,55. Generated by similar β- and γ-cleavages on amyloid-like protein 1 (APLP1, another member of the amyloid precursor protein [APP] gene family), which also includes APLP2 and APP), APL1β28 was recently reported to be a surrogate biomarker for AD with the use of mass spectroscopy56. Similar to APP, which produces the amyloid beta species (Aβ40, Aβ42), a component of senile plaque57,58,59, APLP1 undergoes α-, β- and γ-secretase; unlike APP, however, no Aβ peptide is generated due to the lack of an Aβ sequence in the gene60,61,62,63. The APL1β28 level is higher in the CSF of patients with MCI and familial Alzheimer’s disease (FAD), as well as that in patients with sporadic AD56,64. Besides the Aβ-related APP gene family, proteins implicated in APP metabolism are also potential targets for biomarkers. Clusterin, the third-strongest genetic risk factor for late-onset Alzheimer’s disease (LOAD), is implicated in the clearance process of Aβ accumulation and is associated with the rate of cognitive decline65,66,67,68,69,70. Clusterin, also called apolipoprotein J, is a disulfide-linked heterodimeric protein whose SNPs, according to genome-wide association studies, are linked to AD71,72. Moreover, increased levels of CSF clusterin have been found to be connected to entorhinal atrophy in AD and MCI patients with high Aβ deposition. Plasma clusterin concentration has been reported to be associated with Mini-Mental State Examination (MMSE) scores in combined MCI/AD cohorts73. However, the relationship between the plasma concentrations of APL1β28 and clusterin, two potential biomarkers implicated in APP processing and metabolism, has not been examined in the aMCI population.
Furthermore, there are a number of risk factors that are strongly linked with SAD. For example, the strongest genetic risk factor in the pathogenesis for LOAD and MCI is considered to be ApoE polymorphisms74,75,76,77. Epidemiological studies have shown that age is the most dominant risk factor for the development of AD and MCI78,79,80; a high level of education has also been connected to a lower incidence of AD81,82. Body mass index (BMI) has been shown to be associated with the CSF biomarkers of amyloid and tau in MCI patients83. Thus, whether these factors, combined with plasma APL1β28 and clusterin levels, might have a synergic effect remains to be determined. In the current study, we focused our analysis on aMCI populations and aimed to investigate whether plasma levels of APL1β28 and clusterin are correlated with cognitive status in the aMCI population and whether these correlations have relationships with other risk factors associated with aMCI and AD.
Results
Forty-seven aMCI patients and thirty-five age-matched healthy controls were recruited for our study. All patients were of Chinese Han ethnicity. Detailed demographic data of all aMCI and NC subjects are presented in Table 1. The enzyme-linked immunosorbent assay (ELISA) was performed to determine the absolute concentrations of APL1β28 and clusterin in plasma ([APL1β28]plasma and [clusterin]plasma, respectively) and we adopted ELISA methods that have been applied and validated previously73. The standard curves for APL1β28 (Supplementary Figure 1) and clusterin (Supplementary Figure 2) show reliable and reproducible measurements. Our data indicate that the mean [APL1β28]plasma and [clusterin]plasma levels were not significantly different between the aMCI and control groups (APL1β28: aMCI group, 2.51 ± 0.15 ng/ml, NC group, 2.41 ± 0.17 ng/ml, p = 0.66; clusterin: aMCI group, 115.27 ± 4.30 μg/ml, NC group, 120.32 ± 6.87 μg/ml, p = 0.52). We then performed a one-sample Kolmogorov-Smirnov test on plasma APL1β and clusterin concentrations and on the MMSE, MoCA, CASI scores in the aMCI and NC groups. All data followed a normal distribution except for the MMSE scores in the NC group (Table S1). We thus adopted Spearman’s rank correlation analysis for all the correlations with MMSE in the NC group and Pearson’s correlation for all other correlation analyses. We tested the correlations between plasma APL1β28 and clusterin levels using scores from the MMSE, which is the most widely used screening instrument for cognitive deficits. As shown in Fig. 1A, the analysis of correlations between [APL1β28]plasma and the MMSE scores in the aMCI subjects demonstrated negative correlations (r = −0.293, p = 0.046), while no significant relationship was observed in the NC group (r = −0.028, p = 0.871). A similar result was obtained for plasma clusterin concentration (Fig. 1B, aMCI group: r = −0.377, p = 0.009; NC group: r = −0.096, p = 0.584). These results indicate that aMCI patients with higher APL1β28 or clusterin levels tend to have lower MMSE scores. Furthermore, the correlation between [APL1β28]plasma and [clusterin]plasma was very strong in both the aMCI and NC populations (Fig. 1C, aMCI group: r = 0.518, p < 1.89 × 10−4; NC group: r = 0.445, p = 0.007). Despite the MMSE’s popularity, the test is less sensitive to milder forms of cognitive impairment and can be affected by factors such as race, education and language ability84,85. Thus, other dementia screening tools have been developed and are well known to allow a more comprehensive understanding of other cognitive domains. The CASI, introduced in 1994, features a scale of 100 points86 and combines the MMSE and the Hasegawa Dementia Rating Scale (HDRS)87. Featuring more detailed assessments and broader scoring ranges, the CASI is considered more useful for determining the severity of dementia. In our study, [clusterin]plasma was also found to be negatively correlated with CASI scores in the aMCI subjects (Fig. 2A, r = −0.346, p = 0.017), while [APL1β28]plasma was not found to be correlated (Fig. 2B, r = −0.206, p = 0.164). Additionally, in the NC group, the CASI scores were not correlated with [clusterin]plasma or with [APL1β28]plasma (Fig. 2A, r = −0.115, p = 0.512; Fig. 2B, r = −0.125, p = 0.474).

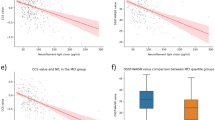
Statistical correlations between MMSE scores and plasma concentrations of APL1β28 and clusterin.
Scatter plots show correlations in all subjects and separately in the individual diagnostic groups. Solid lines indicate linear regression. (A) MMSE scores in the aMCI group (red circle) negatively correlate with APL1β28 concentrations in plasma. (B) MMSE scores in the aMCI group (red circle) negatively correlate with clusterin concentrations in plasma. (C) Plasma concentrations of APL1β28 and clusterin show strong correlations in both the aMCI (red circle) and NC (black triangle) groups. Note: Statistical comparisons were made using the student’s t-test.

Statistical correlations between CASI and MoCA scores and plasma concentrations of APL1β28 and clusterin.
(A) CASI and MoCA scores in the aMCI group (red circle) negatively correlate with clusterin concentrations in plasma. (B) Plasma concentrations of APL1β28 do not correlate with CASI and MoCA scores in the aMCI or NC groups.
The MoCA, introduced by Nasreddine et al.88 in 2005, is designed specifically to be used for patients with MCI or with mild AD. The [clusterin]plasma of aMCI patients, but not that of the controls, was negatively correlated with the MoCA scores (Fig. 2A, aMCI group: r = −0.392, p = 0.012; NC group: r = −0.031, p = 0.870). The MoCA scores in the aMCI and NC groups were not correlated with [APL1β28]plasma (Fig. 2B, left panel, r = 0.068, p = 0.677; Fig. 2B, right panel, r = 0.114, p = 0.542).
Age is unquestionably the strongest risk factor for the development of AD and MCI78,79,80. Thus, we performed multivariate analysis to evaluate whether age is a factor in the correlations between APL1β28 or clusterin levels in plasma and MMSE/MoCA/CASI scores. Our data show that the correlations of clusterin or APL1β28levels with MMSE scores were independent of age (Table 2). After adjusting for age, the correlations of clusterin levels with MoCA or CASI scores remained significant and those of APL1β28 remained not significant. Next, we tested whether education level or sex might affect these correlations. As summarized in Table 2, after adjusting for education and sex, clusterin levels correlate with MMSE, MoCA and CASI significantly; however, only the correlation efficiency of APL1β28 with MMSE showed a trend toward significance (p = 0.055 and 0.059, respectively). The correlation of APL1β28 with MoCA and CASI remained not significant after adjusting for education and sex.
The strongest genetic risk factor in the pathogenesis for AD and MCI is ApoE polymorphisms74,75,76,77. To determine whether there is interaction between the ApoE genotype and plasma APL1β28 and clusterin levels, we compared the average levels of these two proteins in the blood of ApoE ε4-carriers and non-carriers. We used Sanger’s sequencing to examine the ApoE polymorphisms in aMCI and control groups and found that 27.7% of the aMCI patients (13 out of 47) and 25.7% of the control patients (9 out of 35) carried a single copy of ApoE ε4 allele, while no subject carrying two copies was identified in either the aMCI or control groups. Our results show that the plasma levels of APL1β28 and clusterin are not affected by the presence/absence of ApoE ε4 allele (Fig. 3A). Furthermore, we tested the effects of ApoE genotype on the correlations between these two proteins with cognitive scores. The data showed that ApoE genotype has no effect on clusterin’s correlation with MMSE, MoCA and CASI scores, but that it increased the correlation efficiency of APL1β28 with the MMSE score from 0.046 to 0.053. To determine whether BMI is associated with plasma APL1β28 and clusterin levels, we plotted the concentration versus the BMI measured at the time of clinical examination. As shown in Fig. 3B, there is no association between APL1β28 and clusterin levels and BMI values in either aMCI or NC populations (APL1β28-aMCI group: r = −0.238, p = 0.144; NC group: r = 0.010, p = 0.954; clusterin-aMCI group: r = −0.168, p = 0.307; NC group: r = 0.165, p = 0.350).

Statistical correlations between ApoE genotype, BMI and plasma concentrations of APL1β28 and clusterin in the aMCI or NC groups.
(A) No significant changes are observed in the APL1β28 and clusterin levels of the aMCI and NC groups. All summary graphs show a mean ± SEM. (B) Plasma concentrations of APL1β28 and clusterin do not correlate with BMI in the aMCI or NC groups.
Discussion
In this study, we found that the MMSE scores reflecting cognitive ability were negatively correlated with plasma APL1β28 and clusterin levels in aMCI patients but not in the levels of healthy controls. In addition, the plasma clusterin level was also correlated with CASI and MoCA scores in the aMCI population. These results are consistent with findings showing that APL1β28 and clusterin levels in CSF are altered in the MCI, PS1-FAD and sporadic AD patients56,89,90. Since the distribution of MMSE scores in the NC groups were within a narrow range and did not follow a normal distribution, we performed parametric analysis (Pearson’s correlation) and non-parametric analysis (Spearman’s rank correlation) and found no correlations in the NC groups.
The correlation between clusterin and MMSE, MoCA or CASI seems specific, since it is independent of age, education level, BMI and ApoE polymorphisms, as revealed by multivariate analysis. Furthermore, plasma clusterin and APL1β28 levels showed a very strong correlation in both aMCI and control subjects, a finding that is consistent with the notion that they are both involved in the processing of APP. These observations add to the existing evidence that suggests a convergent role of APP dysfunction in the decline of cognitive ability. This finding is consistent with previous reports showing that clusterin interacts with Aβ to cause AD pathology. For instance, clusterin concentrations in CSF show a significant interaction with CSF Aβ1-42 on the atrophy rate of the entorhinal cortex in AD and MCI patients, as well as that in healthy controls89. Moreover, plasma clusterin levels have been found to be an indicator for the rate of cognitive decline and brain atrophy in AD patients73,89,91,92. Although Aβ25-35 treatment of primary neurons elevates intracellular clusterin levels and reduces extracellular-secreted clusterin specifically, treatment with other stressors, including MG132 (the proteasome inhibitor) and ultraviolet irradiation causes cell death without significant changes in clusterin levels. Furthermore, the inactivation of clusterin expression in neurons reduces Aβ-mediated neurotoxicity93. In transgenic mice carrying FAD mutations (PS1M146V, APPSwe, and tauP301L), clusterin in the serum has been reduced by about 30%; this reduction can be fully rescued by treating the mice with coenzyme Q1094.
When compared to those of clusterin, the correlations of APL1β28 with cognitive scores are rather weak, reaching a significant level only when correlated with MMSE (p = 0.046) but not when correlated with MoCA or CASI. Furthermore, after adjustment for sex, education level or ApoE genotype, the correlation remains not significant (p = 0.05–0.06). We speculate that there might be two possibilities for this: the first is that the weak correlation between APL1β28 with MMSE is because APL1β28 strongly correlates with clusterin and clusterin in turn strongly correlates with MMSE. That is to say, the [APL1β28]plasma-MMSE correlation is a consequence of clusterin’s effect on the cognitive ability of aMCI subjects. The second possibility is that the plasma levels of APL1β28 might not accurately reflect the secretase activity in the brain. Therefore, further studies are required to determine whether APL1β share identical cleavage processes with Aβ and whether the levels of [APL1β28]plasma correlate with brain enzymatic activity of α-, β- and γ-secretase and the severity of Aβ peptides deposition in the brain.
Despite the significant increases of CSF clusterin and APL1β28 in AD and MCI patients, the average levels of [APL1β28]plasma and [clusterin]plasma were not different in the aMCI subjects compared to those in the healthy controls, a result that is consistent with a previous study by Thambisetty et al.73. We found that aMCI patients showed an increased trend in clusterin levels and trended toward a decreasing performance in cognitive tests, changes that are identified as potential candidates for early events in the pre-dementia stages. Interestingly, we found that the average levels of [APL1β28]plasma and [clusterin]plasma were not different in the ApoE ε4-carriers and non-carriers. Similar to ApoE, clusterin targets at amyloid-β aggregation and clearance, lipid homeostasis which is related to the pathogenesis of AD65,66,67,68,69. However, the relationship between ApoE ε4 subtypes and brain clusterin levels remains elusive, which might be due to the complication of this disease95. Furthermore, whether the plasma clusterin level reflects the brain clusterin level needs further investigation. In our current study, we did not have enough aMCI-AD conversion cases due to the limited number of aMCI patients and a relatively short monitoring period post-diagnosis. Follow-up cohort studies are needed to evaluate whether the plasma levels of APL1β28 and clusterin could serve as indicators for the conversion rate of aMCI to AD in a Chinese population.
Materials and Methods
Ethics statement
All experiments were conducted in accordance with protocols approved by the institutional review board of Peking University Institute of Mental Health. Legally binding informed consent was obtained from all subjects.
Subjects
All study participants were mainland China citizens of Han ethnicity who were prospectively recruited to establish a case registry at the Dementia Care and Research Center, Peking University Institute of Mental Health. The study, which was conducted from 2006 to 2011, included 47 individuals with amnestic mild cognitive impairment (the aMCI group) and 35 healthy adult controls (the NC group). All the subjects received a clinical review and a battery of neuropsychological tests and laboratory tests; standing body weight was measured with an electronic scale, height (without shoes) was measured with an anthropometer and the BMI was computed based on these parameters (kg weight/m2height).The education level was equated to the amount of time the participant spent in school (elementary school through graduate school).
Diagnostic criteria
The clinical diagnosis of amnestic MCI was based on the criteria established by Petersen96. The diagnostic criteria of aMCI were defined as follows: (1) age ≥ 50 years and met the Petersen criteria; (2) complained of memory impairment that (preferably) could be corroborated by another individual; (3) the impaired memory function was not compatible with patient’s age and/or education; (4) the total MMSE score was no less than 24 and the CDR score was not more than 0.5; (5) the activities of daily living were intact; and (6) DSM-IV criteria for the diagnosis of dementia was not met.
The exclusion criteria were as follows: (1) diagnosed with other neurodegenerative disease; (2) cognitive dysfunction was induced by traumatic brain injuries, tumor or infection; (3) cognitive dysfunction was induced by alcohol or drug use; and (4) cognitive dysfunction was induced for reasons other than mentioned above.
Inclusion criteria for the normal control (NC) group were (1) age ≥ 50 years; (2) no serious physical diseases; and (3) normal cognitive function.
Neuropsychological assessment
These tests were administered using standardized procedures as previously described97,98. In brief, the neuropsychological tests were conducted in Chinese by well-trained and certified evaluators. The evaluators were not informed of the subjects’ diagnoses in advance. The MMSE, the MoCA and the cross-cultural neuropsychological test battery (CCNB), including the Cognitive Ability Screening Instrument (CASI C-2.0), were administered to all participants.
The MMSE, which is widely used as a screening tool to evaluate subjects’ general cognitive function, includes five subtest areas: orientation, registration, recall, attention/concentration/calculation and language; scores range from 0 (severe impairment) to 30 (no impairment)19,99. Further, general cognitive function was assessed with the MoCA and CASI C-2.0, which provide more comprehensive assessment than the MMSE. The CASI includes nine domains: long-term memory, short-term memory, attention, concentration, orientation, reasoning (comprising abstraction and judgment), language abilities, visual construction and category fluency100. The MoCA is designed specifically for patients with MCI or with mild AD. Executive function, short-term memory, language skills and visuo-spatial processing are categories included on the MoCA test.
Quantitative measurements of APL1β28 and clusterin from human plasma
Plasma APL1β28 and clusterin concentrations were assayed by commercially available ELISA kits (Human APL1β28 ELISA, EK-018–42; Human Clusterin ELISA, EK-018-35, Phoenix Pharmaceuticals, Inc.). All samples were run in duplicate.
Apolipoprotein (ApoE) genotype
ApoE genotyping (ε2, ε3 and ε4 allele) was performed on DNA samples from the subjects’ blood, as previously described101.
Statistical analyses
Data analysis was performed using IBM SPSS Statistics 16.0 for Windows. We first used partial correlation analysis to investigate the associations between the cognitive tests and plasma clusterin and APL1β28 levels, respectively. Analyses were adjusted for age, sex, ApoE ε4 status and education when applicable. We then compared differences in plasma clusterin and APL1β28 concentrations between the MCI and control groups (independent sample t-tests) to test the entire sample for differences in plasma clusterin and APL1β 28 concentrations and found no significant differences. Finally, within the diagnostic categories, group comparisons of continuous variables according to their ApoE ε4 status were performed using the student’s t-test, which revealed no significant differences. A priori level of significance was set at p<0.05 for all analyses.
Additional Information
How to cite this article: Meng, Y. et al. A correlativity study of plasma APL1β28 and clusterin levels with MMSE/MoCA/CASI in aMCI patients. Sci. Rep. 5, 15546; doi: 10.1038/srep15546 (2015).
References
Mariani, E., Monastero, R. & Mecocci, P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 12, 23–35 (2007).
Lopez, O. L. et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol 60, 1385–1389 (2003).
Manly, J. J. et al. Implementing diagnostic criteria and estimating frequency of mild cognitive impairment in an urban community. Arch Neurol 62, 1739–1746 (2005).
Koen, J. D. & Yonelinas, A. P. The effects of healthy aging, amnestic mild cognitive impairment and Alzheimer’s disease on recollection and familiarity: a meta-analytic review. Neuropsychol Rev 24, 332–354 (2014).
Hu, Z., Wu, L., Jia, J. & Han, Y. Advances in longitudinal studies of amnestic mild cognitive impairment and Alzheimer’s disease based on multi-modal MRI techniques. Neurosci Bull 30, 198–206 (2014).
Tannenbaum, C., Paquette, A., Hilmer, S., Holroyd-Leduc, J. & Carnahan, R. A systematic review of amnestic and non-amnestic mild cognitive impairment induced by anticholinergic, antihistamine, GABAergic and opioid drugs. Drugs Aging 29, 639–658 (2012).
Simon, S. S., Yokomizo, J. E. & Bottino, C. M. Cognitive intervention in amnestic Mild Cognitive Impairment: a systematic review. Neurosci Biobehav Rev 36, 1163–1178 (2012).
Kidd, P. M. Alzheimer’s disease, amnestic mild cognitive impairment and age-associated memory impairment: current understanding and progress toward integrative prevention. Altern Med Rev 13, 85–115 (2008).
Mitchell, A. J. & Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia—meta-analysis of 41 robust inception cohort studies. Acta Psychiatr Scand 119, 252–265 (2009).
Panza, F. et al. Impact of depressive symptoms on the rate of progression to dementia in patients affected by mild cognitive impairment. The Italian Longitudinal Study on Aging. Int J Geriatr Psychiatry 23, 726–734 (2008).
Langa, K. M. & Levine, D. A. The diagnosis and management of mild cognitive impairment: a clinical review. JAMA 312, 2551–2561 (2014).
Vega, J. N. & Newhouse, P. A. Mild cognitive impairment: diagnosis, longitudinal course and emerging treatments. Curr Psychiatry Rep 16, 490 (2014).
Henderson, T. A. The diagnosis and evaluation of dementia and mild cognitive impairment with emphasis on SPECT perfusion neuroimaging. CNS Spectr 17, 176–206 (2012).
Albert, M. S. et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 270–279 (2011).
Zhang, Y. Y. & Wang, L. N. Diagnosis and intervention of mild cognitive impairment. Zhonghua Liu Xing Bing Xue Za Zhi 25, 905–907 (2004).
Asada, T. Diagnosis of mild cognitive impairment. Seishin Shinkeigaku Zasshi 106, 88–92 (2004).
de Mendonca, A., Guerreiro, M., Ribeiro, F., Mendes, T. & Garcia, C. Mild cognitive impairment: focus on diagnosis. J Mol Neurosci 23, 143–148 (2004).
Robles, A., Del Ser, T., Alom, J. & Pena-Casanova, J. Proposal of criteria for clinical diagnosis of mild cognitive impairment, dementia and Alzheimer’s disease. Neurologia 17, 17–32 (2002).
Markwick, A., Zamboni, G. & de Jager, C. A. Profiles of cognitive subtest impairment in the Montreal Cognitive Assessment (MoCA) in a research cohort with normal Mini-Mental State Examination (MMSE) scores. J Clin Exp Neuropsychol 34, 750–757 (2012).
Chhatwal, J. P. & Sperling, R. A. Functional MRI of mnemonic networks across the spectrum of normal aging, mild cognitive impairment and Alzheimer’s disease. J Alzheimers Dis 31 Suppl 3, S155–167 (2012).
Sperling, R. Functional MRI studies of associative encoding in normal aging, mild cognitive impairment and Alzheimer’s disease. Ann N Y Acad Sci 1097, 146–155 (2007).
Radanovic, M. et al. White matter abnormalities associated with Alzheimer’s disease and mild cognitive impairment: a critical review of MRI studies. Expert Rev Neurother 13, 483–493 (2013).
Dimou, E. et al. Amyloid PET and MRI in Alzheimer’s disease and mild cognitive impairment. Curr Alzheimer Res 6, 312–319 (2009).
Jack, C. R., Jr. et al. Hypothetical model of dynamic biomarkers of the Alzheimer’s pathological cascade. Lancet Neurol 9, 119–128 (2010).
Leuzy, A. et al. Concordance and Diagnostic Accuracy of [11C]PIB PET and Cerebrospinal Fluid Biomarkers in a Sample of Patients with Mild Cognitive Impairment and Alzheimer’s Disease. J Alzheimers Dis 45, 1077–88 (2015).
Jack, C. R., Jr. et al. Serial PIB and MRI in normal, mild cognitive impairment and Alzheimer’s disease: implications for sequence of pathological events in Alzheimer’s disease. Brain 132, 1355–1365 (2009).
Gietl, A. F. et al. Regional cerebral blood flow estimated by early PiB uptake is reduced in mild cognitive impairment and associated with age in an amyloid-dependent manner. Neurobiol Aging 36, 1619–1628 (2015).
Pike, K. E. et al. Beta-amyloid imaging and memory in non-demented individuals: evidence for preclinical Alzheimer’s disease. Brain 130, 2837–2844 (2007).
Koivunen, J. et al. PET amyloid ligand [11C]PIB uptake and cerebrospinal fluid beta-amyloid in mild cognitive impairment. Dement Geriatr Cogn Disord 26, 378–383 (2008).
Forsberg, A. et al. High PIB retention in Alzheimer’s disease is an early event with complex relationship with CSF biomarkers and functional parameters. Curr Alzheimer Res 7, 56–66 (2010).
Jack, C. R., Jr. et al. 11C PiB and structural MRI provide complementary information in imaging of Alzheimer’s disease and amnestic mild cognitive impairment. Brain 131, 665–680 (2008).
Zhang, S. et al. (11)C-PIB-PET for the early diagnosis of Alzheimer’s disease dementia and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev 7, CD010386 (2014).
Noble, J. M. & Scarmeas, N. Application of pet imaging to diagnosis of Alzheimer’s disease and mild cognitive impairment. Int Rev Neurobiol 84, 133–149 (2009).
Hampstead, B. M. & Brown, G. S. Using neuroimaging to inform clinical practice for the diagnosis and treatment of mild cognitive impairment. Clin Geriatr Med 29, 829–845 (2013).
Forlenza, O. V., Diniz, B. S., Teixeira, A. L., Stella, F. & Gattaz, W. Mild cognitive impairment. Part 2: Biological markers for diagnosis and prediction of dementia in Alzheimer’s disease. Rev Bras Psiquiatr 35, 284–294 (2013).
Ritchie, C. et al. Plasma and cerebrospinal fluid amyloid beta for the diagnosis of Alzheimer’s disease dementia and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev 6, CD008782 (2014).
Verhey, F. R. & Visser, P. J. Use of cerebrospinal fluid (CSF) biomarkers for Alzheimer’s type dementia: diagnosis in mild cognitive impairment. Ned Tijdschr Geneeskd 157, A5596 (2013).
Gonzalez-Cuyar, L. F., Sonnen, J. A., Montine, K. S., Keene, C. D. & Montine, T. J. Role of cerebrospinal fluid and plasma biomarkers in the diagnosis of neurodegenerative disorders and mild cognitive impairment. Curr Neurol Neurosci Rep 11, 455–463 (2011).
Mitchell, A. J. CSF phosphorylated tau in the diagnosis and prognosis of mild cognitive impairment and Alzheimer’s disease: a meta-analysis of 51 studies. J Neurol Neurosurg Psychiatry 80, 966–975 (2009).
Riemenschneider, M. et al. Cerebrospinal fluid tau and beta-amyloid 42 proteins identify Alzheimer disease in subjects with mild cognitive impairment. Arch Neurol 59, 1729–1734 (2002).
Zetterberg, H., Wahlund, L. O. & Blennow, K. Cerebrospinal fluid markers for prediction of Alzheimer’s disease. Neurosci Lett 352, 67–69 (2003).
Hampel, H. et al. Value of CSF beta-amyloid1-42 and tau as predictors of Alzheimer’s disease in patients with mild cognitive impairment. Mol Psychiatry 9, 705–710 (2004).
Herukka, S. K., Hallikainen, M., Soininen, H. & Pirttila, T. CSF Abeta42 and tau or phosphorylated tau and prediction of progressive mild cognitive impairment. Neurology 64, 1294–1297 (2005).
Hansson, O. et al. Association between CSF biomarkers and incipient Alzheimer’s disease in patients with mild cognitive impairment: a follow-up study. Lancet Neurol 5, 228–234 (2006).
Herukka, S. K. et al. CSF Abeta42, Tau and phosphorylated Tau, APOE epsilon4 allele and MCI type in progressive MCI. Neurobiol Aging 28, 507–514 (2007).
Hansson, O. et al. Prediction of Alzheimer’s disease using the CSF Abeta42/Abeta40 ratio in patients with mild cognitive impairment. Dement Geriatr Cogn Disord 23, 316–320 (2007).
Bouwman, F. H. et al. CSF biomarkers and medial temporal lobe atrophy predict dementia in mild cognitive impairment. Neurobiol Aging 28, 1070–1074 (2007).
Brys, M. et al. Prediction and longitudinal study of CSF biomarkers in mild cognitive impairment. Neurobiol Aging 30, 682–690 (2009).
Mattsson, N. et al. CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA 302, 385–393 (2009).
Hampel, H. et al. Total and phosphorylated tau protein as biological markers of Alzheimer’s disease. Exp Gerontol 45, 30–40 (2010).
Lewczuk, P., Mroczko, B., Fagan, A. & Kornhuber, J. Biomarkers of Alzheimer’s disease and mild cognitive impairment: a current perspective. Adv Med Sci 60, 76–82 (2015).
Ferreira, D. et al. Improving CSF Biomarkers’ Performance for Predicting Progression from Mild Cognitive Impairment to Alzheimer’s Disease by Considering Different Confounding Factors: A Meta-Analysis. Front Aging Neurosci 6, 287 (2014).
Yamasaki, T. et al. Relevance of in vivo neurophysiological biomarkers for mild cognitive impairment and Alzheimer’s disease. J Alzheimers Dis 31 Suppl 3, S137–154 (2012).
Monge-Argiles, J. A. et al. Biomarkers in the cerebrospinal fluid of patients with mild cognitive impairment: a meta-analysis of their predictive capacity for the diagnosis of Alzheimer’s disease. Rev Neurol 50, 193–200 (2010).
Song, F., Poljak, A., Smythe, G. A. & Sachdev, P. Plasma biomarkers for mild cognitive impairment and Alzheimer’s disease. Brain Res Rev 61, 69–80 (2009).
Yanagida, K. et al. The 28-amino acid form of an APLP1-derived Abeta-like peptide is a surrogate marker for Abeta42 production in the central nervous system. EMBO Mol Med 1, 223–235 (2009).
Goate, A. et al. Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer’s disease. Nature 349, 704–706 (1991).
Murrell, J., Farlow, M., Ghetti, B. & Benson, M. D. A mutation in the amyloid precursor protein associated with hereditary Alzheimer’s disease. Science 254, 97–99 (1991).
Chartier-Harlin, M. C. et al. Early-onset Alzheimer’s disease caused by mutations at codon 717 of the beta-amyloid precursor protein gene. Nature 353, 844–846 (1991).
Slunt, H. H. et al. Expression of a ubiquitous, cross-reactive homologue of the mouse beta-amyloid precursor protein (APP). J Biol Chem 269, 2637–2644 (1994).
Paliga, K. et al. Human amyloid precursor-like protein 1—cDNA cloning, ectopic expression in COS-7 cells and identification of soluble forms in the cerebrospinal fluid. Eur J Biochem 250, 354–363 (1997).
Eggert, S. et al. The proteolytic processing of the amyloid precursor protein gene family members APLP-1 and APLP-2 involves alpha-, beta-, gamma- and epsilon-like cleavages: modulation of APLP-1 processing by n-glycosylation. J Biol Chem 279, 18146–18156 (2004).
Scheinfeld, M. H., Ghersi, E., Laky, K., Fowlkes, B. J. & D’Adamio, L. Processing of beta-amyloid precursor-like protein-1 and -2 by gamma-secretase regulates transcription. J Biol Chem 277, 44195–44201 (2002).
Tagami, S. et al. Relative ratio and level of amyloid-beta 42 surrogate in cerebrospinal fluid of familial Alzheimer disease patients with presenilin 1 mutations. Neurodegener Dis 13, 166–170 (2014).
Li, X. et al. Clusterin in Alzheimer’s disease: a player in the biological behavior of amyloid-beta. Neurosci Bull 30, 162–168 (2014).
Wu, Z. C., Yu, J. T., Li, Y. & Tan, L. Clusterin in Alzheimer’s disease. Adv Clin Chem 56, 155–173 (2012).
Yu, J. T. & Tan, L. The role of clusterin in Alzheimer’s disease: pathways, pathogenesis and therapy. Mol Neurobiol 45, 314–326 (2012).
Nuutinen, T., Suuronen, T., Kauppinen, A. & Salminen, A. Clusterin: a forgotten player in Alzheimer’s disease. Brain Res Rev 61, 89–104 (2009).
Calero, M., Rostagno, A., Frangione, B. & Ghiso, J., Clusterin and Alzheimer’s disease. Subcell Biochem 38, 273–298 (2005).
Calero, M. et al. Apolipoprotein J (clusterin) and Alzheimer’s disease. Microsc Res Tech 50, 305–315 (2000).
Harold, D. et al. Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer’s disease. Nat Genet 41, 1088–1093 (2009).
Lambert, J. C. et al. Genome-wide association study identifies variants at CLU and CR1 associated with Alzheimer’s disease. Nat Genet 41, 1094–1099 (2009).
Thambisetty, M. et al. Association of plasma clusterin concentration with severity, pathology and progression in Alzheimer disease. Arch Gen Psychiatry 67, 739–748 (2010).
Verghese, P. B., Castellano, J. M. & Holtzman, D. M. Apolipoprotein E in Alzheimer’s disease and other neurological disorders. Lancet Neurol 10, 241–252 (2011).
Tycko, B. et al. Polymorphisms in the human apolipoprotein-J/clusterin gene: ethnic variation and distribution in Alzheimer’s disease. Hum Genet 98, 430–436 (1996).
Mui, S. et al. A newly identified polymorphism in the apolipoprotein E enhancer gene region is associated with Alzheimer’s disease and strongly with the epsilon 4 allele. Neurology 47, 196–201 (1996).
Shen, L. et al. Whole genome association study of brain-wide imaging phenotypes for identifying quantitative trait loci in MCI and AD: A study of the ADNI cohort. Neuroimage 53, 1051–1063 (2010).
Wu, C. K. Mild cognitive impairment, healthy aging and Alzheimer’s disease. Med Health R I 91, 132–133 (2008).
Smith, G. Is mild cognitive impairment bridging the gap between normal aging and Alzheimer’s disease? J Neural Transm Suppl 62, 97–104 (2002).
Petersen, R. C. Aging, mild cognitive impairment and Alzheimer’s disease. Neurol Clin 18, 789–806 (2000).
Hall, K. S., Gao, S., Unverzagt, F. W. & Hendrie, H. C. Low education and childhood rural residence: risk for Alzheimer’s disease in African Americans. Neurology 54, 95–99 (2000).
Yasuno, F. et al. Low amyloid-beta deposition correlates with high education in cognitively normal older adults: a pilot study. Int J Geriatr Psychiatry 30, 919–926 (2014).
Vidoni, E. D., Townley, R. A., Honea, R. A. & Burns, J. M. Alzheimer disease biomarkers are associated with body mass index. Neurology 77, 1913–1920 (2011).
Bowie, P., Branton, T. & Holmes, J. Should the Mini Mental State Examination be used to monitor dementia treatments? Lancet 354, 1527–1528 (1999).
Wood, R. Y., Giuliano, K. K., Bignell, C. U. & Pritham, W. W. Assessing cognitive ability in research: use of MMSE with minority populations and elderly adults with low education levels. J Gerontol Nurs 32, 45–54 (2006).
Teng, E. L. et al. The Cognitive Abilities Screening Instrument (CASI): a practical test for cross-cultural epidemiological studies of dementia. Int Psychogeriatr 6, 45–58 (1994).
Hasegawa, K. The clinical assessment of dementia in the aged: A dementia screening scale for psychogeriatric patients in Aging in the eighties and beyond (eds Bergener, M. et al. ) 207–218 (Springer, 1983).
Nasreddine, Z. S. et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53, 695–699 (2005).
Desikan, R. S. et al. The role of clusterin in amyloid-beta-associated neurodegeneration. JAMA Neurol 71, 180–187 (2014).
Okochi, M., Tagami, S. & Takeda, M. Analysis of APL1beta28, a surrogate marker for Alzheimer Abeta42, indicates altered precision of gamma-cleavage in the brains of Alzheimer disease patients. Neurodegener Dis 7, 42–45 (2010).
Sattlecker, M. et al. Alzheimer’s disease biomarker discovery using SOMAscan multiplexed protein technology. Alzheimers Dement 10, 724–734 (2014).
Schrijvers, E. M., Koudstaal, P. J., Hofman, A. & Breteler, M. M. Plasma clusterin and the risk of Alzheimer disease. JAMA 305, 1322–1326 (2011).
Killick, R. et al. Clusterin regulates beta-amyloid toxicity via Dickkopf-1-driven induction of the wnt-PCP-JNK pathway. Mol Psychiatry 19, 88–98 (2014).
Sui, X. et al. Proteomic analysis of serum proteins in triple transgenic Alzheimer’s disease mice: implications for identifying biomarkers for use to screen potential candidate therapeutic drugs for early Alzheimer’s disease. J Alzheimers Dis 40, 575–586 (2014).
Bertrand, P., Poirier, J., Oda, T., Finch, C. E. & Pasinetti, G. M. Association of apolipoprotein E genotype with brain levels of apolipoprotein E and apolipoprotein J (clusterin) in Alzheimer disease. Brain Res Mol Brain Res 33, 174–178 (1995).
Petersen, R. C. et al. Current concepts in mild cognitive impairment. Arch Neurol 58, 1985–1992 (2001).
Zhou, S. et al. The influence of education on Chinese version of Montreal cognitive assessment in detecting amnesic mild cognitive impairment among older people in a Beijing rural community. Scientific World Journal 2014, 689456 (2014).
Wang, X. et al. Apolipoprotein E epsilon4 Modulates Cognitive Profiles, Hippocampal Volume and Resting-State Functional Connectivity in Alzheimer’s Disease. J Alzheimers Dis 45, 781–795 (2015).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12, 189–198 (1975).
Mok, G. S. et al. Evaluation of the screening power of Cognitive Abilities Screening Instrument for probable Alzheimer’s disease using voxel-based morphometry. Clin Imaging 36, 46–53 (2012).
Wang, X., Wang, H., Li, H., Li, T. & Yu, X. Frequency of the apolipoprotein E epsilon4 allele in a memory clinic cohort in Beijing: a naturalistic descriptive study. PLoS One 9, e99130 (2014).
Acknowledgements
This work was supported by grants from the National Basic Research Program of China (2011CB809102, 2014CB942804, 2014BAI03B01 and 2012YQ0302604), National Key Technology R&D Program (2015BAI13B01), the National Science Foundation of China (31222025, 31171025, 81171018) and the National Century Excellent Talents in University of China (NCET-11-0020) and the Seeding Grant for Medicine and Life Sciences of Peking University(2014-MB-11).
Author information
Authors and Affiliations
Contributions
Y.M., H.L. and R.H. carried out the experiments. H.W., J.L., X.Y. and C.Z. contributed to the planning of the work. H.W., X.Y. and C.Z. wrote the paper.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Meng, Y., Li, H., Hua, R. et al. A correlativity study of plasma APL1β28 and clusterin levels with MMSE/MoCA/CASI in aMCI patients. Sci Rep 5, 15546 (2015). https://doi.org/10.1038/srep15546
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep15546
This article is cited by
-
Dynamics of clusterin protein expression in the brain and plasma following experimental traumatic brain injury
Scientific Reports (2019)
-
Integrated Cognitive Assessment: Speed and Accuracy of Visual Processing as a Reliable Proxy to Cognitive Performance
Scientific Reports (2019)
-
Association between clusterin concentration and dementia: a systematic review and meta-analysis
Metabolic Brain Disease (2019)
-
Plasma biomarkers are associated with agitation and regional brain atrophy in Alzheimer’s disease
Scientific Reports (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
