
Abstract
The association between mild renal dysfunction and bone mineral density (BMD) has not been fully explored. It is also unclear how menopausal status and the use of Chinese herb affect this association. This is a cross-sectional study that included a total of 1,419 women aged 40 to 55 years old who were recruited from the MJ Health Management Institution in Taiwan between 2009 and 2010. Spinal BMD was assessed by dual-energy X-ray absorptiometry. Renal function was assessed using estimated glomerular filtration rate (eGFR) and creatinine clearance rate (CCr). The multivariable logistic regression and general linear models were employed to assess the association between renal function and BMD. Stratification analyses were performed by menopausal status and use of Chinese herbs. Low CCr levels were significantly associated with low BMD [adjusted odds ratio (AOR) = 1.48, 95% confidence interval (CI) = 1.15–1.90]. This association was observed in premenopausal women (AOR = 1.43, 95% CI = 1.07–1.92) and in women not taking Chinese herbs (AOR = 1.48, 95% CI = 1.14–1.94). CCr is a better predictor for low BMD in middle-aged women. Menopausal status and the use of Chinese herbs also affected this association.
Similar content being viewed by others
Introduction
Osteoporosis is a disease characterized by low bone mass and loss of bone tissue, resulting in an increased risk of fractures in the spine, hip and wrist1. According to the US National Health and Nutrition Examination Survey (2005–2008), the prevalence of spinal osteoporosis in the elderly was highest among Mexican Americans (women: 24.4%, men: 4.6%), followed by Caucasian Americans (women: 10.9%, men: 2.2%) and African Americans (women: 5.3%, men: data not shown)2. The Nutrition and Health Survey of Taiwan (2005–2008) reported that spinal osteoporosis occurs in 12.6% and 4.3% of women and men of the same age group, respectively3. Osteoporosis is currently considered as an important disease among the elderly.
About 61% and 24% of Caucasian women with osteoporosis have mild to moderate and severe renal disease, respectively4. Patients with chronic kidney disease (CKD) lose the capacity to excrete adequate phosphates and fail to convert vitamin D to 1,25-dihydroxyvitamin D5. These conditions contribute to the development of secondary hyperparathyroidism and the elevation of fibroblast growth factor (FGF)-236, resulting in the release of calcium from the bones and a decrease in bone formation. These characteristics are considered symptoms of a CKD-mineral bone disorder.
Previous studies have shown that dialysis patients are at an increased risk for osteoporosis and hip fractures7,8. However, studies exploring “mild” renal dysfunction (e.g., CKD stages 1 and 2 or decreased renal function) are limited. Earlier reports have reported that decreased renal function was associated with low bone mineral density (BMD) or osteoporosis9,10,11,12; however, these studies were mostly based on small study populations (N = 27 to 659). The use of different methods to estimate renal function [e.g., Cockcroft-Gault (C-G) equation for creatinine clearance rate (CCr) or modification of diet in renal disease (MDRD) equation for estimated glomerular filtration rate (eGFR)] has also led to inconsistencies in the results. In addition, past studies included postmenopausal women only4,9,10,11,12, which does not allow the assessment of the effects of menopause on BMD.
In sum, past studies have focused on severe renal dysfunction and postmenopausal women. To screen low BMD risk at an early age, this study aimed to explore the association of mild renal dysfunction with BMD in middle-aged women. Chinese herbs are known to play an important role in CKD in the Chinese population13,14 because of some harmful ingredients in them. In addition, menopause is a major predictor of BMD. Therefore, this study further assessed how menopausal status and the use of Chinese herbs affected the association between renal function and low BMD.
Materials and Methods
Study population
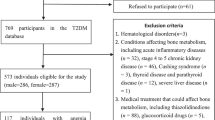
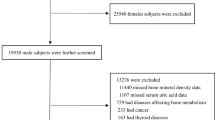
A cross-sectional study was conducted, which consisted of a total of 1,575 Taiwanese women aged 40 to 55 years and underwent health examination at the MJ Health Management Institution in Taipei, Taiwan between 2009 and 2010. Participants with the following conditions or diseases were excluded (N = 156): (1) diseases known to affect BMD levels, e.g., hyperparathyroidism, hyperthyroidism, type 1 diabetes, inflammatory bowel disease, chronic active hepatitis, liver cirrhosis, chronic cholestatic diseases and multiple myeloma (n = 2), (2) medications known to affect BMD, e.g., hormone replacement therapy (n = 60), steroids (n = 6), (3) low BMD of the lumbar spine (n = 86) and (4) lack of blood samples or data for the calculation of eGFR or CCr (n = 2). After exclusion, a total of 1,419 women were included for data analyses. Informed consent was obtained from each participant. The institutional review boards of the MJ Health Management Institution and National Taiwan University approved the study protocol. The present study complied with the guidelines of the World Medical Association Declaration of Helsinki.
A self-reported questionnaire was used to collect information on lifestyle [e.g., smoking, alcohol consumption and regular exercise (≥30 min for 2 to 3 days per week)], menopausal status, disease history (e.g., hypertension and diabetes) and medication history. Menopause was defined as a woman who did not have a period for 12 months, which is not attributable to other biological or physiological causes15.
Determination of bone mineral density
BMD (g/cm2) of the lumbar spine was measured using dual-energy X-ray absorptiometry (DXA, GE Lunar Health Care, DPX-L, USA), which was calibrated using a standard automated test program provided by the manufacturer.
Assessment of renal function and biochemical measurements
eGFR and CCr were used to estimate renal function. According to the 2003 Guidelines of the National Kidney Foundation-Kidney Disease Outcomes Quality Initiative (NKF-KDOQI), the MDRD equation and C-G equation were recommended for the assessment of CKD. A simplified MDRD equation was used to estimate GFR (mL/min/1.73 m2) = 186 × [serum creatinine] − 1.154 × [age] − 0.203 (×0.742 if female). The C-G equation was used to estimate CCr (mL/min) = [(140 − Age) × weight (kg)] (×0.85 if female)/[(serum creatinine) × 72].
Obesity has been known to affect BMD and osteoporosis16. Therefore, measurements relating to the lipid profile of the study participants were collected, e.g., total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol, triglyceride, alkaline phosphatase (ALP), fasting glucose (FG), serum creatinine and uric acid (UA).
Statistical analyses
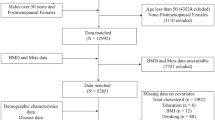
The Student’s t test (for normally-distributed continuous variables), Mann-Whitney U test (for non-normally distributed continuous variables) and χ2 test (for categorical variables) were used to compare the distribution of potential confounders by high and low BMD (T2+T3 vs. T1, defined as below). In addition to the use of continuous BMD variables for data analysis, BMD was further tertiled (T1, T2 and T3) to identify a susceptible population in terms of public health. High BMD was defined as T2 plus T3 and low BMD was defined as T1 (Fig. 1). Grouping was conducted as described in our recent publication17 and other studies18,19. In the present study, only a small portion of participants had abnormal eGFR value when clinical cutoff point was applied (eGFR < 60 mL/min/1.73 m2: 1.1%) because middle-age women are relatively healthy than old women. In addition, our goal is to assess if preclinical renal dysfunction is related to low BMD. Therefore, clinical cutoffs may not be suitable for this population. Similar approaches using Youden’s index to identify cutoff points for a study population were commonly used previously17,20. A general linear regression model was used to estimate adjusted BMD (g/cm2) by renal function. A logistic regression model was used to estimate adjusted odds ratios (AORs) and 95% confidence intervals (CIs) in women with low versus high BMD for eGFR and CCr values, respectively. An ordinal logistic regression model was also applied when treating BMD as an ordinal variable (T1, T2 and T3).

Distribution and tertiles of BMD.
T1: BMD < 1.138 g/cm2; T2: 1.138 g/cm2 ≤ BMD < 1.258 g/cm2; T3: BMD ≥ 1.258 g/cm2. High BMD indicates T2+T3; low BMD indicates T1. Abbreviations: BMD, bone mineral density; T, tertile.
Factors known to affect BMD or osteoporosis were adjusted in the model, e.g., age, menopausal status, body weight, serum ALP, LDL-C, FG, hypertension, use of Chinese herb, UA and body height. Because few participants had abnormal serum ALP values (20 to 140 IU: 0.14%) and no clinical cutoff values were available for body weight and height, these variables were treated as continuous variables in the model.
The impact of menopausal status (yes/no) was explored by generating a product term of renal function and important covariates (e.g., menopausal status and the use of Chinese herb) in the regression models. Stratified analysis was performed based on menopausal status and the use of Chinese herbs, respectively, to establish the relationship between eGFR or CCr and BMD. All analyses were performed using SAS v 9.3 (SAS Institute, Cary, NC). All statistical tests were two-sided and P values < 0.05 were considered statistically significant.
Results
Characteristics of the study population
The present study included a total of 1,419 women. Compared to women with high BMD values, women with low BMD levels were older (47.8 vs. 45.7 years old), had a lower body weight (53.5 vs. 57.1 kg), higher LDL-C values (111.6 vs. 107.1 mg/dL), lower FG values (96.9 vs. 99.1 mg/dL), higher ALP levels (65.1 vs. 56.8 IU), lower CCr values (74.8 vs. 80.5 mL/min) and more participants had experienced menopause (39% vs. 13%, Table 1). The distribution of UA, eGFR, use of Chinese herbs, history of hypertension, cigarette smoking, alcohol consumption, calcium supplement intake and regular exercise were similar between the high and low BMD groups. eGFR was negatively correlated with BMD, body weight and UA (age-adjusted Spearman correlation coefficient: −0.25 to −0.06, P < 0.05). In contrast, CCr was positively correlated with BMD, body weight, hypertension, LDL-C, FG, ALP, UA and eGFR (age-adjusted Spearman correlation coefficient: 0.07 to 0.72, P < 0.05).
Association between renal function (eGFR or CCr) and BMD
Low eGFR values protected against low BMD [<80 vs. ≥80 mL/min/1.73 m2: AOR = 0.69, 95% CI = 0.53–0.89, Table 2]. Low CCr values were associated with an increased risk for low BMD (<78 vs. ≥78 mL/min, AOR = 1.48, 95% CI = 1.15–1.90, Table 2). The logistic regression models (binary BMD) and the ordinal logistic regression models (tertiled BMD) showed similar results (eGFR: <80 vs. ≥80 mL/min/1.73 m2: AOR = 0.64, 95% CI = 0.52–0.80; CCr: <78 vs. ≥78 mL/min, AOR = 1.42, 95% CI = 1.15–1.75).
Adjusted mean BMD according to high and low renal function
After adjusting for other covariates, the mean BMD level was significantly lower in women with high eGFR values (high vs. low eGFR: 1.18 vs. 1.21 g/cm2, P = 0.001, Table 3); the opposite trend was observed for CCr (high vs. low CCr: 1.22 vs. 1.17 g/cm2, P < 0.0001, Table 3).
Stratification by menopausal status
No significant interaction was observed between renal function (eGFR or CCr) and menopausal status (Pinteraction = 0.21 and 0.60, respectively, Table 2). After stratification by menopausal status, low eGFR values showed a protective effect against low BMD in premenopausal women (<80 vs. ≥80 mL/min/1.73 m2: AOR = 0.63, 95% CI = 0.46–0.86, Table 2). In contrast, low CCr values showed an increased risk of low BMD in premenopausal women (<78 vs. ≥78 mL/min: AOR = 1.43, 95% CI = 1.07–1.92, Table 2).
After adjusting for other covariates, among premenopausal women, the mean BMD level was significantly lower in those with high eGFR levels (1.20 g/cm2) compared with those with low eGFR (1.24 g/cm2, P < 0.0001, Table 3); no significant difference in BMD levels was observed in postmenopausal women. In terms of CCr, BMD levels were significantly lower in premenopausal with low CCr (1.20 g/cm2) compared with premenopausal women with high CCr (1.23 g/cm2, P < 0.0001). Similar findings were found in postmenopausal women (high CCr: BMD = 1.14 g/cm2, low CCr: BMD = 1.09 g /cm2, P = 0.001).
Stratification by the use of Chinese herbs
The use of Chinese herbs significantly influenced the association between eGFR and the risk of low BMD (Pinteraction = 0.03). Among women not using Chinese herbs, low eGFR protected against low BMD (AOR = 0.62, 95% CI = 0.47–0.82, Table 4) compared with those with high eGFR. In contrast, in women not using Chinese herbs, low CCr was associated with an increased risk of low BMD (AOR = 1.48, 95% CI = 1.14–1.94, Table 4).
After adjusting for other covariates, among women not using Chinese herbs, the mean BMD level was significantly lower in those with high eGFR (1.19 g/cm2) compared with those with low eGFR (1.21 g/cm2, P = 0.001, Table 5). In contrast, among women not using Chinese herbs, BMD levels were significantly lower in those with low CCr (1.17 g/cm2) compared with those with high CCr (1.22 g/cm2, P < 0.0001, Table 5).
Discussion
Previous studies have shown that advanced CKD was associated with low BMD levels and accelerated bone loss21,22. However, no study has assessed the effectiveness of using mild renal dysfunction in predicting low BMD at an early age. Therefore, this study was aimed to determine this association in a middle-aged, healthy female population. The present study observed that low CCr values were associated with an increased risk of low BMD in premenopausal women (AOR = 1.43); however, previous Caucasian and Japanese studies observed this association in postmenopausal women9,11. In contrast, low eGFR protected against low BMD in premenopausal women (AOR = 0.63), which has not been explored previously. Decreased renal function has been associated with vitamin D deficiency, hyperphosphatemia and hyperparathyroidism5, which in turn results in the release of calcium from bones and a decrease in the rate bone formation. The inconsistencies between the present study and previous investigations might be attributable to the severity of impaired renal function (healthy people vs. advanced CKD patients) and the study population (pre- and postmenopausal women in this study vs. postmenopausal women only in previous studies). Although the C-G and MDRD equations generated similar predictions on renal function among Asians23,24, the contradictory findings between eGFR and CCr in predicting low BMD risk might be attributable to the inclusion of weight, which is an important BMD predictor, in the C-G equation. Both body weight and body mass index (BMI) had major effects on BMD especially weight-bearing bones in women25. In our study, overweight showed a protective effect on low BMD (BMI ≥ 24 vs. 18.5 ≤ BMI < 24, AOR = 0.42, 95% CI = 0.30–0.59). While low BMI was associated with higher risk of low BMD (BMI < 18.5 vs. 18.5 ≤ BMI < 24, AOR = 2.69, 95% CI = 1.61–4.49). Because either BMI or weight is collinear with CCr, statistical models assessing the association between CCr and BMD did not adjust for these variables. Therefore, the findings of the present study indicate that CCr is a better predictor of low BMD compared to eGFR. The following discussion focuses on the findings relating to CCr.
Estrogen induces osteoclast apoptosis, inhibits osteoblast apoptosis and blocks the formation of new osteoclasts to prevent bone loss26,27. Menopausal status is considered an important factor in the maintenance of BMD levels, especially when estrogen levels decrease during menopause. To the best of our knowledge, no study has evaluated the effect of menopausal status or the use of Chinese herbs on the association between renal function and BMD. This study has shown that low CCr values are associated with an increased risk of low BMD in premenopausal women and this effect was further enhanced in postmenopausal women. It is possible that the reduction in estradiol levels might have led to renal injury via its effects on the renin-angiotensin system, wherein rennin levels are elevated in postmenopausal women28. Furthermore, the stronger association observed in postmenopausal women might be a result of accelerated bone loss during late perimenopause and postmenopausal years, whereas minimal changes occur during pre- and early perimenopause29. Additional studies clarifying the interaction between menopause and renal function on BMD are therefore warranted.
Chinese herb is a mixture of different medicinal plants or animal parts. Reports have shown that some Chinese herbs significantly affect renal function30. Ingredients like ephedra used in slimming pills is composed in Chinese herb and can cause nephrolithiasis, while heavy metals (cadmium, arsenic, lead) in contaminated soil where herbs grow up can induce renal dysfunction30,31. Another composition aristolochic acid is a strong carcinogen that can cause kidney interstitial fibrosis, impaired kidney function, urothelial atypias, tumors of the urinary tract and Chinese herb nephropathy14,32,33,34. A Taiwanese study observed that the regular use of Chinese herbs markedly increased the risk of CKD and all-cause mortality35. These properties could explain our findings that low CCr levels were associated with a low BMD risk in women not using Chinese herbs. This association slightly increased but did not reach statistical significance among women who used Chinese herbs, probably because of the small sample size in this subgroup (N = 120). The present study observed that, in women not using Chinese herbs, BMD was significantly higher in those with higher CCr (1.22 g/cm2) than those with low CCr (1.17 g/cm2, P < 0.0001). However, this difference did not reach statistical significance among women using Chinese herbs (high CCr: BMD = 1.18 g/cm2, low CCr: BMD = 1.15 g/cm2, P = 0.28). In addition, BMD levels were lower in women using Chinese herbs (1.16 g/cm2) compared to those who did not (1.20 g/cm2, P = 0.005). It is possible that women with low BMD take Chinese herbs to improve their health. However, low BMD might also be the effect of using Chinese herbs. Because Chinese herbs contain various ingredients that have different effects on BMD, assessing the effects of Chinese herbs on renal function and BMD might be more complicated than previously assumed.
The present study has several strengths. First, the sample size (N = 1,419) is relatively large compared to most previous studies (N = 27 to 659). Second, this study included both pre- and postmenopausal women and thus allowed us to explore how menopausal status influenced the association between renal function and BMD. Third, Chinese herbs are considered as the leading cause of renal insufficiency in Taiwanese people because of some harmful ingredients in them. The inclusion of Chinese herbs in the analysis has helped us clarify the association between renal function and BMD in this Chinese population. The present study also has some limitations. First, this study used a cross-sectional design and thus the causal inference between renal function and BMD was unavailable. In addition, information on the use of Chinese herbs was self-reported, which no further details on the types of herbs and their corresponding doses utilized.
In summary, the present study has shown that CCr is a better predictor of BMD than eGFR because the former incorporated the weight variable, which is an important predictor of BMD, into the equation. Low CCr values were associated with a further increase in the risk of low BMD in postmenopausal women and in women using Chinese herbs. Chinese herbs are commonly used in this population and have been related to poor renal function. It is thus possible that some medications (e.g., bisphosphonates) for the treatment of low BMD might not be appropriate for patients with low renal function (CCr < 35 mL/min)36 . Therefore, physicians should consider renal function during the design of a treatment regimen for female patients with low BMD. Prospective studies exploring the role of CCr in predicting low BMD risk and in designing the appropriate treatment of patients are therefore warranted.
Additional Information
How to cite this article: Sheng, Y.-H. et al. Association of Renal Function and Menopausal Status with Bone Mineral Density in Middle-aged Women. Sci. Rep. 5, 14956; doi: 10.1038/srep14956 (2015).
References
Looker, A. C., Melton, L. J., 3rd, Harris, T. B., Borrud, L. G. & Shepherd, J. A. Prevalence and trends in low femur bone density among older US adults: NHANES 2005–2006 compared with NHANES III. Journal of Bone and Mineral Research 25, 64–71 (2010).
Dawson-Hughes, B. et al. The potential impact of the National Osteoporosis Foundation guidance on treatment eligibility in the USA: an update in NHANES 2005-2008. Osteoporos Int 23, 811–820 (2012).
Lin, Y. C. & Pan, W. H. Bone mineral density in adults in Taiwan: results of the Nutrition and Health Survey in Taiwan 2005-2008 (NAHSIT 2005-2008). Asia Pac J Clin Nutr 20, 283–291 (2011).
Klawansky, S. et al. Relationship between age, renal function and bone mineral density in the US population. Osteoporos Int 14, 570–576 (2003).
Levin, A. et al. Prevalence of abnormal serum vitamin D, PTH, calcium and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 71, 31–38 (2007).
Stubbs, J. R. et al. Longitudinal evaluation of FGF23 changes and mineral metabolism abnormalities in a mouse model of chronic kidney disease. J Bone Miner Res 27, 38–46 (2012).
Stein, M. S., Packham, D. K., Ebeling, P. R., Wark, J. D. & Becker, G. J. Prevalence and risk factors for osteopenia in dialysis patients. Am J Kidney Dis 28, 515–522 (1996).
Alem, A. M. et al. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int 58, 396–399 (2000).
Jassal, S. K., von Muhlen, D. & Barrett-Connor, E. Measures of renal function, bone mineral density, bone Loss and osteoporotic fracture in older adults: The Rancho Bernardo Study. J Bone Miner Res 22, 203–210 (2007).
Briet, M. et al. Age-independent association between arterial and bone remodeling in mild-to-moderate chronic kidney disease. Nephrol Dial Transplant 25, 191–197 (2010).
Kaji, H., Yamauchi, M., Yamaguchi, T., Shigematsu, T. & Sugimoto, T. Mild renal dysfunction is a risk factor for a decrease in bone mineral density and vertebral fractures in Japanese postmenopausal women. J Clin Endocrinol Metab 95, 4635–4642 (2010).
Kim, H. L. et al. A decline in renal function is associated with loss of bone mass in Korean postmenopausal women with mild renal dysfunction. J Korean Med Sci 26, 392–398 (2011).
Lai, M. N. et al. Increased risks of chronic kidney disease associated with prescribed Chinese herbal products suspected to contain aristolochic acid. Nephrology (Carlton) 14, 227–234 (2009).
Nortier, J. L. et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). N Engl J Med 342, 1686–1692 (2000).
National Institute on Aging. Menopause: Time for a Change, < https://www.nia.nih.gov/health/publication/menopause-time-change/introduction-menopause> (Accessed: 6th July 2015).
Dennison, E. M. et al. Lipid profile, obesity and bone mineral density: the Hertfordshire Cohort Study. QJM 100, 297–303 (2007).
You, Y. S. et al. Association between metabolome and low bone mineral density in Taiwanese women determined by (1) H NMR Spectroscopy. J Bone Miner Res 29, 212–222 (2013).
Nock, N. L. et al. Higher bone mineral density is associated with a decreased risk of colorectal adenomas. Int J Cancer 129, 956–964 (2011).
Bidoli, E., Schinella, D. & Franceschi, S. Physical activity and bone mineral density in Italian middle-aged women. Eur J Epidemiol 14, 153–157 (1998).
Parker, C. R., Blackwell, P. J., Freemont, A. J. & Hosking, D. J. Biochemical measurements in the prediction of histologic subtype of renal transplant bone disease in women. Am J Kidney Dis 40, 385–396 (2002).
Spasovski, G. B. et al. Spectrum of renal bone disease in end-stage renal failure patients not yet on dialysis. Nephrol Dial Transplant 18, 1159–1166 (2003).
Nickolas, T. L. et al. Rapid cortical bone loss in patients with chronic kidney disease. J Bone Miner Res 28, 1811–1820 (2013).
Aizawa, M. et al. Comparison of prediction equations of glomerular filtration rate in Japanese adults. Nihon Jinzo Gakkai Shi 48, 62–66 (2006).
Zuo, L. et al. Application of GFR estimating equations in Chinese patients with chronic kidney disease. Am J Kidney Dis 45, 463–472 (2005).
Felson, D. T., Zhang, Y., Hannan, M. T. & JJ, A. Effects of weight and body mass index on bone mineral density in men and women: the Framingham study. J Bone Miner Res 8, 567–573 (1993).
Weitzmann, M. N. & Pacifici, R. Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest 116, 1186–1194 (2006).
Nakamura, T. et al. Estrogen prevents bone loss via estrogen receptor a and induction of Fas ligand in osteoclasts. Cell 130, 811–823 (2007).
Schunkert, H. et al. Effects of estrogen replacement therapy on the renin-angiotensin system in postmenopausal women. Circulation 95, 39–45 (1997).
Finkelstein, J. S. et al. Bone mineral density changes during the menopausetransition in a multiethnic cohort of women. J Clin Endocrinol Metab 93, 861–868 (2008).
Asif, M. A brief study of toxic effects of some medicinal herbs on kidney. Adv Biomed Res 1, 44 (2012).
Thévenod, F. Nephrotoxicity and the proximal tubule. Insights from cadmium. Nephron Physiol 93, 87–93 (2003).
Vanherweghem, J. L. et al. Rapidly progressive interstitial renal fibrosis in young women: association with slimming regimen including Chinese herbs. Lancet 341, 387–391 (1993).
Debelle, F. D. et al. Aristolochic acids induce chronic renal failure with interstitial fibrosis in salt-depleted rats. J Am Soc Nephrol 13, 431–436 (2002).
Cosyns, J. P. et al. Chronic aristolochic acid toxicity in rabbits: a model of Chinese herbs nephropathy? Kidney Int 59, 2164–2173 (2001).
Wen, C. P. et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462293 adults in Taiwan Lancet 371, 2173–2182 (2008).
Markowitz, G. S. et al. Toxic acute tubular necrosis following treatment with zoledronate (Zometa). Kidney Int 64, 281–289 (2003).
Acknowledgements
Funding for the study was provided by National Science Council grants 98-2314-B-002-081 and 99-2314-B-002-128 and by a grant from Academia Sinica.
Author information
Authors and Affiliations
Contributions
S.Y., C.Y. and C.J. wrote the manuscript. C.J., T.K., T.C. and C.Y. conceived this study. C.J.M. and L.Y. offered statistical consultation. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Sheng, YH., Chen, JH., Chiou, JM. et al. Association of Renal Function and Menopausal Status with Bone Mineral Density in Middle-aged Women. Sci Rep 5, 14956 (2015). https://doi.org/10.1038/srep14956
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep14956
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
