
Abstract
The PSMD6 variant rs831571 has been identified as a susceptibility locus for type 2 diabetes mellitus (T2DM). This study aimed to investigate the association of this variant with therapeutic effects of oral antidiabetic drugs in Chinese T2DM patients. 209 newly diagnosed T2DM patients were randomly assigned to treatment with repaglinide or rosiglitazone for 48 weeks and the therapeutic effects were compared. In the rosiglitazone cohort, rs831571 showed significant associations with fasting plasma glucose (FPG), 2-h glucose and decrement of glycated haemoglobin (HbA1c) levels after 24 weeks of treatment (P = 0.0368, 0.0468 and 0.0247, respectively). The C allele was significantly associated with a better attainment of FPG at 24 and 32 weeks (P = 0.0172 and 0.0257, respectively). Survival analyses showed CC homozygotes were more likely to attain a standard FPG level (P = 0.0654). In the repaglinide cohort, rs831571 was significantly associated with decreased HbA1c levels after 24 weeks of treatment, the homeostatic model assessment of insulin resistance and fasting insulin level after 48 weeks of treatment with repaglinide (P = 0.0096, 0235 and 0.0212, respectively). In conclusion, we observed that the PSMD6 variant rs831571 might be associated with the therapeutic effects of rosiglitazone and repaglinide in Chinese T2DM patients. However, these findings need to be confirmed in the future.
Similar content being viewed by others

Introduction
Type 2 diabetes mellitus (T2DM) is a chronic disease that is growing worldwide at an epidemic rate and the huge cost of treatment for T2DM is a heavy public health burden. Despite the availability of various drug classes for the treatment of T2DM, the management of hyperglycaemia is not satisfactory. For all known efficacious interventions, some patients respond to treatment, whereas others do not. This divide has been partly attributed to the various clinical responses to the drugs among individuals. In addition, other factors such as age, gender, liver and renal function, severity of the disease, genetic factors involved in drug absorption, distribution, metabolism and drug target also play an important role in the observed individual variability1.
With the development of genome-wide association studies (GWASs), an increasing number of susceptibility loci for T2DM have been identified. A lot of T2DM susceptibility genes, such as PAX4, KCNQ12,3 and so on, had been reported associated with pharmacogenomics effects of oral antidiabetic drugs including thiazolidinediones (TZDs) and glinides4. The single-nucleotide polymorphism (SNP) rs831571 in PSMD6 gene has been identified as a novel susceptibility locus for T2DM in different ethnic populations5. The encoded protein of PSMD6 gene is a subunit of the 26S proteasome, which is a member of the ubiquitin-proteasome system (UPS)6. UPS is the major cellular machinery responsible for both the recognition and degradation of proteins7 and has also been reported to have important roles in mediating the actions of insulin and insulin secretion8,9.
However, it remains unknown whether this SNP influences the therapeutic effects of oral antihyperglycaemic drugs. Thus, we chose newly diagnosed patients treated with either repaglinide or rosiglitazone to investigate the association of the PSMD6 variant rs831571 with the therapeutic effects of these drugs.
Results
Of the total 105 patients recruited in the rosiglitazone cohort, 93 completed the 48-week study. Of the twelve patients who were withdrawn from the study, one patient had elevated hepatic enzymes, 5 patients with inadequate control of blood glucose were excluded and 6 patients were lost to follow-up. Genotyping was not performed one patient and 92 patients were ultimately included in the statistical analysis. The CC, CT and TT genotype distribution of rs831571 among the rosiglitazone patients was 35, 47 and 10. Of the 104 total patients treated with repaglinide, 91 completed the entire study. Among the 13 patients who withdrew, 4 had a glycated haemoglobin (HbA1c) level ≥8% at two consecutive time points and 9 patients were lost to follow-up. The CC, CT and TT genotype distribution of rs831571 among the repaglinide patients was 34, 50 and 7. The genotype distribution of PSMD6 rs831571 was in agreement with Hardy–Weinberg equilibrium.
Rosiglitazone cohort
The association between rs831571 and clinical parameters before and after rosiglitazone treatment is shown in Table 1. At baseline, there was no significant difference between the genotype groups with regard to all the clinical parameters. After 24 weeks of treatment with rosiglitazone, rs831571 was significantly associated with body mass index (BMI), fasting plasma glucose (FPG) and 2-h glucose (P = 0.0309, 0.0368 and 0.0468, respectively). In addition, rs831571 also showed a significant association with reduced HbA1c levels after 24 weeks of treatment (P = 0.0247). We also observed the trends towards associations between rs831571 with the homeostatic model assessment of beta cell function (HOMA-B) and its augmentation after 24 weeks of rosiglitazone treatment (P = 0.0561 and 0.0547, respectively). Besides, we also found there were differences between different genotype in HbA1c levels after 24 weeks of treatment, the decrement of 2-h glucose after 24 weeks of treatment and HbA1c levels after 48 weeks of treatment (P = 0.0233, 0.0364 and 0.0460, respectively).
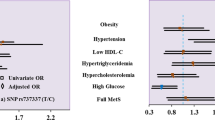
We defined a FPG level of <6.1 mmol/L, a 2-h glucose of <7.8 mmol/L and an HbA1c of <6.5% as attainment and used logistic regression analysis adjusted for age, gender and BMI at baseline to estimate the genotype distributions between two groups with different responses to the drugs. We identified that the rs831571 C allele was significantly associated with a better attainment of FPG at the 24- and 32-week time points (P = 0.0172 and 0.0257, OR (95%CI) = 2.358(1.164, 4.778) and 2.224(1.102, 4.489), respectively). Furthermore, we observed the trends towards associations between the rs831571 C allele and better attainment of FPG at 12 and 48 weeks (P = 0.0680 and 0.0895, OR (95%CI) = 1.904(0.9533, 3.801) and 1.822(0.9115, 3.643), respectively).
We further adopted Cox regression model analysis to explore associations between rs831571 and the rate of attainment of target levels of FPG, 2-h glucose and HbA1c. Survival analyses showed that after adjusting for age, gender and BMI at baseline, rs831571 CC homozygotes were more likely to attain the standard FPG level than the other patients at all assessment points (P = 0.0654).
Repaglinide cohort
The association between PSMD6 rs831571 and clinical features in the repaglinide cohort is shown in Table 2. We found that rs831571 was significantly associated with decreased HbA1c levels after 24 weeks of treatment (P = 0.0096). In addition, rs831571 showed significant associations with the homeostatic model assessment of insulin resistance (HOMA-IR) and fasting insulin level after 48 weeks of treatment with repaglinide (P = 0.0235 and 0.0212, respectively ). Besides, we also observed there were differences in Δvalues of acute insulin response (AIR) to arginine after 24 weeks of treatment, the decrement of FPG and HbA1c levels after 48 weeks of treatment (P = 0.0308, 0.0371 and 0.0101, respectively ).
However, we did not identify any difference in genotype distributions between two groups with different responses to repaglinide and survival analyses showed no difference between genotype groups.
Discussion
Rosiglitazone is a member of the TZD drug family, a class of widely used insulin sensitisers that increase insulin-dependent glucose disposal and reduce hepatic glucose output. TZDs act mainly through nuclear receptor peroxisome proliferator-activated receptor-γ (PPARγ). Acting as agonists of PPARγ, TZDs potentiate insulin signaling and improve insulin sensitivity10,11,12. Besides, recent studies reported TZDs could also have its insulin-sensitizing effects independent of PPARγ. For example, it was reported that TZDs could have its effects by activating of AMP-kinase or binding mitochondrial membranes13. In addition to improving insulin sensitivity and glycaemic control, rosiglitazone has also been shown to preserve pancreatic ß-cell function and insulin secretion14,15. Glinides are a type of fasting insulin secretagogue that could help mimic early-phase insulin release, thus providing improved control of postprandial glucose (PPG) levels16,17. Glinides stimulate insulin secretion by inhibiting ATP-sensitive potassium channels present on the pancreatic β-cell membrane17,18. Repaglinide is one of most widely used glinides and is effective for lowering PPG and HbA1c19,20. In addition, HOMA-B and HOMA-IR were significantly improved after repaglinide treatment in clinical trials21,22,23.
The PSMD6 gene encodes a member of the protease subunit S10 family. The encoded protein is a subunit of the 26S proteasome, which is a member of the UPS, the major cellular machinery responsible for both the recognition and degradation of proteins7. UPS is involved in many biological processes, such as protein quality control, cell cycle regulation, gene expression and regulation of life-span and its alterations are associated with many diseases, including cancer and diabete24,25,26,27,28. UPS has also been reported to have important roles in mediating the actions of insulin and insulin secretion. Indeed, the inappropriate degradation of proteins involved in the insulin signalling pathway such as the insulin receptor substrate (IRS) by UPS can contribute to the development of insulin resistance8,29. Furthermore, the role of UPS in insulin secretion has also been identified and changes in the UPS are involved in human beta cell dysfunction in type 2 diabetes9,30.
In this study, we observed that PSMD6 gene variant rs831571 is associated with the efficacy of rosiglitazone and repaglinide. In the rosiglitazone cohort, rs831571 was significantly associated with BMI, FPG, 2-h glucose and HbA1c levels. HOMA-B was also different among the three genotypes. The rs831571 C allele was significantly associated with better attainment of FPG and this variant also had an influence on the efficacy of repaglinide on HbA1c and HOMA-IR. As mentioned above, UPS plays important roles in insulin sensitivity and insulin secretion. The activity of UPS was associated with β cell function and insulin section. The downregulation of UPS genes and reduced proteasome activity were observed in T2DM islet9. The overactivity of UPS and inappropriate degradation by the UPS of IRS-1 and IRS-2 was associated the development of insulin resistance. Because the 26S proteasome is a component of UPS, SNPs in the PSMD6 gene encoding this component might have an effect on insulin sensitivity and secretion, thus influencing the effect of oral antidiabetic drugs. Nevertheless, all above are our rational speculation and the specific underlying mechanism remains to be elucidated in a future functional study.
Several limitations in this study should be noted when interpreting the results. First, the sample size of this study is relatively small and consequently we may not have had enough statistical power to detect effects of genetic variants on some of the parameters. Second, because we did not adjust for multiple comparisons, we cannot exclude the possibility that our findings were false positive. However, as the variables tested in our study were related, Bonferroni correction was not appropriate and highly conservative. Third, the Kruskal-Wallis test was largely used to analyse the Δ value of parameters among the three genotypes due to the skew distribution; thus, confounding factors such as age, sex, BMI could not be adjusted. Fourth, as the variant of rs831571 is in non-coding area and did not lead to the change of protein function, so we could not carry out the in vitro cellular studies to further reveal the underlying molecular mechanism of its pharmacogenomics effects. Fifth, we do not have a control group in this study and we could not exclude the possibility that we are simply observing the effect of genotype and not specifically modification of the response to the medication. So the findings in this study need to be confirmed in the future study with a proper control group.
In conclusion, we observed that the PSMD6 variant rs831571 might be associated with the therapeutic efficacy of rosiglitazone and repaglinide in Chinese patients with type 2 diabetes. However, in consideration to the limitation of this study and the unknown underlying mechanisms, further studies with a larger sample size and a proper control group as well as functional investigations are necessary in the future.
Methods
Patients and study design
All experiments were carried out according to the guidelines and the regulations of the Ethical Committee of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. The study was approved by the institutional review board of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai, China. Written informed consent was obtained from each patient.
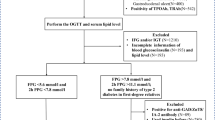
A total of 209 newly diagnosed type 2 diabetes patients, defined according to World Health Organization criteria, were recruited from outpatient clinics in Shanghai, China. Detailed information on this study population has been described previously3,31,32. All patients received no previous pharmacologic therapies for type 2 diabetes prior to the study and were randomly divided into two groups after recruitment. After a 2-week run-in period (diet and exercise therapy only), 104 patients were treated with repaglinide (NovoNorm; Novo Nordisk, Copenhagen, Denmark) and the other 105 patients were given rosiglitazone treatment (Avandia; GlaxoSmithKline, Munich, Germany) for 48 weeks. The patients were visited at weeks 0, 2, 4, 12, 24, 32 and 48 and designed clinical assessments were performed during these visits. Repaglinide was initially administered in a mealtime dosage of 0.5 mg and increased stepwise to 1, 1.5 and 2 mg until the patient achieved a glycaemia target of FPG <7 mmol/L (126 mg/dL) and/or 2 h plasma glucose <11 mmol/L (200 mg/dL). Rosiglitazone treatment was begun with a dosage of 4 mg and titrated to 8 mg when the patient failed to achieve the glycaemic targets. Patients with FPG >13 mmol/L (234 mg/dL), 2hPG >18 mmol/L (324 mg/dL) or HbA1c ≥8% at 2 consecutive time points (a maximal interval of 6 d) were excluded from the study.
Anthropometric and clinical laboratory measurements
General anthropometric parameters including height (in m), weight (in kg) and systolic and diastolic blood pressure (in mmHg) were measured in all patients at baseline and 48 weeks after repaglinide or rosiglitazone treatment. Body mass index (BMI, kg/m2) was calculated as weight/height2.
At each visit (weeks 0, 2, 4, 12, 24, 32 and 48), blood samples were collected after an overnight fast and 2 h after a 75 g oral glucose tolerance test (OGTT). Plasma glucose concentrations were measured using the glucose oxidase-peroxidase method with commercial kits (Shanghai Biological Products Institution, Shanghai, China). HbA1c values were determined by high-performance liquid chromatography using a Bio-Rad Variant II haemoglobin testing system (Bio-Rad Laboratories, Hercules, CA, USA) at weeks −2, 0, 12, 24, 32 and 48. Insulin levels in these samples were measured using radioimmunoassay (Linco Research, St Charles, MO, USA).
Arginine stimulation tests were performed to evaluate potential pancreatic beta-cell function on all patients at the beginning of the run-in period (–2 weeks) and 48 weeks after treatment in overnight-fasted states. We collected blood samples at 0 min and 2, 4 and 6 min after intravenous injection of arginine hydrochloride (10% arginine hydrochloride of 50 mL, 5 g) within 30–60 s. The AIR to arginine (in mU/L) was calculated as the mean insulin value of the 2, 4 and 6 min samples minus the fasting insulin concentration.
We used the homeostatic model assessment to estimate insulin resistance and β-cell function33. HOMA-IR is calculated using the following formula: fasting insulin concentration (in mU/L) × fasting plasma glucose concentration (in mmol/L)/ 22.5. HOMA-B is calculated using the following formula: 20 × fasting insulin concentration/ (fasting plasma glucose concentration - 3.5).
Genotyping
Genomic DNA was extracted from peripheral blood leucocytes in whole blood samples. PSMD6 rs831571 was genotyped by means of matrix-assisted laser desorption/ionisation time-of-flight mass spectroscopy using a MassARRAY platform (MassARRAY Compact Analyser; Sequenom, San Diego, CA, USA). DNA sequencing with a 3130xl Genetic Analyzer (Applied Biosystems, Foster City, CA, USA) was used to confirm the genotyping results.
Statistical analysis
The data are shown as the mean values ± SEM. Allele frequencies were calculated by gene counting and Hardy–Weinberg equilibrium tests were performed. Δvalues were calculated as the final value at week 24 or 48 minus the initial value. Multiple linear regressions adjusted for age, gender, BMI and dosage at baseline or signed rank–sum tests were used to assess the differences in quantitative traits among three genotype groups when appropriate. We defined a FPG of <6.1 mmol/L, a 2-h glucose of <7.8 mmol/L and an HbA1c of <6.5% as attainment. Logistic regression adjusted for age, gender and BMI at baseline was adopted to estimate genotype distributions between two groups with different responses to the drugs using PLINK (v1.07). The attainment rates between the three genotypes groups were compared by Cox regression model analysis adjusted for age, gender and BMI at baseline. A two-tailed P value of <0.05 was considered statistically significant. The statistical analyses were performed using SAS for Windows (version 8.0; SAS Institute, Cary, NC, USA).
Additional Information
How to cite this article: Chen, M. et al. A variant of PSMD6 is associated with the therapeutic efficacy of oral antidiabetic drugs in Chinese type 2 diabetes patients. Sci. Rep. 5, 10701; doi: 10.1038/srep10701 (2015).
References
Eichelbaum, M., Ingelman-Sundberg, M. & Evans, W. E. Pharmacogenomics and individualized drug therapy. Annual review of medicine 57, 119–137 (2006).
Chen, M. et al. Association of PAX4 genetic variants with oral antidiabetic drugs efficacy in Chinese type 2 diabetes patients. The pharmacogenomics journal 14, 488–492 (2014).
Yu, W. et al. Effects of KCNQ1 polymorphisms on the therapeutic efficacy of oral antidiabetic drugs in Chinese patients with type 2 diabetes. Clin Pharmacol Ther 89, 437–442 (2011).
Chen, M., Hu, C. & Jia, W. Pharmacogenomics of glinides. Pharmacogenomics 16, 45–60 (2015).
Cho, Y. S. et al. Meta-analysis of genome-wide association studies identifies eight new loci for type 2 diabetes in east Asians. Nature genetics 44, 67–72 (2012).
Wang, X. et al. Mass spectrometric characterization of the affinity-purified human 26S proteasome complex. Biochemistry 46, 3553–3565 (2007).
Wong, E. & Cuervo, A. M. Integration of clearance mechanisms: the proteasome and autophagy. Cold Spring Harbor perspectives in biology 2, a006734 (2010).
Balasubramanyam, M., Sampathkumar, R. & Mohan, V. Is insulin signaling molecules misguided in diabetes for ubiquitin-proteasome mediated degradation? Molecular and cellular biochemistry 275, 117–125 (2005).
Bugliani, M. et al. Microarray analysis of isolated human islet transcriptome in type 2 diabetes and the role of the ubiquitin-proteasome system in pancreatic beta cell dysfunction. Molecular and cellular endocrinology 367, 1–10 (2013).
Yki-Jarvinen, H. Thiazolidinediones. N Engl J Med 351, 1106–1118 (2004).
Elte, J. W. & Blickle, J. F. Thiazolidinediones for the treatment of type 2 diabetes. European journal of internal medicine 18, 18–25 (2007).
Schoonjans, K. & Auwerx, J. Thiazolidinediones: an update. Lancet 355, 1008–1010 (2000).
Soccio, R. E., Chen, E. R. & Lazar, M. A. Thiazolidinediones and the promise of insulin sensitization in type 2 diabetes. Cell metabolism 20, 573–591 (2014).
Lebovitz, H. E., Dole, J. F., Patwardhan, R., Rappaport, E. B. & Freed, M. I. Rosiglitazone monotherapy is effective in patients with type 2 diabetes. J Clin Endocrinol Metab 86, 280–288 (2001).
Kim, H. S. et al. PPAR-gamma activation increases insulin secretion through the up-regulation of the free fatty acid receptor GPR40 in pancreatic beta-cells. PloS one 8, e50128 (2013).
Dornhorst, A. Insulinotropic meglitinide analogues. Lancet 358, 1709–1716 (2001).
Landgraf, R. Meglitinide analogues in the treatment of type 2 diabetes mellitus. Drugs Aging 17, 411–425 (2000).
Guardado-Mendoza, R., Prioletta, A., Jimenez-Ceja, L. M., Sosale, A. & Folli, F. The role of nateglinide and repaglinide, derivatives of meglitinide, in the treatment of type 2 diabetes mellitus. Archives of medical science : AMS 9, 936–943 (2013).
Rosenstock, J. et al. Repaglinide versus nateglinide monotherapy: a randomized, multicenter study. Diabetes Care 27, 1265–1270 (2004).
Scott, L. J. Repaglinide: a review of its use in type 2 diabetes mellitus. Drugs 72, 249–272 (2012).
Fang, F. S. et al. Comparison of repaglinide and metformin monotherapy as an initial therapy in Chinese patients with newly diagnosed type 2 diabetes mellitus. European journal of endocrinology / European Federation of Endocrine Societies 170, 901–908 (2014).
Li, J. et al. Improvement of insulin sensitivity and beta-cell function by nateglinide and repaglinide in type 2 diabetic patients - a randomized controlled double-blind and double-dummy multicentre clinical trial. Diabetes Obes Metab 9, 558–565 (2007).
Ma, J. et al. Comparison of metformin and repaglinide monotherapy in the treatment of new onset type 2 diabetes mellitus in China. Journal of diabetes research 2014, 294017 2014).
Bedford, L., Paine, S., Sheppard, P. W., Mayer, R. J. & Roelofs, J. Assembly, structure and function of the 26S proteasome. Trends in cell biology 20, 391–401 (2010).
Clague, M. J. & Urbe, S. Ubiquitin: same molecule, different degradation pathways. Cell 143, 682–685 (2010).
Xie, Y. Structure, assembly and homeostatic regulation of the 26S proteasome. Journal of molecular cell biology 2, 308–317 (2010).
Wing, S. S. The UPS in diabetes and obesity. BMC biochemistry 9 (Suppl 1), S6 (2008).
Petroski, M. D. The ubiquitin system, disease and drug discovery. BMC biochemistry 9 (Suppl 1), S7 (2008).
Rome, S., Meugnier, E. & Vidal, H. The ubiquitin-proteasome pathway is a new partner for the control of insulin signaling. Current opinion in clinical nutrition and metabolic care 7, 249–254 (2004).
Hofmeister-Brix, A., Lenzen, S. & Baltrusch, S. The ubiquitin-proteasome system regulates the stability and activity of the glucose sensor glucokinase in pancreatic beta-cells. The Biochemical journal 456, 173–184 (2013).
Wang, J. et al. Effects of ABCA1 variants on rosiglitazone monotherapy in newly diagnosed type 2 diabetes patients. Acta pharmacologica Sinica 29, 252–258 (2008).
He, Y. Y. et al. Association of KCNJ11 and ABCC8 genetic polymorphisms with response to repaglinide in Chinese diabetic patients. Acta pharmacologica Sinica 29, 983–989 (2008).
Matthews, D. R. et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Acknowledgements
We thank all the patients who participated in this study and are appreciative of the doctors and nurses at the Shanghai Clinical Center for Diabetes. This project was funded by 973 Program (2011CB504001), grants from NSFC (81322010, 81170735 and 81300691), 863 Program (2012AA02A509), Excellent Young Medical Expert of Shanghai (XYQ2011041), Shanghai Talent Development Grant (2012041) and National Young Top Talent Supporting Program.
Author information
Authors and Affiliations
Contributions
M.C. and C.H. performed research, analyzed Data and wrote manuscript. W.J. and designed Research. R.Z., F.J., J.W., D.P., S.T., X.S., J.Y., S.W., T.W. and Y.B. performed Research.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Chen, M., Hu, C., Zhang, R. et al. A variant of PSMD6 is associated with the therapeutic efficacy of oral antidiabetic drugs in Chinese type 2 diabetes patients. Sci Rep 5, 10701 (2015). https://doi.org/10.1038/srep10701
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep10701
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
