
Abstract
The incidence of colorectal cancer (CRC) in young patients (≤50 years of age) appears to be increasing. However, their clinicopathological characteristics and survival are controversial. Likewise, the biomarkers are unclear. We used the West China (2008-2013, China), Surveillance, Epidemiology and End Results program (1973-2011, United States) and Linköping Cancer (1972-2009, Sweden) databases to analyse clinicopathological characteristics, survival and multiple biomarkers of young CRC patients. A total of 509,934 CRC patients were included from the three databases. The young CRC patients tended to have more distal location tumours, fewer tumour numbers, later stage, more mucinous carcinoma and poorer differentiation. The cancer-specific survival (CSS) of young patients was significantly better. The PRL (HR = 12.341, 95% CI = 1.615-94.276, P = 0.010), RBM3 (HR = 0.093, 95% CI = 0.012-0.712, P = 0.018), Wrap53 (HR = 1.952, 95% CI = 0.452-6.342, P = 0.031), p53 (HR = 5.549, 95% CI = 1.176-26.178, P = 0.045) and DNA status (HR = 17.602, 95% CI = 2.551-121.448, P = 0.001) were associated with CSS of the young patients. In conclusion, this study suggests that young CRC patients present advanced tumours and more malignant pathological features, while they have a better prognosis. The PRL, RBM3, Wrap53, p53 and DNA status are potential prognostic biomarkers for the young CRC patients.
Similar content being viewed by others


Introduction
Colorectal cancer (CRC) is a major cause of cancer mortality worldwide, with an estimated one million new cases and a half million deaths each year1. In the United States, although incidence of CRC steadily declined2, it is still the third most common cancer and ranked as third leading cause of cancer-related deaths3. The same phenomenon was observed in Sweden, where CRC is the second most common cancer type in both men and women4. In some Asian countries, such as China, the incidence of CRC has increased 2-4 fold and reached to the level of the Western countries during the past decades5.
Besides the improvement of surgical and adjuvant therapy, these decreases of CRC incidence are partially attributed to population based CRC screening which is generally recommended to begin at 50 years of age. In sharp contrast to overall decreasing trends, the incidence of CRC in young patients (≤50 years of age) appears to be increasing6. Since one of the earliest articles describing young CRC patients published in 19397, a series of investigations reported the clinicopathological features and survival of young CRC patients. However, because of the likely biases associated with single-institution experiences or limit cohort sizes, the data vary markedly. Most afflicted individuals lack any identifiable risk factor for their development or potential biomarker for prognosis prediction. The mechanisms underlying the apparent increase in CRC among young patients are poorly understood.
In the present study, we analysed clinicopathological characteristics, prognostic factors and survival of young CRC patients from the West China (WC), Surveillance, Epidemiology and End Results program (SEER) and Linköping Cancer (LC) databases. Furthermore, we assessed the molecular features and the prognostic value of these biomarkers in young CRC patients in LC database.
Results
Patient characteristics
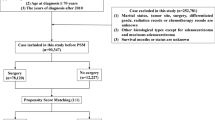
We have identified a total of 509,934 eligible patients with CRC in three databases (n = 5,918 in WC, n = 503,002 in SEER and n = 1,014 in LC). Patient demographic and clinicopathological characteristics of each database are shown in Supplementary Table 1. We divided the patients into two groups according to age for analysis: young group (≤50 years of age at diagnosis, n = 43,821) and elderly group (>50 years of age at diagnosis, n = 466,113). There were 530 (9.0%), 43,236 (8.6%) and 55 (5.4%) young patients in WC, SEER and LC, respectively.
Clinicopathological differences between two age groups
Compared with elderly group, significant differences in young group had been observed concerning the clinicopathological characteristics as follows (Table 1): gender (fewer males in WC and more males in SEER), tumour location (occurring predominately on left colon and the rectum in WC, SEER and LC), tumour numbers (fewer cases with multiple tumours in WC and SEER), TNM stage (later stage in WC and SEER), tumour growth pattern (more frequent in expansive growth in WC), histological type (more mucinous carcinoma in WC and SEER), differentiation (poorer differentiation in WC and SEER), surgical type (more patients underwent radical surgery in WC) and radiotherapy (more patients received radiotherapy in SEER).
Survival differences between two age groups
The follow-up information is available in two databases (SEER and LC). The median follow-up period in SEER and LC was 75 months (range, 0-467 months) and 87 months (range, 0-349 months), respectively. In SEER, the 3, 5, 10-year overall cancer-specific survival (CSS) rates were 73.2%, 66.9%, 61.7% in young group and 66.9%, 60.5%, 54.3% in elderly group, respectively. The CSS of young patients was significantly better than elderly patients (P < 0.001, Figure 1a). In LC, the 3, 5, 10-year overall CSS rates were 76.7%, 74.7%, 66.2% in young group and 71.1%, 62.9%, 56.9% in elderly group, respectively. Similarly, the CSS of young patients was better than elderly patients, although the difference was not statistically significant (P = 0.102, Figure 1b). When the survival analyses were stratified by each stage in SEER and LC, the same trend of CSS at stage I (P < 0.001, P = 0.245, Supplementary Figure 1a), II (P < 0.001, P = 0.152, Supplementary Figure 1b), III (P < 0.001, P = 0.524, Supplementary Figure 1c) and IV (P < 0.001, P = 0.132, Supplementary Figure 1d) had been found.

The cancer-specific survival of young and elderly CRC patients in (a) SEER, P < 0.001 and (b) LC, P = 0.102.
In LC, the 3 and 5-year disease-free survival (DFS) rates were 68.4% and 63.2% in young group and 69.6% and 62.3% in elderly group, respectively. The DFS was not significantly different between two age groups (P = 0.690, Fig. 2). Recurrence rate was 27.6% in young group and 34.1% in elderly group (P = 0.606). In consideration of recurrence type, local recurrence rate (15.8% vs. 13.5%, P = 1.000) and distant metastasis rate (26.3% vs. 35.0%, P = 0.611) had no significant difference between young group and elderly group.

The disease-free survival (DFS) of young and elderly CRC patients in LC. The DFS was not significantly different between two age groups, P = 0.690.
Multiple biomarkers differences between two age groups
The differences of multiple biomarkers between young and elderly group in LC are shown in Table 2. Compared with elderly group, there were more young patients with moderate/strong PRL (phosphatase of regenerating liver, P = 0.014), positive Wrap53 (WD40-encoding RNA antisense to p53, P = 0.017), positive RBM3 (RNA-binding motif protein3, P = 0.018), weak TAZ (Tafazzin, P = 0.044) expression and DNA diploid (P = 0.030). The impact of the studied characteristics on prognosis by univariate analyses is presented in Table 3. In young group, TNM stage, tumour growth pattern, surgical type, recurrence, PRL (hazard ratios, HR = 12.341; 95% confidence intervals, CI = 1.615-94.276; P = 0.010; Supplementary Figure 2a), RBM3 (HR = 0.093, 95% CI = 0.012-0.712, P = 0.018; Supplementary Figure 2b), Wrap53 (HR = 1.952, 95% CI = 0.452-6.342, P = 0.031; Supplementary Figure 2c), p53 (HR = 5.549, 95% CI = 1.176-26.178, P = 0.045; Supplementary Figure 2d) and DNA status (HR = 17.602, 95% CI = 2.551-121.448, P = 0.001; Supplementary Figure 2e) were strongly associated with CSS. Nevertheless, TAZ did not have any prognostic value for CSS although its expression was different in two age groups. Taking into consideration the limited number of young group, we did not further analyse the prognostic value of these biomarkers by multivariable modelling.
Protein-protein interactions (PPIs) network and pathways of biomarkers in young CRC group
All PPIs for each significant biomarker with a confidence score ≥0.4 (medium confidence) were fetched from the Search Tool for the Retrieval of Interacting Genes/Proteins (STRING) resource (Supplementary Table 2). Then the top 10 confident proteins for each biomarker (total 55 proteins) were used to build the final PPIs network (Supplementary Figure 3) and to do the further gene function enrichment analysis. According to the gene ontcology (GO) enrichment analysis, totally 30 GO terms were enriched with statistically significant raw P value and adjusted p value, as shown in Supplementary Table 3, mainly enriched in metabolic process (6 GO terms) and molecular binding functions (8 GO terms, Supplementary Figure 4). With the strict cut-off criterion (adjusted P < 0.001), the Kyoto Encyclopaedia of Genes and Genomes (KEGG) pathway enrichment analysis showed a total of four pathways enriched including pathways of Jak-STAT signalling, cell cycle and p53 signalling, as well as pathways in cancer (Supplementary Table 4).
Discussion
In the present study, we provided large number of CRC patients and extensive clinicopathological data from multiple-institutions in China, U.S. and Sweden. For the first time, the integrated analysis of multiple biomarkers and prognostic factors was performed in young CRC patients compared with elderly patients. Moreover, we utilized the bioinformatics analysis to explore the function of prognostic biomarkers for young CRC patients.
The results described in our study suggested that young CRC patients had distinct clinicopathological characteristics. In accordance with our observations, several investigations showed that CRC in young patients tended to occur predominately on distal location. A literature review of 55 articles concerning young CRC patients exhibited that the sigmoid colon and rectum were the frequent sites (54%)8. Similarly, You YN et al9 identified 64,068 young patients (≤50 years of age) in a large population-based study and found that young-onset CRC commonly arose from the splenic flexure to rectum. Another study based on SEER database also revealed that 32% of CRCs in young patients (35-39 years of age) occurred in the rectum and these percentages decreased to 15.1% in older patients (>85 years of age)10. These findings indicated that the distal colon and rectum were identified as the predilection location of CRC in young patients. It helps us realize that these sites might be the high-yield anatomic regions for endoscopic evaluation in symptomatic young patients and potentially cost-effective targets for screening programs in presymptomatic young adults. In addition, we observed, for the first time, that there were less cases with multiple tumours in young CRC. It is increasingly recognized that a few minor predisposition loci could be responsible for a complex form of CRC heredity11. Therefore, such a genetic predisposition could be involved in a part of young CRC patients. Recently, Kirzin S et al12 found the less frequent synchronous adenoma in sporadic young CRC patients. Taken together, the evidence from this study could reflect accelerated carcinogenesis secondary to predisposing conditions to support this hypothesis.
We showed that young CRC patients had more mucinous carcinoma, poorer differentiation and later stage. A review by O’Connell JB et al8 indicated that 24% of young CRC patients had mucinous or signet-ring cell carcinomas, 27% were poorly differentiated and 66% presented with later stage. You YN et al9 also reported that the poor or undifferentiation and advanced-stage were more commonly in young CRC patients. A large-scale study found that 85% of young CRC patients with poorly differentiated tumour presented at stage III or IV, in comparison to only 15% in the elderly patients13. The potential reason for young CRC patients with later stage might be lower screening rates and delayed diagnosis. Therefore, some researchers have suggested that average-risk screening begin at younger than 50 years of age10.
As with regards to the prognosis of young CRC patients, it remains controversial. In this study, we analysed 43,291 young CRC patients with long follow-up information from two independent databases in U.S. and Sweden. The largest cohort size to date, together with CCS and DFS data, made our results more convincing. Despite these poor prognostic factors likewise have been observed, interestingly, we did find that the 3, 5, 10-year CSS of young patients were significantly better than elderly patients in SEER. The same trend had been seen in LC. The further analysis compared stage-for-stage survival of young with elderly CRC patients. It showed that young patients had better CSS than elderly patients with same stage. Combined with the finding more patients underwent radical surgery and received radiotherapy in young group, our results reflected partially that young patients had a less comorbidities, lower risk of postoperative complications and higher comprehensive treatment completion rate including surgery and adjuvant therapy8. In this study, the young group may include hereditary CRC, particularly Lynch syndrome-associated CRC which typically have improved survival compared with non-Lynch syndrome-related CRC. This might be another reason for better survival in young group. Furthermore, we showed that none of DFS, local recurrence and distant metastasis was significantly different between two age groups, which may be relevant to higher proportions of advanced stage disease as well as poorly differentiated and mucinous tumours in young CRC patients. Overall, young CRC patients present advanced tumours occurring distal location and poorer pathological features; nonetheless, these patients had a better prognosis compared with elderly counterparts.
For the first time, we provided an overview of the panel of CRC-related proteins in our published and unpublished data and performed integrated analysis of more than 25 biomarkers and prognostic factors in CRC patients. Because of the historic association of MSI with Lynch syndrome accounting for 2-7% young CRC patients, most efforts have focused on DNA mismatch repair proteins14. Several studies have shown the increased rates of MSI in young CRC patients15, whereas Yantiss et al16 demonstrated the opposite finding in their cohort, with only 4% of patients younger than 40 having MSI tumours compared to 13% of older controls. In our study, we found no significant difference in microsatellite status across age groups and MSI was not a prognostic biomarker in both young and elderly group. We further found that the PRL, RBM3, Wrap53, TAZ and DNA status were differentially expressed biomarkers between young and elderly group. Additionally, the PRL, RBM3, Wrap53, p53 and DNA status were prognostic biomarkers for young CRC patients. PRL, the gene locating on chromosome 8q24.3, was involved in the metastatic process of CRC. Strong PRL expression could predict resistance to radiotherapy and unfavourable survival in rectal cancer patients with preoperative radiotherapy17. Here, we found that PRL expression was negatively related to the CSS of young CRC patients. As a glycine rich protein, high expression of RBM3 has been found to be associated with good prognosis in several types of cancers, including CRC18. Consistent with these studies, we showed RBM3 positive expression predicted an improved prognosis in young CRC patients. Wrap53 gene encodes a regulatory RNA essential for p53 function upon DNA damage. The Wrap53 overexpression promotes cellular transformation, whereas Wrap53 knockdown triggers apoptosis of cancer cells. In a previous study, we found increased expression of Wrap53 protein was a predict marker for poor prognosis in CRC patients19. Moreover, the p53 positive expression increased with advancing stage and predicted poor survival of CRC patients20. Our present study corroborates the finding by Torsello A et al21 that p53 positive expression was less frequent in young CRC and p53 positivity was an independent predictor of poor survival. Various cancers with increased and abnormal DNA status (DNA non-diploid) have been associated with poor prognosis22. In the present study, fewer patients with DNA non-diploid had been observed in young group. DNA non-diploid was strongly associated with poor CSS of both young and elderly CRC patients. It is accordant to our previous study showing similar result in all-aged CRC patients23.
These significant biomarkers mainly enriched on metabolic process, molecular binding functions and four signalling pathways including Jak-STAT, cell cycle, p53 and pathways in cancer. The Jak-STAT signalling pathway is the important part of PI3K-Akt signalling pathways which were involved in colorectal carcinogenesis. Accumulating evidence demonstrated that the inhibition of Jak-STAT signalling would lead to cell growth inhibition and induction of apoptosis in CRC cells24. Further investigation of these significant biomarkers and their corresponding signalling pathways in a larger population will probably offer the better understanding of the mechanism of underlying cancer development and the prognosis prediction in young CRC patients.
There are several limitations in the present study. Firstly, both the WC and LC databases are collected from a relatively small number of the patients from regional hospitals in China and Sweden, which are not reprehensive of the entire corresponding populations. Although the SEER has been considered a high-quality population-based cancer registry data, it is still limited to 28% of the total U.S. population. Secondly, we are not able to perform a survival analysis in the patients from WC due to a lack of the follow-up data. Thirdly, there is no information on the family history of CRC, therefore we are unable to evaluate the influence of familiar or hereditary CRC particularly Lynch syndrome-associated CRC, if there is, on clinical and biological characteristics. The fourth limitation is that the biomarkers are only examined in a small number of the LC patient samples but not in SEER and WC.
In summary, the present study suggests that young CRC patients have distinct clinicopathological and molecular entity compared to elderly patients. It appears that the young CRC patients tend to occur predominately on distal location, more mucinous carcinoma and poorer differentiation, fewer tumour numbers and to present later stage. However, the overall CSS of young patients is better than elderly patients. The integrated analysis of more than 25 biomarkers shows that PRL, RBM3, Wrap53, TAZ and DNA status are differentially expressed between young and elderly group. Furthermore, the PRL, RBM3, Wrap53, p53 and DNA status are prognostic biomarkers for young CRC patients. The GO and KEGG pathway enrichment analysis suggests that these significant biomarkers mainly enrich on metabolic process, molecular binding functions and four signalling pathways (Jak-STAT, cell cycle, p53 and pathways in cancer). Our results might provide valuable information for refining the previously debatable description of this specific form of CRC and insight into its precise molecular features.
Methods
Database
We respectively used three databases from China, U.S. and Sweden to analyse demographic and clinicopathological characteristics of CRC patients; 1) The WC database included the consecutive patients (2008-2013) from hospitals in the Western China; 2) The SEER database (1973-2011) collected patients from population-based cancer registries in U.S. (based on 2010 census); and 3) The LC database included patients (1972-2009) from the Southeast Swedish Health Care region including hospitals in Linköping, Norrköping, Jönköping, Motala, Eksjö, Varnamo and Vastervik (see supplementary data). The histopathological characteristics, inflammatory infiltration, necrosis and fibrosis were included in this study, according to our published data25.
Biomarker analysis
Immunohistochemistry was performed at our laboratory for the following biomarkers: Astrocyte elevated gene-1 (AEG-1)26, CD16327, c-erbB-228, cyclooxygenase-2 (Cox-2)29, D2-4030, FXYD-331, Ki-6732, Meningioma associated protein 3 (Mac30)33, Nuclear factor-kappaB (NFκB)34, p5320, p7335, Particularly interesting new cysteine-histidine-rich protein (PINCH)36, Peroxisome proliferator-activated receptor delta (PPARD)37, PRL17, ras38, RBM3 (unpublished data), TAZ39 and Wrap5319. The microsatellite status (microsatellite stability, MSS; microsatellite instability, MSI) was determined by PCR based assays as previous describing40. Apoptotic cells were detected by the terminal deoxynucleotidy transferase-mediated dUTP-biotin nick end-labelling (TUNEL) assay41. DNA content and S-phase fraction (SPF) were measured by flow cytometry. The details were described previously23.
Functional analysis
To further analyse the function of the significant biomarkers, STRING resource was utilized for PPIs network analysis42 and the WEB-based Gene Set Analysis Toolkit (WebGestalt) was performed for comprehensive gene functional enrichment analysis43, including GO enrichment and KEGG pathway enrichment analysis44
Statistical analysis
The relationships of age groups with clinicopathological characteristics and biomarkers were analysed by Chi-square (χ2) test. Survival curves were generated using Kaplan-Meier estimates, differences between the curves were analysed by log-rank test. The impact of each characteristic on survival was examined by the Cox’s proportional hazard regression models. The data were summarized with HR and their 95% CI. The test was two-sided and a P value of less than 0.05 was considered statistically significant. All statistical analyses were performed using R software ( http://www.R-project.org/). For details, see supplementary data.
Additional Information
How to cite this article: Wang, M.-J. et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci. Rep. 5, 10645; doi: 10.1038/srep10645 (2015).
References
Garcia, M. et al. Global Cancer Facts & Figures 2007. Atlanta, GA: American Cancer Society (2007), www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf. [accessed March 1, 2015].
Edwards, B. K. et al. Annual report to the nation on the status of cancer, 1975-2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening and treatment) to reduce future rates. Cancer 116, 544–573 (2010).
Siegel, R., Naishadham, D. & Jemal, A. Cancer statistics, 2013. CA Cancer J Clin 63, 11–30 (2013).
Allemani, C. et al. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 385, 977–1010 (2015).
Sung, J. J., Lau, J. Y., Goh, K. L., Leung, W. K. & Asia Pacific Working Group on Colorectal, C. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 6, 871–876 (2005).
Siegel, R. L., Jemal, A. & Ward, E. M. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev 18, 1695–1698 (2009).
Bacon, H. E. & Sealy, W. B. Malignancy of the anus, rectum and sigmoid colon in the young: With report of a case at four and a half years. Am J Surg 45, 9 (1939).
O’Connell, J. B., Maggard, M. A., Livingston, E. H. & Yo, C. K. Colorectal cancer in the young. Am J Surg 187, 343–348 (2004).
You, Y. N., Xing, Y., Feig, B. W., Chang, G. J. & Cormier, J. N. Young-onset colorectal cancer: is it time to pay attention? Arch Intern Med 172, 287–289 (2012).
Davis, D. M. et al. Is it time to lower the recommended screening age for colorectal cancer? J Am Coll Surg 213, 352–361 (2011).
Cicek, M. S. et al. Colorectal cancer linkage on chromosomes 4q21, 8q13, 12q24 and 15q22. PLoS One 7, e38175 (2012).
Kirzin, S. et al. Sporadic early-onset colorectal cancer is a specific sub-type of cancer: a morphological, molecular and genetics study. PLoS One 9, e103159 (2014).
Marble, K., Banerjee, S. & Greenwald, L. Colorectal carcinoma in young patients. J Surg Oncol 51, 179–182 (1992).
Boland, C. R. & Goel, A. Microsatellite instability in colorectal cancer. Gastroenterology 138, 2073–2087, e2073 (2010).
Liang, J. T. et al. Clinicopathological and molecular biological features of colorectal cancer in patients less than 40 years of age. Br J Surg 90, 205–214 (2003).
Yantiss, R. K. et al. Clinical, pathologic and molecular features of early-onset colorectal carcinoma. Am J Surg Pathol 33, 572–582 (2009).
Wallin, A. R., Svanvik, J., Adell, G. & Sun, X. F. Expression of PRL proteins at invasive margin of rectal cancers in relation to preoperative radiotherapy. Int J Radiat Oncol Biol Phys 65, 452–458 (2006).
Hjelm, B. et al. High nuclear RBM3 expression is associated with an improved prognosis in colorectal cancer. Proteomics Clin Appl 5, 624–635 (2011).
Zhang, H., Wang, D. W., Adell, G. & Sun, X. F. WRAP53 is an independent prognostic factor in rectal cancer- a study of Swedish clinical trial of preoperative radiotherapy in rectal cancer patients. BMC Cancer 12, 294 (2012).
Sun, X. F. et al. Prognostic significance of cytoplasmic p53 oncoprotein in colorectal adenocarcinoma. Lancet 340, 1369–1373 (1992).
Torsello, A. et al. P53 and bcl-2 in colorectal cancer arising in patients under 40 years of age: distribution and prognostic relevance. Eur J Cancer 44, 1217–1222 (2008).
Krajcovic, M. & Overholtzer, M. Mechanisms of ploidy increase in human cancers: a new role for cell cannibalism. Cancer Res 72, 1596–1601 (2012).
Sun, X. F. Clinicopathological and biological features of DNA tetraploid colorectal cancers. Cancer J 12, 501–506 (2006).
Slattery, M. L., Lundgreen, A., Kadlubar, S. A., Bondurant, K. L. & Wolff, R. K. JAK/STAT/SOCS-signaling pathway and colon and rectal cancer. Mol Carcinog 52, 155–166 (2013).
Knutsen, A., Adell, G. & Sun, X. F. Inflammatory infiltration, fibrosis, necrosis and mucinous content in relation to clinicopathological and molecular factors in rectal cancers with or without preoperative radiotherapy. Oncol Rep 16, 321–327 (2006).
Gnosa, S. et al. AEG-1 expression is an independent prognostic factor in rectal cancer patients with preoperative radiotherapy: a study in a Swedish clinical trial. Br J Cancer 111, 166–173 (2014).
Shabo, I., Olsson, H., Sun, X. F. & Svanvik, J. Expression of the macrophage antigen CD163 in rectal cancer cells is associated with early local recurrence and reduced survival time. Int J Cancer 125, 1826–1831 (2009).
Sun, X. F., Carstensen, J. M. & Nordenskjold, B. Expression of c-erbB-2 and p53 in colorectal adenocarcinoma. Anal Cell Pathol 8, 203–211 (1995).
Zhang, H. & Sun, X. F. Overexpression of cyclooxygenase-2 correlates with advanced stages of colorectal cancer. Am J Gastroenterol 97, 1037–1041 (2002).
Gao, J. et al. Clinical and biological significance of angiogenesis and lymphangiogenesis in colorectal cancer. Dig Liver Dis 41, 116–122 (2009).
Loftas, P. et al. Expression of FXYD-3 is an independent prognostic factor in rectal cancer patients with preoperative radiotherapy. Int J Radiat Oncol Biol Phys 75, 137–142 (2009).
Jansson, A. & Sun, X. F. Ki-67 expression in relation to clinicopathological variables and prognosis in colorectal adenocarcinomas. APMIS 105, 730–734 (1997).
Moparthi, S. B. et al. Expression of MAC30 protein is related to survival and biological variables in primary and metastatic colorectal cancers. Int J Oncol 30, 91–95 (2007).
Evertsson, S. & Sun, X. F. Protein expression of NF-kappaB in human colorectal adenocarcinoma. Int J Mol Med 10, 547–550 (2002).
Sun, X. F. p73 overexpression is a prognostic factor in patients with colorectal adenocarcinoma. Clin Cancer Res 8, 165–170 (2002).
Loof, J. et al. Impact of PINCH expression on survival in colorectal cancer patients. BMC Cancer 11, 103, 10.1186/1471-2407-11-103 (2011).
Yang, L. et al. Biological function and prognostic significance of peroxisome proliferator-activated receptor delta in rectal cancer. Clin Cancer Res 17, 3760–3770 (2011).
Sun, X. F., Ekberg, H., Zhang, H., Carstensen, J. M. & Nordenskjold, B. Overexpression of ras is an independent prognostic factor in colorectal adenocarcinoma. APMIS 106, 657–664 (1998).
Pathak, S. et al. Tafazzin protein expression is associated with tumorigenesis and radiation response in rectal cancer: a study of Swedish clinical trial on preoperative radiotherapy. PLoS One 9, e98317 (2014).
Evertson, S. et al. Microsatellite instability and MBD4 mutation in unselected colorectal cancer. Anticancer Res 23, 3569–3574 (2003).
Adell, G. C. et al. Apoptosis in rectal carcinoma: prognosis and recurrence after preoperative radiotherapy. Cancer 91, 1870–1875 (2001).
Franceschini, A. et al. STRING v9.1: protein-protein interaction networks, with increased coverage and integration. Nucleic Acids Res 41, D808–815 (2013).
Wang, J., Duncan, D., Shi, Z. & Zhang, B. WEB-based GEne SeT AnaLysis Toolkit (WebGestalt): update 2013. Nucleic Acids Res 41, W77–83 (2013).
Kanehisa, M. & Goto, S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic Acids Res 28, 27–30 (2000).
Acknowledgements
This work was supported by the grants from Swedish Cancer Foundation, Swedish Research Council and the Health Research Council in the South-East of Sweden and the National Scientific Foundation of China (Grant NO. 81401949, 8130035).
Author information
Authors and Affiliations
Contributions
M.J.W. and J.P. planned the research, wrote the manuscript and calculated statistics. G.A. and G.A. collected data. Y.L., Z.G.Z and X.F.S. supervised the entire project and helped to write the manuscript. B.N., W.J.M., H.Z., Y.Y.Y., C.W. and L.Y. provided technical and material support. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Wang, MJ., Ping, J., Li, Y. et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci Rep 5, 10645 (2015). https://doi.org/10.1038/srep10645
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep10645
This article is cited by
-
Log odds of positive lymph nodes show better predictive performance on the prognosis of early-onset colorectal cancer
International Journal of Colorectal Disease (2023)
-
Is early-onset cancer an emerging global epidemic? Current evidence and future implications
Nature Reviews Clinical Oncology (2022)
-
The role of PDGFRA as a therapeutic target in young colorectal cancer patients
Journal of Translational Medicine (2021)
-
Reconsideration of the optimal minimum lymph node count for young colon cancer patients: a population-based study
BMC Cancer (2018)
-
Alcohol consumption promotes colorectal carcinoma metastasis via a CCL5-induced and AMPK-pathway-mediated activation of autophagy
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
