
Abstract
Although erythromelalgia (EM) has been documented in the literature for almost 150 years, it is still poorly understood. To overcome this limitation, we examined the spatial distribution of epidemic EM and explored the association between temperature fluctuation and epidemic EM outbreaks in China. We searched all peer-reviewed literature on primary epidemic EM outbreaks in China. A two-stage model was used to characterize the relationship between temperature fluctuation and epidemic EM outbreaks. We observed that epidemic EM outbreaks were reported from 13 provinces during 1960–2014 and they mainly occurred between February and March in southern China. The majority of EM cases were middle school students, with a higher incidence rate in female and resident students. The major clinical characteristics of EM cases included burning, sharp, tingling and/or stinging pain in toes, soles and/or dorsum of feet, fever, erythema and swelling. A large “V”-shaped fluctuation of daily average temperature (TM) observed during the epidemic EM outbreaks was significantly associated with the number of daily EM cases (β = 1.22, 95%CI: 0.66 ~ 1.79), which indicated that this “V”-shaped fluctuation of TM probably triggered the epidemic EM outbreaks.
Similar content being viewed by others
Introduction
Erythromelalgia (EM) is characterized by a clinical syndrome of erythema, fever and associated discomfort, including burning pain, tingling, or similar sensations, preferentially involving the extremities brought on or aggravated by standing, walking or heat and relieved by the horizontal position and by cold1,2. EM was named by Weir Mitchell in 1878 based on his research results2. The first case of what became later known as EM was reported by the Irish physician Robert James Graves in 18343. Although EM has been documented in the literature for almost 150 years2, it is still poorly understood. A few recent studies demonstrated that EM patients had lower quality of life, higher risks of disability, mortality and morbidity1,4. For instance, Friberg et al. investigated the quality of life (QOL) among EM patients in New Zealand and found that they had significantly worse scores in the categories of physical function, bodily pain, general health, vitality, social function, emotional roles and mental health compared with healthy respondents1. Some severe EM patients have reported to systematically cool their feet in iced water for up to 20 hours a day to relieve the burning pain in their feet5.
EM occurs either as a primary or secondary disorder5,6. Secondary EM occurs in association with various conditions including small fibre peripheral neuropathy of any cause such as diabetes, or secondary to myeloproliferative diseases, mushroom poisoning, as a side effect of some medications or as a paraneoplastic syndrome4,7,8,9,10. Primary EM has no identifiable causes. A number of hypotheses have been proposed including vascular shunting11, neuropathic aetiologies12, microvascular aetiologies13 and inflammatory aetiologies14. Some researchers have found that SCN9A gene mutations might be associated with primary EM15.
To date, few studies have investigated the prevalence of EM in western countries. A study conducted in Norway estimated that the annual incidence was 2/100,0005. In a population-based study of EM in the USA, the reported annual incidence was 1.3/100,00016 and the overall annual population-based incidence of EM in Sweden was 0.36/100,00017. Although data on the prevalence of EM are very limited, it is proposed that EM may be more common than previously thought5. In China, Zhu reported the first clinical EM case in 194518 and the first epidemic EM event in 196019. Since then, at least 100 studies have reported more than 80,000 EM cases in China, of which most cases were primary epidemic EM patients20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37. For example, during February and March of 1990, a total of 11,589 epidemic EM cases were reported in 13 cities/counties of Hainan province and most of these cases were in middle school students24. In early 1987, 219 middle schools across 29 cities/counties of Hubei province reported a total of 19,278 epidemic EM cases and most of them were female students38. Between late February and early March of 2014, another epidemic EM outbreak with 494 cases was reported from two middle schools of Foshan city, Guangdong province, southern China. These reports suggest that epidemic EM is common in China, but the importance of this epidemic condition has not fully been recognized by international researchers due to language barrier39.
The etiology of epidemic EM outbreaks in China remains unclear. Some previous studies conducted in middle school students reported possible risk factors including heavy academic burden, poor living conditions and nutrition supply, menarche, poxviruses and climatic factors28,39,40. Some studies found that an epidemic EM outbreak often followed a large ambient temperature fluctuation between February and March hypothesizing that the sharp drop and subsequent rapid rising of ambient temperature possibly induced the dysfunction of peripheral vasodilation and hence induced the EM28,29,38. However, until now this hypothesized relationship between temperature and epidemic EM has not been tested quantitatively and some other questions about choice of temperature indicator (average temperature, maximum temperature, minimum temperature, or their corresponding apparent temperature) to best predict an EM outbreak have remained unanswered. Answering these questions will extend our understanding of the mechanisms of epidemic EM and provide important information for the control and prevention of this disease in the future.
In order to fill this knowledge gap, we searched all published papers from various databases that described epidemic EM in China and conducted a comprehensive analysis using data extracted from these papers. We aimed to understand the spatial distribution of epidemic EM and explore the association between temperature fluctuation and epidemic EM outbreaks in China.
Methods
Literature search
We searched all literature published between January 1st, 1956 and March 31st 2014 and indexed in MEDLINE, PubMed, China National Knowledge Infrastructure (CNKI), Wanfang, SinoMed and Chong Qing VIP (CQVIP) databases. The database searches used the following keywords: “erythromelalgia”, “erythermalgia”, “erythema”, “burning pain”, “increased temperature”, or “extremity”. We also manually searched other relevant references listed in published papers. Only peer-reviewed publications in English or Chinese were considered.
Inclusion and exclusion criteria
Because there is no laboratory test that can verify the diagnosis of EM, papers that employed the following inclusion criteria (symptoms and signs) to define an EM case were included in the potential relevant papers pool: burning extremity pain, pain aggravated by warming, pain relieved by cooling, erythema of affected skin and increased temperature of affected skin41. In order to demonstrate the spatial distribution of epidemic EM events in China, all the relevant papers which met the following criteria were included: (a) subjects must be primary epidemic EM cases; (b) time and location of study must be provided; and (c) the study location must be in China. Secondly, in order to summarize the temperature characteristics during an epidemic EM outbreak, papers that further met the additional following criteria were included: (d) must provide the exact beginning and end date of an epidemic EM outbreak. Finally, in order to assess the relationship between temperature fluctuation and number of daily EM cases, all the papers that met criteria (a) to (d) and also provided the daily number of epidemic EM cases were included. If multiple studies covering the same population were identified, the article with the most information was selected. Accordingly, papers that did not meet the above criteria were excluded. The process of study selection is presented in detail in Figure 1. In addition, we also included two reports that investigated the epidemic EM outbreaks in Shaoguan of 2009 and Foshan of 2014 in Guangdong province, China, respectively (See supplementary materials 1 and 2).

Flow chart of the study selection process.
Data extraction and collection
For each included paper which met criteria (a), (b) and (c), we extracted the following information: authors, year, source of publication, time and location of the epidemic EM outbreak. For studies which further met criteria (d), the exact date and prevalence of EM were added. For studies which met all the inclusion criteria, we also collected the number of daily EM cases and a range of daily temperature measures including mean temperature (TM), maximum temperature (Tmax), minimum temperature (Tmin), apparent TM, apparent Tmax and apparent Tmin. If the temperature data were not provided in the papers, we obtained it from the China Meteorological Administration for the city where the outbreak occurred.
All data extraction was carried out by two authors using a standard form and minor discrepancies were resolved by discussion. Apparent temperature indexes were calculated by the method provided by the Bureau of Meteorology, Australia (www.Bom.Gov.Au/info/thermal_stress).
Statistical analysis
Firstly, ArcGis (ArcMap 9.3, Environmental Systems Research Institute, Redlands, USA) technology was employed to describe the spatial distribution of epidemic EM events from 1950 to 2014 in China.
In order to explore which temperature index (mean temperature, maximum temperature, minimum temperature, or their corresponding apparent temperature) was the best predictor of EM outbreaks, we used a two-stage model to analyze the data from the twelve papers which reported the number of daily EM cases. In the first stage, a multiple linear regression model was used to estimate the association between different temperature indicators and number of daily EM cases in each paper. A partial regression coefficent (β) for a one degree Celsius increment and its standard error (SE) were reported. The analysis duration was restricted to the time of temperature rising in each study, because most studies found that the majority of EM cases occurred during the rising of temperature. In the second stage, a meta-analysis model was employed to estimate the summary β of different temperature indexes. The heterogeneity of the included studies was assessed using Cochran's Q statistic. If the heterogeneity test was significant, a random-effects model was used to estimate the pooled association between temperature indicators and daily EM cases. Otherwise, the estimated results based on a fixed-effects model were reported. The results indicated that mean temperature (TM) had the largest β with number of daily EM cases (Supplementary Figure 3). Therefore, all the analyses reported were conducted using TM.
To summarize the temperature characteristics during epidemic EM outbreaks, the TM and date were standardized. We firstly defined the beginning and end date of each EM outbreak. Then, the TM for each day was subtracted by the Tmin during each EM outbreak. The Tmin was defined as the lowest daily TMs during an EM outbreak days. The day with the Tmin was defined as “0”, the date before the “0” was defined as minus and the date after the “0” was defined as plus. For example, if the date of March 3rd was defined as the “0”, March 1st and March 5th would be defined as “−2” and “+2” day, respectively. Then we calculated the average standardized TM in each standardized date for all included papers. A line graph was used to reveal the fluctuation of standardized TM. In order to qualitatively assess the association between TM fluctuation and incidence rate of EM, we divided all 24 papers which reported the incidence rate of EM into three groups: group 1 (the incidence rates of EM were less than 10%), group 2 (the incidence rates of EM were between 10% and 20%) and group 3 (the incidence rates of EM were larger than 20%). The line graph of TM fluctuation vs date was respectively made for each group.
Finally, a multiple-line graph was used to explore the relationship between TM and number of daily EM cases in the twelve papers and the summary association was also reported based on the above two-stage model. In addition, we also conducted a sensitivity analysis to test the robustness of our findings, in which the study with the largest β, smallest β and both were respectively removed.
All statistical tests were two-tailed and p < 0.05 was considered statistically significant. We used R software (version 2.15.2; R Development Core Team 2012, www.R-project.org/) to analyze the data. The “Metafor” package was used to fit meta-analysis.
Results
Search results
A total of 73 papers reported outbreaks of epidemic EM in China and provided the study location. Of them, 46 papers provided the exact beginning and end date of epidemic EM outbreak, in which, 12 papers further provided the number of daily epidemic EM cases.
Epidemiological characteristics of epidemic EM
A total of 54 regions located in 13 provinces experienced epidemic EM outbreaks from 1960 to 2014. Most regions were located in the southern part of China (south of the Yellow River). Two large outbreaks occurred in 1987 and 1990. The 1987 outbreak happened in central provinces in China including Hubei, Hunan and Jiangxi provinces (near the middle part of the Yangtze River), while the 1990 outbreak was mainly in south China including Fujian, Guangdong and Hainan provinces (Figure 2).

The distribution of epidemic EM events in China.
Note: These maps were generated by ArcMap 9.3 software (Environmental Systems Research Institute, Redlands, USA).
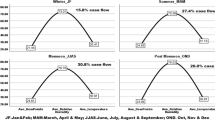
Almost all the epidemic EM events happened between February and March when ambient temperature experienced a large fluctuation. The EM cases included students, young labor workers, young medical workers and soldiers, but the majority were middle school students. Furthermore, the incidence rates of EM were higher for female students (22.6%) than male students (9.5%) and for resident students (24.5%) than non-resident students (9.4%).
Clinical characteristics of epidemic EM
The major clinical characteristics of EM cases included burning, sharp, tingling and/or stinging pain in toes, soles and/or dorsum of feet, increased temperature, erythema and swelling. Some cases reported burning pain in fingers, wrists and knees. These symptoms were more severe during the night, walking, standing, exercising and when the individual was near a heater. Patients could relieve their pains by rest, elevating feet, using cold packs, walking on cold floors, immersing feet in cold water, or sleeping with the affected part outside the quilts. Some patients used an electric fan to keep cooling their feet. These symptoms were reported as both sustained or paroxysmal. The duration of symptoms varied among cases with most cases lasting from minutes to hours, but in a few patients the symptoms continued for one to two days, or even years.
The characteristics of temperature during epidemic EM outbreaks
A “V”-shaped fluctuation of TM during epidemic EM outbreaks was observed in data obtained from 46 studies (Figure 3). The characteristics of the fluctuation were that firstly, the TM sharply and continuously dropped to a low level, usually lower than the minimum temperature during the same periods in neighboring years. The mean duration and decline rate of TM were 6.9 days and 2.2°C/day, respectively. Subsequently, TM rapidly increased to a high level. The mean duration and increment rate of TM for the entire epidemic event period were 12.5 days and 1.2°C/day respectively (Table 1). Most epidemic EM cases occurred during the TM increase period. After the TM became stable at a higher level, nil or very few EM cases were reported.

The standardized temperature during epidemic EM events.
Note: The standardized temperature was defined as the average temperature subtracted by the minimum temperature during each EM outbreak. The day with the minimum temperature was defined as “0” in the time axis, the date before the “0” was defined as minus and the date after the “0” was defined as plus. (A): Relationship between the temperature and time in all included articles. (B): Relationship between the temperature and time in articles with the incidence of EM less than 10.0%. (C): Relationship between the temperature and time in articles with the incidence of EM between 10.0% and 20.0%. (D): Relationship between the temperature and time in articles with the incidence of EM larger than 20.0%.
The 24 studies which reported the incidence rate of EM were divided into three groups and the number of studies were 10, 6 and 8, respectively. Compared with group 1, TM after time “0” rose slightly faster in group 2 and group 3 (Figure 3).
Associations between TM fluctuation and number of daily EM cases
Table 2 shows the characteristics of the 12 studies selected to analyze the associations between TM fluctuation and EM cases. The event occurred between February and March in all studies. These studies came from 6 provinces of southern China and included a total of 3,874 EM cases. Almost all cases in these studies were middle school students, except for one study which did not provide the details on occupation.
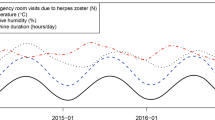
Figure 4 shows the relationship between standardized TM and the number of daily EM cases in the 12 studies. We observed that TM had a similar fluctuation with the daily number of EM cases after day “0”. A similar graph was drawn for each included study (Supplementary Figure 4). The results of meta-analysis show that the summary β of TM was 1.22 (95%CI: 0.66 ~ 1.79), which indicated that one degree Celsius increment was associated with an average increment of 1.22 cases (Figure 5).

The relationship between standardized temperature and number of daily EM cases.
Note: The standardized temperature was defined as the average temperature subtracted by the minimum temperature during each EM outbreak. The day with the minimum temperature was defined as “0” in the time axis, the date before the “0” was defined as minus and the date after the “origin” was defined as plus. The red line indicates the number of daily EM cases and blue line indicates the standardized TM.

Forest plot of the summary association between daily average temperature and number of daily EM cases.
Sensitivity analysis
Sensitivity analyses indicate that the results were robust to the estimation methods and to removing any single study (Figure 6).

Sensitivity analyses of meta-analysis methods on the association between daily average temperature and number of daily EM cases.
(A): Summary β was estimated in all included papers. (B): Summary β was estimated by removing the largest β. (D): Summary β was estimated by removing the smallest β. (D): Summary β was estimated by simultaneously removing the largest and smallest βs.
Discussion
Although erythromelalgia epidemics have been quite common in China, few studies from China have been reported in the international literature1. This study collected epidemic EM data from previously published papers in China to conduct a comprehensive analysis. We found that epidemic EM outbreaks were not rare in China, especially in southern China and the “V”-shaped fluctuation of TM between February and March was significantly associated with an epidemic EM outbreak.
The spatial distribution of epidemic EM cases show that most EM outbreaks occurred in southern China. This interesting spatial distribution may be related to the local climatic characteristics and inadequate adaptive capacity. During the late winter and early spring (February and March), temperature usually has a large fluctuation in China. For example, during mid-February in 1987, under the influence of El Nino, three episodes of cold air mass from Siberia moved into central China, which led to a sharp decline in temperature. The minimum temperature in some regions of Hubei province was 2°C lower than the average level in the same period of the past 34 years and temperatures dramatically declined by 17.8°C within 48 hours. This was closely followed by a warm air mass from the Pacific Ocean that caused the consequent rapid rising of temperature in this region38. This large fluctuation of temperature might cause thermoregulatory, automatic nerve and peripheral vascular contraction dysfunction and hence induced epidemic EM11,14,20. In northern China, the heating system could mitigate the effect of this temperature fluctuation on human health. However, in southern China, where cold weather is not common, heating systems are not common and this contributes to higher exposure to the varied ambient temperature42. In addition, populations in southern China have acclimatized well to the warm weather but it is possible that when exposed to the cold air mass, the rapid decline in temperature may exceed the range of their adaptive ability and potentially induce the thermoregulatory dysfunction20.
The majority of EM cases in this study were middle school students, particularly female and resident students. We suggest some possible reasons for this. Firstly, these students are in an age of rapid development and their automatic nervous and thermoregulatory systems are likely to be more sensitive to a large temperature fluctuation during a short period. In addition, they, especially resident students, often participate in less outdoor activities, have less emotional care from their families, poor accommodation and nutrition supply, factors which also increase their sensitivity to ambient temperature impacts43. However, it is unclear why female students were more vulnerable to EM. Some studies have postulated that it may be related to the relatively lower physical activities compared with males and endocrine hormone changes44. Research conducted in the future should explore the exact mechanisms of these differences between the sexes, such as mechanisms concerning immunity or heritage.
As there is no laboratory test that can verify the diagnosis of EM, all the previous cases were diagnosed based on clinical characteristics and symptoms3. This may lead to misclassification of other common diseases, such as chilblain. Chilblain is a localized disease which presents as inflammatory, erythematous or purple, intensely pruritic or painful acral lesions45. It is commonly seen in susceptible individuals after prolonged exposure to nonfreezing cold temperatures and damp conditions46. This disease is commonly seen in Chinese people, especially in young students from rural areas47. Although it has similar symptoms with EM, some remarkable symptoms, such as intensely pruritic and inflammatory that often attack the face, ears and dorsal side of hands and feet47, distinguish it easily from EM. More importantly, most chilblain cases occur during the rapid decline of ambient temperature and the peak of cases usually occurs near the lowest temperature48. By contrast, EM has some symptoms that are specific, such as pain aggravated by warming and relieved by cooling and in contrast EM usually occur during the rapid rising phase of ambient temperature.
We observed a common “V”-shaped fluctuation of TM during the epidemic EM outbreaks. We believe that this “V”-shaped fluctuation of temperature probably trigger the epidemic EM outbreak. During a sharp decline of temperature, it is likely that the acral small superficial arteries intensely constrict and dilate3, which induces the enhanced responses of these arteries to temperature. During the following rapid increase of temperature, the intense expansion of capillaries irritate the nerve endings around and thus lead to syndromes including burning pain, increased temperature, erythema and swelling11,14,20. In addition, we further quantitatively assessed the relationship between EM cases and different temperature indicators and found that TM, compared with Tmax, Tmin and their apparent temperatures, had the most pronounced association with EM cases. Some previous studies have also demonstrated that TM is a better predictor of mortality and morbidity fluctuation than Tmax and Tmin49, since TM represents an average exposure based on the whole day while Tmax and Tmin only reflect the exposure for a short period. These findings demonstrate that the pattern of ambient temperature fluctuation might be a pivotal predictor of epidemic EM and provide significant information on building up early warning system of epidemic EM especially for vulnerable populations like middle school female students.
Some limitations should be considered when interpreting our results. Firstly, the prevalence of epidemic EM may be underestimated in China because this syndrome is not monitored in routine disease surveillance system and few clinical doctors are aware of the diagnosis and treatment of EM. This may cause selection bias. Secondly, publication bias can not be avoided because most data in this study was obtained from the published papers. Thirdly, not all included papers reported the incidence rates of epidemic EM, which may induce information bias on the total estimated incidence of EM. Fourthly, due to the large variation of study periods and locations, we can not easily determine the threshold of temperature which triggered the outbreak of epidemic EM. Lastly, no study has reported epidemic EM outbreaks in other countries. It is not clear why this syndrome is specific in China and why it has association with climatic factors. More research should be conducted to fill these knowledge gaps.
Conclusions
Epidemic EM appears quite common in southern China. Middle school students, especially female and resident students appear to be the most vulnerable groups. The “V”-shaped fluctuation of daily average temperature during the late winter and early spring might trigger an epidemic EM outbreak. As climate change proceeds, more EM outbreaks may occur because extreme weather events are projected to increase in coming decades. We suggest that epidemic EM should be included in the current routine disease surveillance system and establish an early warning system of epidemic EM based on measured or projected temperature fluctuation in China.
References
Friberg, D., Chen, T., Tarr, G. & van Rij, A. Erythromelalgia? A clinical study of people who experience red, hot, painful feet in the community. Int J Vasc Med. 864961, 10.1155/2013/864961 (2013).
Brown, G. E. Erythromelalgia and other disturbances of the extremities accompanied by vasodilatation and burning. Am J Med Sci. 183, 468–484 (1932).
Kalgaard, O. M. Erythromelalgia: Clinical aspects, pathology and therapy. Dissertation for the degree of philosophiae doctor (Ph.D) at the University of Oslo, Norway. pp.63 (2012). Available at: www.duo.uio.no/bitstream/handle/10852/28041/dravhandling-kalgaard.pdf?sequence=2. (Accessed: 8th July 2014).
Davis, M. D., O'Fallon, W. M., Rogers, R. S., 3rd & Rooke, T. W. Natural history of erythromelalgia: presentation and outcome in 168 patients. Arch Dermatol. 136, 330–336 (2000).
Kalgaard, O. M., Seem, E. & Kvernebo, K. Erythromelalgia: a clinical study of 87 cases. J Intern Med. 242, 191–197 (1997).
Richard, R. B., Alarcon-Segovia, D. & Fairbairn, J. F. Erythermalgia review of 51 cases. Circulation. 29, 136–141 (1964).
Jeffcoate, W., Idris, I. & Game, F. Erythromelia, or mitchell's syndrome–new names for unexplained signs of inflammation in distal symmetrical neuropathy in diabetes. Diabetic Medicine. 21, 1334–1338 (2004)
Sunahara, J. F., Gora-Harper, M. L. & Nash, K. S. Possible erythromelalgia-like syndrome associated with nifedipine in a patient with raynaud's phenomenon. Ann Pharmacother. 30, 484–486 (1996).
Saviuc, P. F., et al. Erythromelalgia and mushroom poisoning. J Toxicol. 39, 403–407 (2001).
Kim, D.-H., Kim, C.-W. & Kim, T.-Y. Erythromelalgia as a paraneoplastic syndrome in a patient with abdominal cancer. Skin. 3, 441 (1980).
Mørk, C., Salerud, E. G., Asker, C. L. & Kvernebo, K. The prostaglandin E1 analog misoprostol reduces symptoms and microvascular arteriovenous shunting in erythromelalgia—A double-blind, crossover, placebo-compared study. J Invest Dermatol. 122, 587–593 (2004).
Ørstavik, K., Mørk, C., Kvernebo, K. & Jørum, E. Pain in primary erythromelalgia—a neuropathic component? Pain. 110, 531–538 (2004).
Mørk, C., Kvernebo, K., Asker, C. L. & Salerud, E. G. Reduced skin capillary density during attacks of erythromelalgia implies arteriovenous shunting as pathogenetic mechanism. J Invest Dermatol. 119, 949–953 (2002).
Michiels, J. J., Johannes, A., Steketee, J., Van Vliet, H. H. & Vuzevski, V. D. Erythromelalgia caused by platelet-mediated arteriolar inflammation and thrombosis in thrombocythemia. Ann Intern Med. 102, 466–471 (1985).
Yang, Y. et al. Mutations in scn9a, encoding a sodium channel alpha subunit, in patients with primary erythermalgia. J Med Genet. 41, 171–174 (2004).
Reed, K. B. & Davis, M. D. Incidence of erythromelalgia: A population-based study in olmsted county, minnesota. J Eur Acad Dermatol Venereol. 23, 13–15, 10.1111/j.1468-3083.2008.02938.x (2009).
Alhadad, A., Wollmer, P., Svensson, A. & Eriksson, K.-F. Erythromelalgia: Incidence and clinical experience in a single centre in sweden. Vasa. 41, 43–48 (2012).
Zhu, G. Erythromelalgia and its treatment by vitmin b. National Medical Journal of China. 31, 6 (1945).
Zhu, S. The epidemiological investigation and clinical analysis of the 433 erythromelalgia cases in guangzhou. National Medical Journal of China. 46, 365–367 (1960).
Wang, Q. X. & Li, Y. Relationship between meteorological conditions and epidemic erythromelalgia. Journal of Shandong Meteorology. 32, 47–50 (1988).
Liang, Y., Xu, G. N., Chen, H. H., Wei, T. Q. & Wang, L. M. An investigation report on the 116 erythromelalgia cases among middle school students. Chinese Journal of School Doctor. 3, 39–40 (1989).
Luo, G. S. et al. An epidemiologic investigation on the 296 epidemic erythromelalgia cases. Jiangxi Medical Journal. 22, 329–330 (1987).
Mo, Y. M. et al. An epidemiological study on erythromelagia. Medical Journal of Wuhan University. 8, 214–218 (1987).
Wang, C. Z. et al. An investigation on the epidemiological characteristics of epidemic erythromelalgia in hainan province. Hainan Medical Journal. 3, 40–44 (1992).
Liu, Y. & Duan, X. L. An epidemiological investigation on the epidemic erythromelalgia outbreak in a school. Journal of Preventive Medicine of Chinese People's Liberation Army. 7, 175–176 (1989).
Li, X. B. et al. An epidemiological invetigation on epidemic erythromelalgia outbreak. Journal of Xiangnan University (Medical Sciences). 13, 48–50 (2011).
Che, J. Y., Ruan, W. Y. & Pan, S. H. An epidemiological investigation and clinic analysis on the 198 erythromelalgia cases. Journal of Nanhua University(Medical Edition). 15, 261–264 (1987).
Shi, L. Y. et al. An epidemiological survey of epidemic melalgia in macheng hubei province. Acta Medicinae Universitatis Scientiae et Technologiae Huazhong. 18, 50–52 (1989).
Xu, F. H. Analysis of 78 primary erythromelalgia of chepu middle school puqi hubei china. Medical Journal of Wuhan University. 8, 224–228 (1987).
Dong, W. C., Li, Y. F. & Tang, X. Y. The clinical analysis on the 910 epidemic erythromelalgia cases. Guangxi Medical Journal. 11, 9–11 (1988).
He, J. X. et al. The epidemiological characteristics of epidemic erythromelalgia. Chinese Journal of Zoonoses. 11, 54–55 (1995).
Xie, F. G., Ning, H. W., Lei, Y. M. & Lei, S. B. An epidemiological investigation on an erythromelalgia outbreak. Practical Preventive Medicine. 17, 1922–1923 (2010).
Liu, X. & Li, X. J. An epidemiological analysis on the 242 erythromelalgia cases in two middle schools. Jun Dui Wei Sheng Za Zhi. 5, 50–52 (1987).
Chen, K. D. et al. An epidemiological investigation on an erythromelalgia outbreak in a high school of dangshan county. Chinese Journal of School Health. 15, 291–293 (1994).
Bi, L. H. An epidemiological investigation on the causes of erythromelalgia outbreaks in henan province. School Health. 8, 13–15 (1987).
Xie, Z. C. et al. An epidemiological investigation on an erythromelalgia outbreak. Guangdong Journal of Health and Epidemic Prevention. 17, 19–22 (1991).
Wang, R. H., Li, G. C., Han, K. Q. & Wang, X. H. An epidemiological investigation on the first outbreak of erythromelalgia in an national middle school of zhenning county. Gui Zhou Yi Yao. 16, 111–112 (1992).
Mo, Y. M. et al. The effect of el nino on epidemic erythromelalgia. Central China Medical Journal. 12, 116–117 (1988).
Zheng, Z., Zhang, J., Hu, J., Liu, S. & Zhu, W. Poxviruses isolated from epidemic erythromelalgia in china. The Lancet. 331, 296 (1988).
Zhu, W. F. & Zhao, Y. Z. A case-control study on epidemical erythromelagia. Chinese Journal of Epidemiology. 10, 94–97 (1989).
Mørk, C. & Kvernebo, K. Erythromelalgia—a mysterious condition? Arch Dermatol. 136, 406–409 (2000).
Xie, H. et al. Short-term effects of the 2008 cold spell on mortality in three subtropical cities in guangdong province, china. Environ Health Perspect. 121, 210–216 (2013).
Qun, L. Z., Mei, J. H., Hui, M. T., Dun, H. Z. & Xia, C. Epidemiological survey on an outbreak of erythromelalgia in a school. Practical Preventive Medicine. 18, 635–638 (2011).
Li, L., He, L. Z., Gai, Q. C., Xiu, B. & Ben, Z. C. Preliminary analysis on the 114 erythromelalgia cases. Henan Health and Epidemic Prevention. 3, 74–76 (1987).
Akkurt, Z. M., Ucmak, D., Yildiz, K., Yuruker, S. K. & Celik, H. O. Chilblains in turkey: A case-control study. An Bras Dermatol. 89, 44–50, 10.1590/abd1806-4841.20142376 (2014).
Raza, N., Habib, A., Razvi, S. K. & Dar, N. R. Constitutional and behavioral risk factors for chilblains: A case-control study from pakistan. Wilderness Environ Med. 21, 17–21 e11. 10.1016/j.wem.2009.12.023 (2010).
Yang, Z. J., Wang, Y. G. & Zhou, Z. G. An epidemiological investigation on the chilblain among the stduents in yimeng mountain area. Journal of Shandong Medical College. 23, 151–152 (2001).
Bi Ke, Z. et al. An epidemic of chilblains in rural boarding schools of a county,chongqing. Chin J Sch Health. 33, 317–319 (2012).
Guo, Y., Punnasiri, K. & Tong, S. Effects of temperature on mortality in chiang mai city, thailand: A time series study. Environmental Health. 11, 36, 10.1186/1476-069X-11-36 (2012).
Acknowledgements
This work was supported by the Natural Science Foundation of Guangdong Province (S2013010014670). This foundation greatly contributed in the process of data collection.
Author information
Authors and Affiliations
Contributions
T.L., Y.Z., X.L., H.L. and W.M. designed the study. T.L., X.L., J.X., W.Z. and Y.G. did the literature search and data collection. T.L. and X.L. managed and analyzed the data. T.L., S.T., S.R. and W.M. conducted the quality control, post-processing and oversight. All authors discussed and commented on the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Supplementary Information
Supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Liu, T., Zhang, Y., Lin, H. et al. A large temperature fluctuation may trigger an epidemic erythromelalgia outbreak in China. Sci Rep 5, 9525 (2015). https://doi.org/10.1038/srep09525
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep09525
This article is cited by
-
The trends of disease burden due to high temperature in Mainland China from 1990 to 2019 and its prediction to 2030
Scientific Reports (2023)
-
Using Baidu Search Engine to Monitor AIDS Epidemics Inform for Targeted intervention of HIV/AIDS in China
Scientific Reports (2019)
-
Early detection of an epidemic erythromelalgia outbreak using Baidu search data
Scientific Reports (2015)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
