
Abstract
This study aimed to quantify arterial volume distensibility in patients with branch retinal vein occlusion (BRVO) in comparison with normal subjects and to investigate factors associated with their differences. 40 normal subjects and 30 BRVO patients were studied. Brachial-ankle pulse wave velocity (baPWV) was measured to determine arterial volume distensibility. In comparison with the normal subjects, after adjusting for pulse pressure, baPWV in the BRVO patients was significantly higher by 2.3 m/s (P < 0.01) and arterial distensibility was significantly lower by 0.015% per mmHg (P < 0.01). No subject in the normal group had an arterial distensibility lower than 0.04% per mmHg, in comparison with 67% (20/30) in the BRVO group. Arterial distensibility was significantly related to systolic and diastolic blood pressures (SBP and DBP) and ageing for both groups (all P < 0.05), but in the BRVO group, blood pressures and ageing had more prominent effect on arterial volume distensibility. Peripheral arterial distensibility has been shown to be significantly lower in BRVO patients in comparison with normal subjects. The more prominent effect of SBP, DBP and ageing on arterial distensibility indicates the potential underlying mechanisms of the interaction between higher blood pressures, ageing and BRVO disease.
Similar content being viewed by others

Introduction
Arteries, arterioles and capillaries play important roles in cardiovascular physiology and pathophysiology. The peripheral arteries and arterioles in the microcirculation are the primary sites of vascular resistance and therefore the primary site for regulation of blood pressure and blood flow. However, the pathogenesis of decreased arterial elasticity is still clinically uncertain1. A loss of arterial elastic properties has been considered intrinsic to the ageing process of the arterial wall2 and also been associated with other different clinical and physiological factors, such as hypertension, heart failure, diabetes, smoking and alcohol3,4,5,6,7. Microvascular processes may also contribute to the loss of arterial elasticity8. More recently, it has been accepted that the elastic properties of arteries can provide an early marker of risk for cardiovascular disease9 and is an independent predictor of cardiovascular mortality10.
Patients with advanced retinal vascular disease have higher risks of cardiac and peripheral vascular diseases11,12. Branch retinal vein occlusion (BRVO) is a very common retinal vascular disease and a major cause of vision loss, affecting approximately 16 million people worldwide13. Therefore, a better understanding of the changing elastic properties of arteries in patients with BRVO is of pathophysiological importance. Although aortic stiffening has been observed in patients with retinal microvascular disease14, to the best of our knowledge, there is no information available on how the peripheral arterial properties change in patients with BRVO.
Various assessment techniques have been developed to non-invasively quantify the peripheral arterial properties15. Pulse wave velocity (PWV) is one of the most commonly used indirect techniques16. In practice, PWV is often calculated from the pulse transmission time over two superficial artery sites with known distance. The stiffer or less elastic the artery is, the higher the velocity of arterial pulse transmission. Arterial volume distensibility, giving the relative change in blood volume with a known change in arterial pressure, is a direct quantification of the elastic and hence structural properties of the arterial wall17. Typically, it is calculated from the measurement of the percentage change in arterial diameter within each cardiac cycle using ultrasound technique15. However, ultrasound technique is highly operator-dependent with large errors in the measurement of artery size, especially with small and medium sized peripheral arteries. Recently, Zheng and Murray reported a simple measurement technique to obtain the peripheral arterial volume distensibility from PWV17. Because of its simplicity, its application to BRVO patients is worth further investigation.
The aim of this study was to quantify arterial volume distensibility of peripheral arteries in patients with BRVO by measuring peripheral PWV and to compare with measurements from normal subjects. The factors influencing peripheral arterial volume distensibility in BRVO patients were also investigated.
Methods
Subjects
Sample size required for clinical trials of the PWV measurement has been reported by Liang et al18. With a reference coefficient of variation of 10%, 30 subjects were enough to achieve a confidence level of 95% and a statistical power of 80%. In this study, 40 normal subjects and 30 BRVO patients were studied. They were matched by age between 36 and 70 years. The study obtained full approval of the Local Clinical Ethics Committee of the Second Affiliated Hospital of Zhejiang University. The investigation conformed to the principles in the Declaration of Helsinki. All subjects gave their written informed consent to participate in the study and confirmed that they had not have participated in any other clinical trials within the previous three months.
Diagnosis of branch retinal vein occlusion (BRVO)
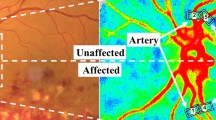
All BRVO patients had eye disease history between 3 to 6 months before they presented for their first eye examination at the Eye Center of Second Affiliated Hospital of Zhejiang University. Patients with previous history of diabetes mellitus and coronary heart disease were excluded. Each patient was initially examined by a consultant ophthalmologist using a fundoscopy, following by a further examination performed on the same day by a retinal specialist using fundus fluorescein angiography (FFA, Heidelberg Engineering Inc., Germany). The diagnosis of BRVO was made by fundus examination by finding retinal hemorrhages in the distribution of an obstructed retinal vein. FFA was used to confirm the diagnosis and determine the degree of retinal ischemia and diagnose macular edema according to the diagnostic criteria summarized by Jaulim et al19. The final diagnosis of BRVO was agreed between the two ophthalmologists. In addition, four biochemical indices, including blood glucose, total cholesterol, triglyceride and low density lipoprotein (LDL), were also tested for each patient.
Brachial-ankle pulse wave velocity (baPWV) measurement
Brachial-ankle PWV measurements were performed immediately after the eye examinations in a quiet, temperature controlled examination measurement room (25°C) at the Second Affiliated Hospital of Zhejiang University. All the PWV measurements were done by one experienced technician. Before formal recording, each subject lay supine on a measurement bed for 10 min to allow cardiovascular stabilization. At the beginning and end of the baPWV measurements, manual auscultatory systolic and diastolic blood pressures and pulse pressure (SBP, DBP and PP) were recorded. During the whole measurement, subjects were asked to breathe regularly and gently.
A VP 1000 automated PWV/ABI analyzer VP1000 (PWV/ABI, Colin Co. Ltd., Komaki, Japan) was used to simultaneously record pulse waveforms of the brachial and posterior tibial arteries based on an automated oscillometric method. The bilateral values of ankle-brachial index (ABI) and baPWV were obtained. The validation of the VP1000 device and its reproducibility has been previously published16.
Peripheral arterial volume distensibility calculation
With the recorded baPWV, the arterial volume distensibility from both the left and right sides were calculated using the method proposed by Zheng and Murray17. The detailed process is summarized as follows:
From the definition of arterial volume distensibility (Distensibility = (ΔV/V)/ΔP, where ΔV is the change in blood volume in each cardiac cycle and ΔP is pulse pressure) and the Bramwell and Hill equation ( , where ρ is blood density = 1025 kg · m−3), peripheral arterial volume distensibility was then derived as follows20:
, where ρ is blood density = 1025 kg · m−3), peripheral arterial volume distensibility was then derived as follows20:

and then  .
.
Data and statistical analysis
The overall means and SDs of ABI, bilateral baPWVs and arterial volume distensibilities were obtained, separately for the normal subjects and BRVO patients. Next, their differences between the left and right sides were compared, as well as their differences between the two groups after the adjustment for PP. Finally, multiple regression analysis was performed to determine the effect of SBP, DBP, age, sex, height, weight, smoking, body mass index (BMI), heart rate and the four biochemical indices on baPWV and arterial volume distensibility, with the correlation coefficient R-value and P-value obtained. SPSS 19.0 software package (SPSS Inc.) was used for the statistical analysis and a value of P < 0.05 was considered statistically significant.
Results
Physiological characteristic information
The subject demographic information is summarized in Table 1. For all the manual blood pressures (SBP, DBP and PP), there was no significant differences between the measurements taken at the beginning and end of the baPWV measurement (all P > 0.05). The average SBP, DBP and PP from the two measurements were used as the reference blood pressures for that subject. As expected, there was a significant difference in blood pressures (SBP, DBP and PP, all P < 0.01) between the normal and BRVO groups. The measured blood glucose and total cholesterol from over 90% of the subjects were within the normal range of 3.89–6.11 mmol/L and 3.10–6.0 mmol/L, respectively. Blood glucose and LDL had significant differences between the two groups (both P < 0.05), but not for age, gender, weight, smoking, total cholesterol and triglyceride (all P > 0.05).
Differences of ABI, baPWV and arterial volume distensibility between the two groups
Table 2 gives the overall means and SDs of ABI, baPWV and arterial volume distensibility from the two groups. All parameters had no significant differences between the left and right sides (P > 0.05). Their average values from the left and right sides of each subject were then used as reference values for that subject.
As shown in Figure 1 and Table 2, before the adjustment for PP, there was no significant difference in ABI between the two groups (P > 0.05). baPWV in the BRVO group was significantly higher by 3.0 m/s (15.7 ± 2.6 vs 12.7 ± 0.9 m/s, P < 0.01) and arterial volume distensibility was significantly lower by 0.02% per mmHg (0.04 ± 0.02 vs 0.06 ± 0.01% per mmHg, P < 0.01). After the adjustment for PP, baPWV in the BRVO group was still significantly higher by 2.3 m/s and arterial volume distensibility significantly lower by 0.015% per mmHg (both P < 0.01). No subject in the normal group had an arterial distensibility lower than 0.04% per mmHg, in comparison with 67% (20/30) in the BRVO group.

Box-plots of brachial-ankle pulse wave velocity (baPWV) (A) and arterial volume distensibility (B) for the normal and BRVO groups. ‘*’ means statistically significant between the normal and BRVO groups after adjusting for pulse pressure.
Effect of blood pressures and ageing on baPWV and arterial volume distensibility
Multiple regression analysis showed that both baPWV and arterial volume distensibility were significantly related to SBP, DBP and age for both the normal and BRVO groups, but they had no relationship with other physiological characteristics (including sex, height, weight, smoking, BMI, heart rate, blood glucose, total cholesterol, triglyceride and LDL) for both groups.
As given in Figure 2–3 and Table 3–4, both baPWV and arterial volume distensibilty had significant relationships with SBP and DBP in both normal and BRVO groups (all P < 0.05). It has also been shown that their absolute regression slopes increased in BRVO group. As demonstrated in Table 3 and 4, in the normal group, baPWV increased by 17% for a SBP increase from 90 to 150 mmHg and 21% for a DBP increase from 45 to 105 mmHg. These increases were more than double in the BRVO group (37% against 17% for SBP and 48% against 21% for DBP). For the same blood pressure increase, more obvious decrease in arterial volume distensibility was obtained in the BRVO group in comparison with the normal group (38% against 30% for SBP and 56% against 36% for DBP).

Brachial-ankle pulse wave velocity (baPWV) as a function of systolic blood pressure (SBP), diastolic blood pressure (DBP) and age for the normal (A1–A3) and BRVO groups (B1–B3).
The regression lines with P values and R values are also shown.

Arterial volume distensibility as a function of systolic blood pressure (SBP), diastolic blood pressure (DBP) and age for the normal (A1–A3) and BRVO groups (B1–B3).
The regression lines with P values and R values are also shown.
Regarding the effect of ageing on both baPWV and arterial volume distensibility, there were significant relationships in the two groups (both P < 0.05). As demonstrated in Table 3 and 4, in the normal group, baPWV increased by 11% and arterial volume distensibility decreased by 18% for an age increase from 45 to 65 year old, but their decrease was nearly double in the BRVO group (22% against 11% for baPWV and 35% against 18% for arterial distensibility).
Discussion
This study has demonstrated that, after adjusting for PP, peripheral arterial volume distensibility was significantly lower in BRVO patients by simply measuring peripheral baPWV. It is clinically useful to have a simple measurement technique to assess arterial elastic properties. Several non-invasive techniques have been reported, but most of them are indirect measurements by assessing factors influenced by arterial properties15. The ultrasound technique has been used to directly measure arterial distensibility of medium-sized arteries21,22. However, the ultrasound technique for arterial distensibility measurement has not been accepted in real clinical use due to the disadvantage of large variability in measuring the diameter of medium or small-sized arteries. The non-invasive method (baPWV) employed in this study to obtain peripheral arterial volume distensibility from baPWV is much simpler and its application to measure the differences in elastic properties of peripheral arteries between normal subjects and heart failure patients has been investigated3. In this study, its potential to measure arterial volume distensibility differences between normal subjects and BRVO patients has been demonstrated, suggesting that baPWV could be a useful technique in assessing BRVO patients.
Our results also showed that arterial volume distensibility is significantly and inversely related to SBP and DBP for both normal subjects and BRVO patients, but not to the biochemical parameters (blood glucose, total cholesterol, triglyceride and LDL). The inverse relationship between arterial distensibility and blood pressures was more pronounced in BRVO patients. This indicates that high blood pressure could be an important factor associated with low arterial volume distensibility in BRVO patients and confirms that hypertension is one of the main factors contributing to the pathophysiology of BRVO.
The effect of ageing on arterial volume distensibility is clinically controversial, especially for peripheral medium-sized arteries23,24. Since baPWV includes peripheral components of the arterial tree, its potential use in clinical research study and for screening vascular disease has been demonstrated16. Our results in normal subjects indicate that the systemic volume distensibility of the peripheral artery calculated from baPWV had statistical relationship with age, which agreed with the published validation study25. However, the ageing effect on baPWV and arterial volume distensibility in BRVO patients has not been well investigated. To the best of our knowledge this is the first study to demonstrate the ageing effect in BRVO patients. We have shown that ageing had prominent effect on baPWV and arterial volume distensibility in BRVO patients in comparison with normal subjects, suggesting the potential underlying mechanisms of the interaction between ageing and BRVO disease. In patients with BRVO, ageing could enhance structural and functional abnormalities of arterial wall and degeneration or disorganization of the medial layer, leading to measurably increased baPWV and decreased distensibility. Nevertheless, further investigation is still required to better understand the underlying mechanism for the changes of arterial elastic properties in BRVO patients.
One of the limitations of this study is that the BRVO patients were uncontrolled hypertensive patients with anti-hypertensive medication. However, all the arterial pulse measurements were performed immediately after the eye examinations. Blood pressures at the beginning and end of the PWV measurement were measured by the gold standard manual auscultatory method and there were no significant differences at the two timing points. This indicates that the cardiovascular hemodynamics was stable during the study and also confirms that using the average blood pressures from the two measurements as a reference blood pressure to investigate its relationship with PWV is acceptable. Secondly, only BRVO patients were studied in this preliminary investigation partly because the risk factors associated with the development of BRVO are much simpler than these for the central retinal vein occlusion (CRVO). In addition, the site of occlusion in BRVO is usually at arteriovenous crossings. Therefore the effect of pathophysiologic changes of arteries on retinal veins could be more obvious and direct at the junctions. The investigation with CRVO patients, as well as the comparison with BRVO patients, could be our future work. Furthermore, the comparison of micro- and macro-vascular function/structure markers and the relationship between microvascular abnormalities and cardiovascular parameters in patients with other retinal vascular diseases are also worth investigation.
Conclusion
The current study demonstrated that BRVO patients had higher baPWV and lower peripheral arterial volume distensibility in comparison with normal subjects. It has also been demonstrated that, in patients with BRVO, blood pressures and ageing had more prominent effect on baPWV and arterial volume distensibility. These findings are clinically and pathophysiologically important and have made an important contribution in understanding the underlying mechanism for the changes of arterial elastic properties in BRVO patients.
References
Liao, D. et al. Relationship between carotid artery stiffness and retinal arteriolar narrowing in healthy middle-aged persons. Stroke 35, 837–842 (2004).
Hodes, R. J., Lakatta, E. G. & McNeil, C. T. Another modifiable risk factor for cardiovascular disease? Some evidence points to arterial stiffness. J Am Geriatr Soc 43, 581–582 (1995).
Liu, C. et al. Elastic properties of peripheral arteries in heart failure patients in comparison with normal subjects. J Physiol Sci 63, 195–201 (2013).
Mahmud, A. & Feely, J. Divergent effect of acute and chronic alcohol on arterial stiffness. Am J Hypertens 15, 240–243 (2002).
Beneto, A. et al. Influence of age, risk factors and cardiovascular and renal disease on arterial stiffness: clinical applications. Am J Hypertens 15, 1101–1108 (2002).
Arnett, D. K. et al. Hypertension and arterial stiffness: the Atherosclerosis Risk in Communities Study. ARIC Investigators. Am J Hypertens 13, 317–323 (2000).
Failla, M. et al. Effects of cigarette smoking on carotid and radial artery distensibility. J Hypertens 15, 1659–1664 (1997).
Angouras, D. et al. Effect of impaired vasa vasorum flow on the structure and mechanics of the thoracic aorta: implications for the pathogenesis of aortic dissection. Eur J Cardiothorac Surg 17, 468–473 (2000).
Mattace-Raso, F. U. et al. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation 113, 657–663 (2006).
Mitchell, G. F. et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation 121, 505–511 (2010).
Chapman, N. et al. Peripheral vascular disease is associated with abnormal arteriolar diameter relationships at bifurcations in the human retina. Clin Sci (Lond) 103, 111–116 (2002).
Wong, T. Y. et al. Retinal microvascular abnormalities and their relationship with hypertension, cardiovascular disease and mortality. Surv Ophthalmol 46, 59–80 (2001).
Rogers, S. et al. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia and Australia. Ophthalmology 117, 313–319 (2010).
Theilade, S., Lajer, M., Persson, F., Joergensen, C. & Rossing, P. Arterial stiffness is associated with cardiovascular, renal, retinal and autonomic disease in type 1 diabetes. Diabetes care 36, 715–721 (2013).
McVeigh, G. E., Hamilton, P. K. & Morgan, D. R. Evaluation of mechanical arterial properties: clinical, experimental and therapeutic aspects. Clin Sci (Lond) 102, 51–67 (2002).
Yamashina, A. et al. Validity, reproducibility and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens Res 25, 359–364 (2002).
Zheng, D. & Murray, A. Peripheral arterial volume distensibility: significant differences with age and blood pressure measured using an applied external pressure. Physiol Meas 32, 499–512 (2011).
Liang, Y. L. et al. Non-invasive measurements of arterial structure and function: repeatability, interrelationships and trial sample size. Clin Sci (Lond) 95, 669–679 (1998).
Jaulim, A., Ahmed, B., Khanam, T. & Chatziralli, P. Branch retinal vein occlusion: epidemiology, pathogenesis, risk factors, clinical features, diagnosis and complications. An update of the literature. Retina 33, 901–910 (2013).
Nichols, W., O'Rourke, M. & Vlachopoulos, C. McDonald's blood flow in arteries: Theoretical, experimental and clinical principles. Sixth Edition. CRC Press, (2011).
MacWilliams, B. A., Hoffman, A. H. & Savilonis, B. J. Variation of arterial compliance within the cardiac pressure pulse. J Biomechanics 31, 867–871 (1998).
Girerd, X. et al. Noninvasive measurement of medium-sized artery intima-media thickness in humans: in vitro validation. J Vasc Res 31, 114–120 (1994).
Bjarnegård, N. & Länne, T. Arterial properties along the upper arm in humans: age-related effects and the consequence of anatomical location. J Appl Physiol 108, 34–38 (2010).
Van Der Heijden-Spek, J. J. et al. Effect of age on brachial artery wall properties differs from the aorta and is gender dependent: a population study. Hypertension 35, 637–642 (2000).
Tomiyama, H. et al. Influences of age and gender on results of noninvasive brachial-ankle pulse wave velocity measurement--a survey of 12517 subjects. Atherosclerosis 166, 303–309 (2003).
Acknowledgements
This project is supported by the Public Welfare Technology Project of Science Technology Department of Zhejiang Province under Grant 2012C23068, Zhejiang Province Medical Platform Program under Grant 2013RCB008, the National Natural Science Foundation of China under Grant 61201049 and the Excellent Young Scientist Awarded Foundation of Shandong Province in China under Grant BS2013DX029. Dingchang Zheng and Chengyu Liu were funded by the Engineering and Physical Sciences Research Council (EPSRC) Healthcare Partnership Award (reference number EP/I027270/1).
Author information
Authors and Affiliations
Contributions
D.Z. and Z.C. designed the study. Z.C. and L.M. collected the data. Z.C., L.M., C.L., J.R.B. and D.Z. performed the data and statistical analyses, interpreted the results and drafted and reviewed the manuscript. Z.C. and C.L. obtained the funding for this study.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Chen, Z., Mao, L., Liu, C. et al. Decreased peripheral arterial volume distensibility in patients with branch retinal vein occlusion in comparison with normal subjects. Sci Rep 4, 6685 (2014). https://doi.org/10.1038/srep06685
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep06685
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
