
Key Points
-
Provides readers with a understanding of bleaching legislation in the United Kingdom.
-
Provide readers with an understanding of discolourations aetiology and management.
-
Provides readers with an understanding regarding bleaching protocols for adolescent patients.
-
Provides readers with key understandings of core bleaching concepts.
Abstract
Following changes in the EU regulations, it became legal for bleaching to be undertaken by dentists and their trained team. However, restrictions remained on bleaching for patients under the age of 18. A revised position statement by the General Dental Council (GDC) determined that bleaching could be undertaken on these patients if it was wholly for the purpose of treating or preventing disease. The purpose of this paper is to discuss the safety, efficacy, indications and techniques for under-18 bleaching.
Similar content being viewed by others


Introduction
Following the 2012 Cosmetic Products Safety Amendment Regulations, it became legal for tooth whitening to be undertaken by dentists and their trained teams (dental therapist and dental hygienist) using tooth whitening material containing less than 6% hydrogen peroxide.1,2 However, restriction on under-18 bleaching remained, limiting the use of whitening treatment for this group of patients to less than 0.1% hydrogen peroxide. This placed dentists in a precarious situation, with regards to clinical situations whereby bleaching was indicated, however, legally could not be provided.
Ethically, these clinical dilemmas were only heightened by the knowledge that more invasive, direct and indirect restorations were permitted. No restoration is 100% successful. Crowned teeth may lose vitality in 19% of patients3 and this may be more significant for adolescent patients due to the larger pulp complexes. Even the less destructive treatment modality of ceramic veneers has a finite life span, with a systematic review by Petridis et al.4 noting that the most frequent complication of the restoration being marginal discolouration (9% at five years), followed by loss of marginal integrity (3.9–7.7%) at five years. The significance of these failures is also compounded by the younger age of these patients. Should a dentist introduce these young adolescent patients into the restorative cycle, simply to comply with EU/UK regulations, even though bleaching would be a more appropriate, less invasive and a less damaging treatment modality?
Thankfully, after lobbying from the British Dental Bleaching Society (BDBS) and the British Society of Paediatric Dentistry (BSPD), a revised position statement on the General Dental Council's (GDC) website was released stating: 'Products containing or releasing between 0.1% and 6% hydrogen peroxide cannot be used on any person under 18 years of age except where such use is intended wholly for the purpose of treating or preventing disease.'5
Despite this, many have argued that legal advice should be sought from indemnity providers before undertaking bleaching treatment on such patients. However, correctly identifying and appropriately treating disease fall well into the scope and everyday practice of general dentistry and as such is not necessary.
Further questions remain with regards to the safety, efficacy and clinical technique required for under-18-year-old bleaching. Furthermore, elaboration on the exact clinical indications covered by the GDC position statement were required. This article will aim to provide an evidence-based response to the unanswered questions on the topic.
Safety of bleaching in adolescent patients
Carbamide peroxide (CP), also known as urea peroxide, was initially used as an oral antiseptic agent and cleanser. In 1964, Benjamin Dickstein reported using CP to treat neonatal oral candidiasis.6 Other earlier studies demonstrated CP's effectiveness on plaque control and gingival inflammation.7,8,9 In 1968, it was this use as an oral antiseptic which led to the incidental discovery of bleaching by Dr Bill Klusmeier.10
Nowadays, there is much research to support the safety of bleaching,11,12,13,14 however, most of this research was conducted on adults and less on the adolescent patient. In 2005, the European Commission Scientific Committee on Consumer Products concluded that 'The proper use of tooth whitening products containing 0.1 to 6.0% hydrogen peroxide is considered safe after consultation with and approval of the consumer's dentist.'15
One concern commonly raised regarding bleaching in the adolescent patient, is the risk of tooth sensitivity. Tooth sensitivity in adults during bleaching treatment is common, and has been reported between 15–65%.16,17,18,19 Sensitivity is related to the easy passage of hydrogen peroxide through intact enamel and dentin (reaching the pulp in five to 15 minutes)20 and to the bleaching tray, which causes sensitivity in 20% of patients.21
It has been hypothesised that due to the proportionally larger pulp complexes in the adolescent patient, tooth sensitivity would be more prevalent during bleaching treatment.
However, many clinical studies have demonstrated that this is not the case.
Bacaksiz et al.22 revealed that in-office bleaching using hydrogen peroxide at high concentrations (25% and 36%) could be undertaken safely on the adolescent patient. Furthermore, several randomised control trials by Donly have shown that tooth sensitivity was relatively minor in adolescent patients in comparison to reported sensitivity among adult patients,23,24,25,26,27 despite greater than normal hydrogen peroxide concentrations being used (6.5%, 9%, 10%). This could be attributed to the increased enamel quantity and quality of the adolescent teeth and also to the larger pulp complexes in adolescent patients' teeth which allow faster recovery from the acute inflammation experienced during a sensitivity episode.27 Importantly, the sensitivity experienced by the under-18 patients is manageable and does not deter them from completing the tooth whitening treatment.12
Gingival irritation is another reported side-effect associated with adolescent treatment.23,24,25,26,27 Gingival irritation is more common in higher concentrations of bleaching products and may be more common among strip-applied bleaching agent in comparison to tray-applied.28 For most patients, gingival irritation is tolerable and is not a barrier to completing the treatment. An ill-fitting tray is usually the primary cause for the irritation and the problem is usually resolved by relieving overextensions of the tray. Furthermore, failure to wipe away excess whitening product may result in gingival irritation and therefore it is essential that this is clearly explained to the patient and their supervising parent on delivery of the tray.13
Effectiveness of under-18 bleaching
Significant bleaching effects following treatment have been repeatedly demonstrated when compared to baselines in clinical trials.23,24,25,26,27 There have been some suggestions that the bleaching success and rate of bleaching may be increased in the adolescent patient, when compared to the adult patient. This may be due to the increased permeability of the dentine and enamel and the diffusion flux experienced due to the anatomy of the younger enamel structure, which is more porous and permeable.29 The young teeth have also had less time in the mouth to acquire stains or deposit secondary dentin. There may also be improved compliance resulting from social pressures experienced in the adolescent age group, however, there is currently no research on this theory.
Indications for bleaching in children and the adolescent patients
The GDC guidance mentioned previously states that products containing or releasing 0.1–6% hydrogen peroxide can be used in under-18 patients, only 'for the purpose of treating or preventing disease'.4 Guidance on the indications and conditions for adolescent bleaching have been listed in Box 1.
Some may suggest that discolouration may not fall under the classification of disease, however, it is prudent to understand the psychological and psychosocial effects associated with discolouration30,31 and the emotional effect on a child resulting from delayed treatment of the discolouration.32 Negative self-image due to a discoloured tooth or teeth can have serious consequences on adolescents. As such, treating discolouration and disease may aid in prevention of bullying and associated or resulting mental health conditions such as depression and suicide.33 Furthermore underlying enamel quality or quantity defects commonly associated with the discolouration also renders the classification of disease appropriate.
It is essential that all treatment options are provided to the patient and parents seeking dental bleaching, including the option of no treatment. All risks and benefits associated with bleaching must also be discussed before commencing treatment and consent appropriately obtained. It should be expressed that further restorative treatment may be required post bleaching, for example microabrasion, resin infiltration and composite bonding where large enamel surface defects exist.12,34
Various factors relevant to the patient's discolourations must be considered when determining the need and urgency for bleaching in the under-18 patients. Some of these are listed in Box 2.
Detailed history taking, initial examinations and appropriate radiographs are essential for accurate diagnosis, treatment planning and identification of risk factors and oral pathology. It is essential to identify any restorations in the aesthetic zone and explain to the patient that post bleaching these may no longer be a matching shade and thus are likely to require replacement.35
Furthermore, discolouration, particularly intrinsic stains, may not simply be an aesthetic problem and bleaching may not be the appropriate or the best choice for treatment.14 This will be discussed later in the article.
Bleaching treatment for the adolescent patient and patient groups is listed in Box 1.
Severe and moderate discolouration
As discussed previously, the psychosocial effects of discolourations can be extreme. Severe discolouration can result from numerous aetiologies, including but not limited to:
-
Fluorosis (Figs 1, 2 and 3)
Figure 1: a) Labial view of severely discoloured maxillary central incisors. 
b) Labial view of the incisors following three weeks of bleaching. c) Labial view of maxillary incisors following ten weeks of bleaching
-
Discoloration caused by antibiotics or resulting from a child's complex medical history (Fig. 4).
Figure 2: a) Labial view of teeth in occlusion demonstrating fluorosis discolouration of the dentition and existing composite restorations. 
b) Labial view of teeth in occlusion following successful treatment with bleaching and composite replacement
Figure 3: Labial view of teeth demonstrating fluorosis discolouration of the dentition. 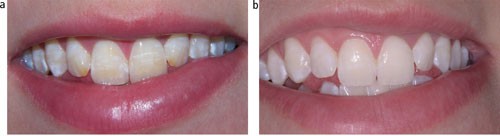
b) Labial view of the result post bleaching and microabrasion treatment
Figure 4: A labial view of central incisors presenting with white markings along the perikymata. 
This was believed to have resulted from amoxicillin which was administered to the child at a young age




Fluorosis can be effectively bleached, as shown in Figures 1, 2 and 3. Bleaching is most effective in class 1 to 3 of the tooth surface index of fluorosis and as such alternative treatment may be required for patients with severe flurorosis.36
Severe discolouration may require prolonged bleaching.14 This can be seen in Figures 1a and 1b, whereby after three weeks of bleaching treatment, the brown discolouration had reduced, however, had not completely resolved. Bleaching treatment was prolonged for an additional seven weeks and this eventually resulted in complete resolution of the brown discolouration (Fig. 1c). The patient was delighted with the final result, despite the presence of the white lesions and as such chose no further treatment.
Enamel conditions
A range of enamel conditions result in discolouration and can be effectively treated with bleaching. These include but are not limited to:
-
Amelogenesis imperfecta (see hereditary section)
-
Post traumatic opacities
-
Idiopathic opacities
-
Chronological hypomineralisation
-
White markings or puffs on the lines of enamel maturation.
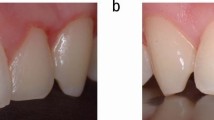
White lesions
White spot lesions have numerous aetiologies.37 Some markings are chronologic in nature and appear as white lines that follow deposition of enamel such as amoxicillin or high temperature defects38 which are shown in Figure 4. Bleaching treatment whitens the surrounding or background enamel of the white lesion, which reduces the contrast of the defect as demonstrated in Figure 5b. It has also been suggested that elevation of salivary Ph and flow rates following carbamide peroxide application39 may alter the refractive index of the white spot by promoting remineralisation, however, further research is required.

b) Labial view of the maxillary incisors following bleaching and use of resin infiltration
Isolated white blemishes (Fig. 5a), can be aesthetically challenging for the young child and tooth bleaching or whitening is a simple way to eradicate these unsightly markings on the teeth. This may need to be followed by microabrasion or resin infiltration. In the patient illustrated in Figures 5a and b, a combination of bleaching using custom tray-applied 10% carbamide peroxide followed by resin infiltration was used to successfully to eradicate the white blemishes on the central incisors (Fig. 5b).
Original white spots may become more noticeable during bleaching treatment, as seen in Figure 1c. This is due to the bleaching material penetrating the weakest part of the enamel first, which is often the white spot. This commonly occurs during the first few days and is referred to as the 'splotchy stage' of bleaching.40 The patient must be urged to persevere with the bleaching treatment to allow time for the bleaching material to dissipate equally throughout the enamel and allow efficient lightening of the background. The 'splotchy stage' must be described to the patient before treatment. This is essential for informed consent and to ensure compliance.41
White spots that are present following completion of bleaching treatment may become less noticeable two weeks post treatment, as oxygen dissipates from the tooth and especially the white spot defect, however further treatment may be required to mask the defect.34
Brown and yellow staining
Isolated yellow and brown stains result from numerous aetiologies.12 Fluorosis may result in brown blemishes as seen in Figures 1a, 1b and 1c. Brown stains can be removed 80% of the time by bleaching alone and as such, should be the first line of treatment for such conditions.42 Cases where bleaching does not completely remove brown staining should utilise additional microabrasion and bonding procedures.43
Coronal defects
Coronal defects can present as discrepancies in tooth shape, size, position, proportion, shade and number. Bleaching often forms an integral part in management of aesthetics and can reduce the need for invasive restorations in the management of such cases. No better is this illustrated in use of bleaching, bonding and orthodontics as compared to the use of porcelain veneers and crowns. Furthermore, the use of bleaching to lighten the value of a tooth, can reduce the requirement for excessive reduction required for indirect restorations to mask discolouration appropriately. This enables the use of more translucent, multi-chromatic restorations, thus improving the outcome of such treatment modalities. Validation of bleaching in such circumstances is particularly noted in severe tetracycline discolouration.
Bleaching material can also improve the longevity of restorations in the anterior region, which may be failing due to exposure of restorative margins or due to discolouration of underlying tooth structure. Although bleaching materials have no effect on porcelain, they can successfully penetrate and bleach tooth structure beneath porcelain veneers.44
As is true for all bleaching cases, further restorative treatment should be delayed for at least two weeks following the completion of bleaching. Bond strength to composites is reduced by 25–50% during bleaching,45 however, returns to normal two weeks following treatment. This results from oxygen, in the enamel because of the bleaching material, inhibiting the set of resin tags in etched enamel. Over a two-week period, the oxygen dissipates out of the enamel thus returning bond strength to normal.
Oxygen present in enamel can also lead to incorrect shade taking and thus, shade taking should also be delayed by at least two weeks and up to six weeks in cases whereby exact shade matching is at a premium.
Molar incisor hypomineralisation (MIH)
MIH lesions often present as demarcated enamel opacities ranging in colour from creamy white to yellow/brown, as seen in Figure 6. It is well documented that children with MIH may suffer from a reluctance to smile or a lack of confidence due to the appearance of their teeth and thus may require treatment early to prevent this.46 Bleaching has been reported to produce some improvement in MIH patients, especially with the yellow brown discoloured defects.47

Labial view of the dentition in a patient with MIH
Teeth affected by MIH show inflammatory changes within the pulp48 and as a result, sensitivity is more common among this group of patients. Therefore, adequate sensitivity prevention before undertaking bleaching treatment is required.
Hereditary factors
Several hereditary conditions can lead to white blemishes and white discolouration of teeth. These markings can be generalised for example in amelogenesis imperfecta (AI) patients (Fig. 7) or there can be a single isolated white mark or white blemish on a tooth. Depending on the severity, tooth whitening can be undertaken as the first option for this group of patients.

Labial view of a patient with a discoloured dentition where the diagnosis is one of amelogenesis
Hereditary conditions associated with defects in enamel and dentine include:
1. Hereditary conditions associated with defects of epithelial tissues:49
-
Congenital erythropoietic porphyria
-
Ectodermal dysplasia
-
Epidermolysis bullosa
-
Tuberous sclerosis
2. Hereditary conditions associated with defects in mineralisation pathways:
-
DiGeorge syndrome50
-
Vitamin D dependent rickets,51 Vitamin D resistant rickets,52 pseudovitamin D deficiency rickets53
3. Dentinogenesis imperfecta54
4. Amelogenesis imperfecta:55
-
Hypoplastic
-
Hypomineralised: hypomaturation (including hypomaturtion-hypoplastic with tuarodontism) and hypocalcified
5. Cystic fibrosis56
Bleaching has been shown to be successful in the minimal invasive treatment of hereditary conditions especially amelogenesis imperfecta57 and dentinogenesis imperfecta.54 This is extremely beneficial for such patients as preservation of existing enamel is crucial in such conditions. Sensitivity may also be an issue for patients with hereditary defects and adequate sensitivity prevention is required.
Traumatised/non-vital teeth
Discolouration associated with trauma or loss of tooth vitality can be very severe and range in colour from yellow, black, brown, purple and grey (as seen in Figure 8).

a and b) Discoloured upper left central incisor in a 13-year-old child following trauma with an aesthetic result following bleaching
Haemorrhage of the pulp is the most common cause of discolouration after trauma. Blood enters the dentinal tubules and then decomposes leading to a deposit of chromogenic blood degradation products, such as haemosiderin, hemine, haematin, and haematoidin. Chromogenic degradation products also result from pulp necrosis.58
Calcific metamorphosis may also results in discolouration and is commonly seen as early as three months after traumatic tooth injury. It is characterised by the deposition of hard tissue within the root canal space and a yellow discolouration of the clinical crown.59
Discolouration may result from iatrogenic induced causes following treatment of the non-vital tooth. These include:
-
Root canal cement or gutta percha in the coronal portion of the access cavity
-
Remnants of the pulp and pulp horns following access cavity preparation60
-
Combining sodium hypochlorite (even at low concentrations) and chlorhexidine irrigation which may result in formation of brownish-red precipitates.61
It is essential that iatrogenic causes are appropriately identified and managed before commencing with bleaching treatment.
Discoloured teeth with a history of trauma should undergo vitality testing and if no previous radiographs have been taken, appropriate radiographic assessment should be undertaken to ensure appropriate treatment is undertaken prior to and post bleaching.62
A single discoloured tooth which retains vitality, for example in calcific metamorphisis,59 should not have elective root canal treatment undertaken. These patients should rather be provided with a 'single tooth' bleaching tray as seen in Figure 9 and bleaching agent applied externally, solely to the targeted discoloured tooth. This is because externally applied bleaching material diffuses readily through teeth and uniformly changes dentine shade throughout, regardless of depth.63

A 'single tooth' bleaching tray is a vacuum formed custom bleaching tray whereby windows have been cut from the labial of the tray on the teeth adjacent to the target tooth
There are several different non-vital bleaching techniques and these have been described elsewhere in the literature.64,65 The author would recommend the inside/outside closed bleaching technique for the adolescent patient. This involves sealing 10% CP into the pulp chamber and providing the patient with a 'single tooth' bleaching tray, who continues bleaching externally at home. This technique allows for adequate cleaning of the pulp chamber without the associated risks of leaving the access cavity open and allows repeated frequent application of bleaching agent externally, thus allowing maximum whitening of the tooth without the patient returning to the practice.
Some may choose to utilise the inside outside open technique. This would involve leaving the access cavity open to allow frequent replacement of the bleaching agent intracoronally, which would otherwise become inactive up to ten hours post application. As mentioned previously, this is unnecessary due to the rapid penetration of bleaching material through the tooth from the external surface. Furthermore, this may also potentially jeopardise the root canal treatment, if the patient fails to keep the access cavity appropriately clean or fails to return in a timely fashion for the access cavity to be closed. As such, this technique should only be used on well-motivated patients who are excellent attenders and with excellent oral hygiene.
Systemic diseases
Numerous systemic diseases can lead to discolouration including but not limited to:
-
Premature birth and low birthweight66
-
Diseases of the blood67
-
Neonatal jaundice
-
Neonatal kidney and liver disease.68
Antibiotics used to treat systemic infections, such as tetracycline,69 amoxicillin38 and ciprofloxacin can also lead to discolouration of teeth. The discolouration experienced as a result of systemic disease is most likely to be intrinsic in nature and, as such, requires prolonged bleaching. Tetracycline staining has been shown to require up to six months of prolonged custom tray-applied 10% CP bleaching to ensure a satisfactory effect.69 This whitening effect has been shown to remain in 60 and 90-month follow up studies.70,71
Changes to bleaching protocol in under-18 patients
Haywood has recommended commencing bleaching in adolescent patients at ages 10–14,40 however, this should still be assessed on an individual basis as discussed earlier (Box 2). A close fitting, non-reservoir, custom tray is recommended for these patients to minimise the amount of bleaching material.72
Carbamide peroxide (CP) is the recommended bleaching product for under-18 patients. This is due to the additional urea having beneficial cariostatic effects and an antibacterial effect which have been shown to improve gingival scores.40,73,74,75 This would be of extreme benefit to the patients listed in Box 1, who commonly suffer from poor gingival health resulting from a lack of motivation or sensitivity. Furthermore carbopol, a slow oxygen releasing agent present in 10% CP, results in a steady slow release of oxygen making the process sustainable through the night.76
Tray design for under-18s
There were initially concerns that wearing beaching trays could impede tooth eruption. Although no research has been undertaken assessing this, current orthodontic opinion is that such trays do not impede eruption and can be safely used for the short time required for bleaching.
The best tray design for under-18s would be vacuum formed, custom made, non-reservoir, close fitting trays made from 0.35 mm soft acrylic. With regards to scalloping design, this is based on clinician's preference. Some clinicians prefer to scallop the tray to avoid any soft tissue contact of the bleaching material with the gingiva. However, extreme care is needed in the tray fabrication to avoid jagged edges on the tray which discourage compliance. There is a greater chance of leakage of material if not well made, so only a minimum of bleaching material should be inserted into the tray. Reservoirs or spacers have been shown to be unnecessary.77
A non-scalloped tray design tends to seal better against the soft tissue, and be more comfortable to wear. Although it would allow the 10% carbamide peroxide to contact the tissue, the CP material is made to contact tissue. The original intent of 10% CP was as an oral antiseptic for wound healing of soft tissue, so generally there is no negative consequence for tissue contact. Should there be any issues, those areas of the tray can be shortened to the scalloped design.
Custom trays should be worn for a minimum of two hours under parental supervision. Either daytime or overnight wear is acceptable, however, as CP can remain active for up to ten hours,78 overnight use is recommended for maximum benefit.
Generally children with malformed or discoloured teeth are very motivated to remove the defect, so comply with treatment very well, especially under parental supervision. If compliance is an issue, treatment should not be undertaken.
Managing sensitivity from bleaching treatment
As discussed previously, sensitivity from bleaching treatment is common and this must be explained to all patients before undertaking treatment. In the majority of bleaching patients, history of sensitivity is the greatest predictor for sensitivity during treatment79 and as such a detailed sensitivity history is required on initial patient examination.
However, for certain groups of patients predisposed to sensitivity such as patients with MIH, AI and other hereditary defects, adequate sensitivity prevention before undertaking treatment would be beneficial. Prevention may be in the following forms:
-
Brushing with a desensitising toothpaste containing potassium nitrate for two weeks before commencing treatment and during bleaching treatment80
-
Wearing of the bleaching tray without bleaching agent for two nights before treatment
-
Wearing of bleaching trays with desensitising agent for two nights before treatment. Ideally this would be potassium nitrate containing,81 however, other products such as ACP-CPP may be beneficial. Regardless of product used, it is essential this is sodium lauryl sulphate (SLS) free, as SLS may result in gingival irritation
-
Alternating nights between bleaching agents and desensitising agents. This can be titrated to the degree of sensitivity, for example, in severe cases, one night of bleaching may be followed by three nights of desensitising agent use
-
Using a low concentration bleaching agent, for example a 5% bleaching agent.82 This is beneficial as bleaching sensitivity is concentration dependant83
-
Using a bleaching agent containing potassium nitrate and flouride.84
If sensitivity is experienced during treatment, two approaches can be undertaken. A passive approach could be taken, whereby the frequency of application of CP or wearing time is reduced. Alternatively, an active approach, employing the use of desensitising agents either in the custom tray or applied during brushing (as described in prevention).
Sensitivity resulting from wearing of the bleaching tray alone, as mentioned previously, is commonly associated with the mechanical pressure of an improperly fitting tray, from occlusion on the tray, and is more common with harder bleaching trays. It is therefore essential that an accurate impression is made and a soft tray is used to prevent or alleviate the tray associated sensitivity.
Conclusion
Tooth bleaching continues to be one of the cornerstones of minimal intervention aesthetic dentistry. Its use, having previously been limited to the over-18 patients, can provide adolescent patients with good aesthetic results, minimal side-effects and minimal safety concerns. Furthermore, effective tooth whitening results can improve patients' self-esteem, self-confidence and can help address key psychosocial issues associated with discolouration.
References
EU. Council Directive 2011/84/EU. 2011. Available at https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2011:283:0036:0038:en:PDF (accessed June 2018).
Dental Protection. Advice on tooth whitening. 2014. Available at http://www.dentalprotection.org/uk/publications-resources/updates/updates/2014/12/08/tooth-whitening (accessed June 2017).
Saunders W P, Saunders E M . Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J 1998; 185: 137–40.
Petridis H P, Zekeridou A, Malliari M, Tortopidis D, Koidis P, Survival of ceramic veneers made of different materials after a minimum follow-up period of five years: a systematic review and meta-analysis. Eur J Esthet Dent 2012; 7: 138–52.
General Dental Council. Position statement on tooth whitening. https://www.gdc-uk.org/api/files/Tooth-Whitening-Position-Statement.pdf (accessed September 2017).
Dickstein B . Neonatal oral candidiasis: evaluation of a new chemotherapeutic agent. Clin Paediatr 1964; 3: 485–488.
Zinner D D, Duany L F, Chilton N W . Controlled study of the clinical effectiveness of a new oxygen gel on plaque, oral debris and gingival inflammation. Pharmacol Ther Dent 1970; 1: 7–15.
Shipman B, Cohen E, Kaslick R S . The effect of a urea peroxide gel on plaque deposits and gingival status. J Periodont 1971; 42: 283–285.
Tartakow D J, Smith R S, Spinelli J A . Urea peroxide solution in the treatment of gingivitis in orthodontics. Am J Orthodont 1978; 73: 560–563, 565–567.
Haywood V B . History, safety and effectiveness of current bleaching techniques: applications of the nightguard vital bleaching technique. Symposium on Esthetic Restorative Materials. 1993. November: 82–92.
Li Y, Greenwall L . Safety issues of tooth whitening using peroxide-based materials. Br Dent J 2013; 215: 29.
L H. Greenwall. Tooth Whitening Techniques Second Edition. Taylor and Francis: London, 2017.
American Dental Association Council on Scientific Affairs. Tooth whitening/bleaching: treatment considerations for dentists and their patients. Chicago: ADA, 2009.
Li Y . Safety controversies in tooth bleaching. Dent Clin North Am 2011; 55: 255–263.
Scientific Committee on Consumer Products (SCCP), European Commission. Opinion on hydrogen peroxide in tooth whitening products. 2005. Available at https://ec.europa.eu/health/ph_risk/committees/04_sccp/docs/sccp_o_022.pdf (accessed June 2018).
Haywood V B, Leonard R H, Nelson C F, Brunson W D . Effectiveness, side effects and long term status of nightguard vital bleaching. J Am Dent Assoc 1994; 125: 1219–1226.
Schulte J R, Morrissette D B, Gasior E J, Czajewski M V . The effects of bleaching application time on the dental pulp. J Am Dent Assoc 1994; 125: 1330–1335.
Leonard R H, Haywood V B, Phillips C . Risk factors for developing tooth sensitivity and gingival irritation associated with nightguard vital bleaching. Quint Int 1997; 28: 527–534.
Tam L . Clinical trial of three 10% carbamide peroxide bleaching products. J Can Dent Assoc 1999; 65: 201–205.
Cooper J S, Bokmeyer T J, Bowles W H . Penetration of the pulp chamber by carbamide peroxide bleaching agents. J Endod 1992; 18: 315–317.
Leonard R H, Garland G K, Eagle J C, Caiman D J . Safety issues when using a 16% carbamide peroxide whitening solution. J Esthet Rest Dent 2002; 14: 358–367.
Bacaksiz A, Tulunoglu O, Tulunoglu I . Efficacy and Stability of Two in-Office Bleaching Agents in Adolescents: 12 Months Follow-Up. J Clin Paediatr Dent 2016; 40: 269–273.
Donly K J, Donly A S, Baharloo L et al. Tooth bleaching in children. Compendium 2002; 23: 22–28.
Donly K J, Gerlach R W . Clinical trials on the use of bleaching strips in children and adolescents. Gen Dent 2002; 50: 242–245.
Donly K J . A controlled clinical trial to evaluate the safety and bleaching efficacy of a 9.5% hydrogen peroxide high-adhesion bleaching strip in a teen population. Am J Dent 2010; 23: 292–296.
Donly K J, Henson T, Jamison D, Gerlach R W . Clinical trial evaluating two peroxide bleaching strips used by teenagers. Gen Dent 2006; 54: 110–112.
Donly K J, Kennedy P, Segura A, Gerlach R W . Effectiveness and safety of tooth bleaching in teenagers. Paediatr Dent 2005; 27: 298–302.
Gerlach R W, Zhou X . Comparative clinical efficacy of two professional bleaching systems. Compend Contin Educ Dent 2002; 23: 35–41.
Camps J, De Frabceschi H, Idir F, Roland C . About I TimeCourse Diffusion of hydrogen peroxide through human dentine: clinical significance for young human dentin. J Endod 2007; 33: 455459.
Donly K J . The adolescent patient: special whitening challenges. Compend Contin Educ Dent 2003; 24: 390–396.
Craig S A, Baker S R, Rodd H D, How do children view other children who have visible enamel defects? Int J Paediatr Dent 2015; 25: 399–408.
Marty M . Time Loss. JDR Clin Transl Res 2016; 20: 1–2.
Arseneault L, Bowes L, Shakoor S . Bullying victimization in youths and mental health problems: 'Much ado about nothing'? Psychol Med 2010; 40: 717–729.
Wallace A, Deery C . Management of Opacities in Children and Adolescents. Dent Update 2015; 42: 951–954, 957–958.
Haywood V B . Pre-Bleaching Examination Vital for Optimum Whitening. Compend Cont Edu Dent 2012; 33: 76–77.
Loyola-Rodriguez J P, de Jesus Pozos-Guillen A, Hernandez-Hernandez F, Berumen-Maldonado R, Patiño-Marin N. Effectiveness of treatment with carbamide peroxide and hydrogen peroxide in subjects affected by dental fluorosis: a clinical trial. J Clin Paediatr Dent 2004; 28: 63–67.
Greenwall L . White lesion eradication using resin infiltration. Aesthet Dent Today 2013: 15–18.
Hong L, Levy S M, Warren J J, Dawson D V, Bergus G R, Wefel J S . Association of amoxicillin use during early childhood with developmental tooth enamel defects. Arch Paediatr Adolesc Med 2005; 159: 943–948.
Leonard R H Jr, Bentley C D, Haywood V B . Salivary pH changes during 10% carbamide peroxide bleaching. Quintessence Int 1994; 25: 547–550.
Haywood V B, Sword R J . Tooth bleaching questions answered. Br Dent J 2017; 223: 369.
Greenwall L . Treatment considerations for bleaching and bonding white lesions in the anterior dentition. Alpha Omegan 2009; 102: 121–127.
Haywood V B . Current status of nightguard vital bleaching. Compendium 2000; 21: S10–S17.
Haywood V B, Leonard R H . Nightguard vital bleaching removes brown discoloration for 7 years: A case report. Quintessence Int 1998; 29: 450–451.
Haywood V B, Parker M H . Nightguard vital bleaching beneath existing porcelain veneers: a case report. Quintessence Int 1999; 30: 743–747.
Cvitko E, Denehy G E, Swift E J, Jr., Pires J A . Bond strength of composite resin to enamel bleached with carbamide peroxide. J Esthet Dent 1991; 3: 100–102.
Fayle SA . Molar incisor hypomineralisation: restorative management. Eur J Paediatr Dent 2003; 4: 121–126.
Rodd H, Abdul Karim A, Yesudian G, O'Mahony J, Marshman Z . Seeking children's perspectives in the management of visible enamel defects. Int J Paediatr Dent 2011; 21: 89–95.
Rodd H D, Boissonade F M, Day P F . Pulpal status of hypomineralized permanent molars. Paediatric Dent 2007; 29: 514–520.
Seow W K . Developmental defects of enamel and dentine: challenges for basic science research and clinical management. Aust Dent J 2014; 59: 143–154.
Nordgarden H, Lima K, Skogedal N, Følling I, Storhaug K, Abrahamsen T G . Dental developmental disturbances in 50 individuals with the 22q11.2 deletion syndrome; relation to medical conditions? Acta Odontol Scand 2012; 70: 194–201.
Malloy P, Feldman D . Genetic disorders and defects in vitamin D action. Endocrinol Metab Clin 2011; 39: 333–346.
Seow W K, Latham S C . The spectrum of dental manifestation in vitamin Dresistant rickets: implications for management. Paediatr Dent 1986; 8: 245–250.
Patzer L, van't Hoff W, Dillon M J . Xlinked hypophosphataemic rickets: recognition, treatment and prognosis. Curr Paediatr 1998; 8: 26–30.
Croll T P . Carbamide Peroxide Bleaching of teeth with Dentinogenesis imperfecta: a report of a case. Quintessence Int 1995; 26: 683–686.
Patel M, McDonnell S T, Iram S, MF W Y C . Amelogenesis imperfecta-lifelong management. Restorative management of the adult patient. Br Dent J 2013; 215: 449–457.
Primosch R E . Tetracycline discoloration, enamel defects, and dental caries in patients with cystic fibrosis. Oral Surg Oral Med Oral Pathol 1980; 50: 301–308.
Nathwani N S, Kelleher M . Minimally destructive management of amelogenesis imperfecta and hypodontia with bleaching and bonding. Dent Update 2010; 37: 170–172, 175–176, 179.
Arens D . The role of bleaching in Esthetics. Dent Clin North Am 1989; 33: 319–36.
Amir F A, Gutmann J L, E Witherspoon D E . Calcific metamorphosis: a challenge in endodontic diagnosis and treatment. Quintessence Int 2001; 32: 447–455.
Zimmerli B, Jeger F, Lussi A . Bleaching of Nonvital teeth: A clinically Relevant Literature Review. Schweiz Monatsschr Zahnmed 2010; 120: 306–320.
Basrani B R, Manek S, Sodhi R N, Fillery E, Manzur A . Interaction between sodium hypochlorite and chlorhexidine gluconate. J Endod 2007; 33: 966–999.
Horner K, Eaton K A . Selection Criteria for Dental Radiography. 3rd edition. London, UK: Faculty of General Dental Practitioners, 2015.
Mccaslin A J, Haywood V B, Potter B J, Dickinson G L, Russell C M . Assessing dentin colour changes from nightguard vital bleaching. J Am Dent Assoc 1999; 130: 1485–1490.
Haywood V B, DiAngelis A J . Bleaching the single dark tooth. Inside Dent 2010; 6: 42–52.
Sulieman M . An overview of bleaching techniques: 2. Night Guard Vital Bleaching and non-vital bleaching. Dent Update 2005; 32: 39–46.
Seow W K . Effects of preterm birth on oral growth and development. Aust Dent J 1997; 42: 85–91.
Watanabe K, Shibata T, Kurosawa T et al. Bilirubin pigmentation of human teeth caused by hyperbilirubinaemia. J Oral Pathol Med 1999; 28: 128–130.
Pindborg J J . Aetiology of developmental enamel defects not related to fluorosis. Int Dent J 1982; 32: 123–34.
Haywood V B . Extended bleaching of tetracyclines tained teeth: a case report. Contemp Esth Restor Pract 1997; 1: 14–21.
Leonard R H, Haywood V B, Eagle J C et al. Nightguard vital bleaching of tetracycline-stained teeth: 54 months post treatment. J Esthetic Restor Dent 1999; 11: 265–77.
Matis B A, Wang Y, Eckert G J, Cochran M A, Jiang T . Extended bleaching of tetracycline-stained teeth: a 5year study. Oper Dent 2006; 31: 643–651.
Lee S S, Zhang W, Lee D H, Li Y . Tooth bleaching in children and adolescents: a literature review. Paediatr Dent 2005; 27: 362–368.
Greenwall-Cohen J, Greenwall L . Carbamide Peroxide and its use in Oral Hygeine and Health. Dent Update 2017; 44: 863–869.
Haywood V B . Bleaching and caries control in elderly patients. Aesth Dent Today 2007; 1: 42–44.
Curtis J W, Dickinson G L, Downey M C et al. Assessing the effects of 10 percent carbamide peroxide on oral soft tissues. JADA 1996; 127: 1218–1223.
Matis B A . Tray whitening: what the evidence shows. Compend Contin Educ Dent 2003; 24: 354–362.
Matis B A, Hamdan Y S, Cochran M A, Eckert G J . A clinical evaluation of a bleaching agent used with and without reservoirs. Oper Dent 2002; 27: 5–11.
Matis B A, Gaiao U, Blackman D, Schultz F A, Eckert G J . In vivo degradation of bleaching gel used in whitening teeth. JADA 1999; 130: 227–235.
Pashley D H, Tay F R, Haywood V B, Collins M A, Drisko C L . Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. Comp Contin Edu Dent 2008; 29: 1–35.
Haywood V B, Cordero R, Wright K, et al. Brushing with a potassium nitrate dentifrice to reduce bleaching sensitivity. J Clin Dent 2004; 16: 17–22.
Haywood V B, Caughman W F, Frazier K B, Myers M L . Tray delivery of potassium nitratefluoride to reduce bleaching sensitivity. Quintessence Int 2001; 32: 105–109
Hyland B W, Macdonald A, Lewis N et al. A new three component formulation for the efficient whitening of teeth(Carbadmide Peroxide Plus). Clin Oral Invest 2015. 19: 1395–1404.
Basting R T, Amaral F L, França F M, Flório F M . Clinical comparative study of the effectiveness of and tooth sensitivity to 10% and 20% carbamide peroxide home-use and 35% and 38% hydrogen peroxide in-office bleaching materials containing desensitizing agents. Oper Dent 2012; 37: 464–473.
Tam L . Effect of potassium nitrate and fluoride on carbamide peroxide bleaching. Quintessence Int 2001; 32: 766–770.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Greenwall-Cohen, J., Greenwall, L., Haywood, V. et al. Tooth whitening for the under-18-year-old patient. Br Dent J 225, 19–26 (2018). https://doi.org/10.1038/sj.bdj.2018.527
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2018.527
This article is cited by
-
Evaluation of bleaching agent effects on color and microhardness change of silver diamine fluoride-treated demineralized primary tooth enamel: An in vitro study
BMC Oral Health (2022)
-
Patient-reported outcome measures for children and adolescents having dental bleaching in the UK
European Archives of Paediatric Dentistry (2022)
-
Patient-reported outcome measure for children and young people with amelogenesis imperfecta
British Dental Journal (2021)
-
Is it time to reconsider the use of vital teeth bleaching in children and adolescents in Europe?
European Archives of Paediatric Dentistry (2021)
-
Vital bleaching for children with dental anomalies: EAPD members’ survey
European Archives of Paediatric Dentistry (2020)
