
Key Points
-
Informs the viability of coronectomy of deciduous teeth as a viable treatment option applicable to oral surgeons, orthodontists and GDPs.
-
Highlights importance of discussing associated risks.
-
Highlights importance of sparing the inferior dental nerve and associated litigation.
Abstract
Coronectomy is a widely-accepted technique available for the treatment of impacted wisdom teeth. The fundamental principle is to prevent trauma to the inferior dental nerve (IDN). Many publications have demonstrated its positive outcomes but there is no literature available regarding coronectomy of deciduous teeth. This case report highlights the complex approach to managing a severely infraoccluded 85 in the mixed dentition of a 10-year-old female. The report demonstrates and discusses the combined orthodontic and oral surgical approach to prevent damage to the IDN and to allow space for orthodontic movement. This case demonstrates how nerve sparing techniques in the mixed dentition are achievable.
Clinical relevance statement When managing severely infraoccluded and impacted deciduous second molars, clinicians must be aware that the option of a coronectomy should be considered and may be the difference between sparing the nerve or causing permanent injury.
Objective The reader should understand that coronectomy is a suitable treatment option in managing impacted deciduous teeth.
Similar content being viewed by others


Case report
Coronectomy is a widely-accepted technique in managing symptomatic impacted wisdom teeth.1 The fundamental principle is to prevent trauma to the inferior dental nerve (IDN).2 Many publications have demonstrated its positive outcomes. The authors would like to share and highlight the use and importance of this technique in oral and maxillofacial surgery. The technique of coronectomy should be considered in cases other than wisdom teeth.
A 10-year-old female was referred to the orthodontic department at Pinderfields Hospital regarding delayed eruption of permanent teeth and severe crowding. She presented in the mixed dentition with a Class I skeletal pattern and Class I incisal relationship. There was an anterior cross-bite along with severe crowding in both upper and lower arches and it was seen that there was insufficient space for all the permanent teeth to erupt.
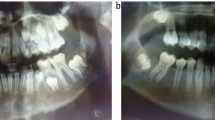
Clinical and radiographic investigation was undertaken. An orthopantomogram (OPG) confirmed presence of all successors. It also revealed a severely infraoccluded lower right second deciduous molar (85) significantly below the occlusal plane, preventing eruption of the adjacent permanent premolars and canine (Fig. 1).

Pre-operative OPG
Interceptive orthodontics was part of the management plan in this case, using an upper removable appliance to correct the anterior cross bite. However, the 85 required a multidisciplinary approach involving orthodontist and oral and maxillofacial surgeons.
Problem list
-
Severe crowding of the upper and lower arches
-
Anterior-posterior skeletal discrepancy
-
Upper anterior cross-bite
-
Transverse skeletal discrepancy
-
Variation in mandibular body heights
-
Infraoccluded and impacted 85.
Aetiology
This case presents with malocclusion due to skeletal growth disturbances. No evidence is seen in which soft tissue or habits play a role.
A cone beam computed tomography (CBCT) scan was taken to further assist in surgical planning for managing the infraoccluded 85 (Figs 2 and 3).3

CBCT-sagittal view

CBCT-coronal view
The CBCT demonstrates the 85 roots are contacting the inferior cortex of the mandible. Additionally, it shows no clear cortical outline between the IDN and the roots, while displaying intimate contact with the middle third of both roots.
Initial considerations before the CBCT result were to surgically remove the 85. Following a multidisciplinary discussion with a consultant orthodontist and a maxillofacial surgeon, it was advised there is high risk of injuring the IDN and possible mandibular fracture. Thus a coronectomy of the 85 was considered (Fig. 4).

Advantages and disadvantages of coronectomy versus complete removal of the '85'
Orthodontic movement of the teeth in the years ahead may be compromised to a degree. However, careful analysis using the CBCT scan demonstrated the roots of the 85 are lying very low and in contact with the inferior cortex of the mandible. This was deemed orthodontically acceptable because as the patient's mandible continues to grow and the height of the body increases there would be no or relatively little impaction on the permanent teeth. Furthermore, in the future if orthodontic forces were to be applied to the permanent teeth, leading to contact against the roots of the deciduous tooth, it would be sufficient to further activate the resorption process.4,5,6Therefore, the permanent teeth would not be obstructed from erupting and movement during orthodontic treatment would not be hindered.7
IDN damage is an important factor in deciding how to proceed. Injury to the nerve may lead to temporary or permanent altered sensation to the lower lip, chin and tongue. In real terms, this may have a profound effect on daily functions such as speaking, eating, kissing and even playing a wind instrument. Weighing up the risks and benefits along with the patient's choice, we planned for a coronectomy of the 85 under general anaesthetic. We believe that minimally invasive surgery would give an increased margin of safety to avoid injury to the IDN and adjacent structures. Combining this thought process along with the patient's age and the fact that the roots were lying very low in the mandible, we felt the planned procedure was justified.
Like all coronectomy techniques the patient was warned of risks of requiring a complete removal or a second procedure in the future. Piezosurgery was used due to its ability to deliver precise cuts in confined areas. The coronectomy of the 85 was conducted as planned with no complications. Figure 5 shows an OPG taken three months post-operation.

Orthopantomogram taken three months post-operation (please forgive the image which displays the upper retainer and earrings in situ)
The patient was monitored at three monthly intervals and to date a one-year post-operative review demonstrates that the patient is asymptomatic with no reported episodes of infection. The lower right first and second premolars have now partially erupted. This case demonstrates that this surgical problem can be managed to reduce the chance of injury to the IDN and without damage to the adjacent teeth, or the integrity of the lower border of the mandible.8
It is important that all clinicians, GDPs, oral surgeons, orthodontists and maxillofacial surgeons are aware of alternative approaches in managing infraoccluded deciduous teeth. The coronectomy technique is a surgical option and should be given due consideration. A multidisciplinary approach and the use of CBCT aided in providing a solution to this problem.
References
Renton T . Update on Coronectomy A safer way to remove high risk mandibular third molars. Dent Update 2013; 40: 362–364, 366–368.
Renton T . Prevention of iatrogenic inferior alveolar nerve injuries in relation to dental procedures. Dent Update 2010; 37: 350–352, 354–356, 358–36.
Hatano Y, Kurita K, Kuroiwa Y, Yuasa H, Ariji E . Clinical evaluations of coronectomy (intentional partial odontectomy) for mandibular third molars using dental computed tomography: a case-control study. J Oral Maxillofac Surg 2009; 67: 1806–1814.
Cuminetti F, Boutin F, Frapier L . Predictive factors for resorption of teeth adjacent to impacted maxillary canines. J Int Orthod 2017; 15: 54–68.
Pereira I F, Santiago F Z M, Sette-Dias A C, Noronha V R A S . Taking advantage of an unerupted third molar: a case report. Dent Press J Orthod 2017; 22: 97–101.
Guarnieri R, Cavallini C, Vernucci R, Vichi M, Leonardi R, Barbato E . Impacted maxillary canines and root resorption of adjacent teeth: A retrospective observational study. Med Oral Patol Oral Cir Bucal 2016; 21: e743–e750.
Nahhas R W, Valiathan M, Sherwood R J . Variation in timing, duration, intensity, and direction of adolescent growth in the mandible, maxilla, and cranial base: The Fels longitudinal study. Anat Rec 2014; 297: 1195–1207.
Mukherjee S, Vikraman B, Sankar D, Veerabahu M . Evaluation of outcome following coronectomy for the management of mandibular third molars in close proximity to inferior alveolar nerve. J Clin Diagn Res 2016; 10: ZC57–ZC62.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hussain, M., Sah, S. & McHenry, I. Case report: coronectomy of an impacted and submerged second deciduous molar. Br Dent J 224, 20–21 (2018). https://doi.org/10.1038/sj.bdj.2018.3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2018.3
This article is cited by
-
The patient-dentist relationship and the future of dentistry
British Dental Journal (2018)
