
Key Points
-
Suggests that dental health is important to patients, even in the context of other multisystem trauma. It aids physical and psycho-social recovery.
-
Highlights that multidisciplinary management is vital in providing patients with holistic care.
-
Demonstrates how continued and particularly immediate involvement of paediatric dentistry helped to mitigate long-term dental complications. This reduced the likelihood of pain and general anaesthetic burden for dental treatment and their associated morbidity.
Abstract
This paper outlines the involvement of dentists in the treatment of patients following the terror attack at Manchester Arena on 22 May 2017. It predominantly describes the role of the authors – a paediatric dental consultant and maxillofacial surgery dental core trainee (DCT). As a result of the incident a number of patients suffered oro-facial injuries, with many treated at Central Manchester Foundation Trust Hospitals' Manchester Royal Infirmary and Royal Manchester Children's Hospital. The major incident response of the trust is discussed, as are the presentation of blast injuries and corresponding NHS guidance. Two paediatric cases present the role of the paediatric dental consultant in the acute, intermediate and long-term management of these patients. The presentation of unique dento-alveolar injuries in the context of other trauma and their subsequent treatment demanded true multidisciplinary management. The importance of teeth and oral health to physical and psycho-social wellbeing and recovery was clear and recognised by other teams involved in the patients' management. The experience reinforced the overall impact dental health has on physical and psycho-social health, and how a holistic approach is integral to treatment of major trauma.
Similar content being viewed by others



Introduction
The terror attack on Manchester Arena resulted in fatalities and many seriously injured adults and children. A major incident of this type involving children was unprecedented in the UK and the unique presentation of dental and facial injuries alongside multiple other injuries in younger patients meant the involvement of maxillofacial and paediatric dental teams was crucial to their holistic management. This paper describes the important role played by the maxillofacial DCT and paediatric dental consultant.
Background
On 22 May 2017 at 22:31 an explosive device containing metal nuts and bolts was detonated at Manchester Arena injuring concert goers and waiting parents in the foyer between the Arena and Manchester Victoria train station. Twenty-two people (adults and children) were killed with a further one hundred and sixteen admitted to hospital.1,2 Sixty-eight were still in hospital three weeks after the attack, with twenty-three in critical care.1,2
The device caused metal objects to fly at high velocity, resulting in fatalities up to 20 m away from the explosion.1,2 Multiple injuries were caused by penetration of foreign bodies and shrapnel, thermal burns, falls and blast shockwaves. It is recognised that blast injuries have a unique presentation and therefore there is specific NHS guidance for major blast injuries.
Types of blast injury3,4,5
-
Primary: the explosion has a blast front of overpressurised air; this change in ambient air pressure causes primary blast injuries. The increased temperature can cause third degree burns which can be fatal
-
Secondary: secondary blast injuries are caused by shrapnel and foreign objects moving at high velocity due to the blast. These can cause blunt or penetrating trauma and are the most common type of blast injury; they should be treated aggressively
-
Tertiary: these injuries are a result of the person being propelled by the velocity of the blast waves into objects or structures, usually resulting in blunt trauma
-
Quaternary: injuries not as a direct result of the blast but a result of its effects, for example, inhalation of toxic substances and asphyxiation or biological agents carried in the bomb or by the bomber. Specialist intervention is required to actively exclude and treat injuries to the tympanic membranes, eyes and face. All patients with wounds should have tetanus and Hepatits B prophylaxis along with HIV testing. A trust microbiological protocol was put into place for all blast victims in Manchester
-
Psychological trauma: all patients should be seen by psychiatric services at an appropriate time.
Blast injuries therefore present a distinct challenge. Dental injuries differ in nature and prognosis from other dental trauma or pathology. Most victims in Manchester suffered multiple injuries at multiple sites requiring management by large multidisciplinary teams, often bigger than a standard trauma team. Several patients suffered maxillofacial injuries and two paediatric patients required immediate and long-term management by the paediatric dental team.
The role of Central Manchester Foundation Trust (CMFT) in a major incident
The Trust deployed its major incident plan when a major incident was declared at 00:00. It details roles and the hierarchy of divisions, along with plans for elective patients, bed management and theatre management.
Pre-hospital priorities included safety (securing and then clearing the scene in the minimum time), clear and effective communication, transport, the tracking of patients and documenting injuries and treatment. At the scene casualties were triaged as priority 1 (immediate), 2 (urgent) and 3 (delayed) according to their injuries and then stabilised and evacuated in order of priority to the appropriate emergency setting. The risk of further explosions meant the site had to be made safe before emergency services could enter, delaying the evacuation of many priority 1 and 2 patients by several hours. The walking wounded were therefore some of the first to arrive at hospitals.
As the only tertiary children's hospital in the region, Royal Manchester Children's Hospital (RMCH) was the admitting hospital for priority 1, 2 and 3 paediatric casualties. Many complex patients with multiple injuries were admitted, often with other injured adult family members as the Trust tried to keep families together where possible. In total 24 children and five mothers were treated in the Paediatric Emergency Department (ED) at RMCH, with 13 children and all five mothers being admitted. One further patient was transferred to RMCH from Stockport. Manchester Royal Infirmary (MRI) ED, which is on the same site as RMCH, treated 26 patients where two unfortunately died and 13 were admitted. Manchester Royal Eye Hospital is also on the same site and ophthalmic specialists treated adult and paediatric patients with significant eye injuries.
Injuries sustained
Victims treated within CMFT displayed a variety of the blast injuries described above, often in combination. The majority sustained penetrating injuries from small metal shrapnel and other larger foreign bodies such as nuts and bolts. These were found in all regions of the body requiring surgical involvement from general, orthopaedic, maxillofacial, ophthalmic, neuro and plastic surgeons. Fractures as a result of these foreign bodies along with tertiary impacts were also extremely common. Patients were admitted under a multidisciplinary team (MDT) with a lead clinician. Daily MDT meetings were carried out in the weeks after the incident.
The oro-facial injuries sustained by patients included:
-
Dento-alveolar trauma; avulsions, fractured teeth, luxations, dento-alveolar fractures
-
Soft tissue injuries; lacerations, abrasions and contusions to the face, tongue, and palate
-
Penetrating injuries, lacerations and abrasions to the eyes
-
Penetrating wounds into deep structures
-
Mandibular, maxillary, orbit, nasal and skull fractures
-
Foreign bodies in hard and soft tissue.
Similar patterns and types of injury have been described in the literature after terror attacks and explosions in Iraq.6,7,8,9 An example being the transverse fractures of teeth at the cemento-enamel junction sustained by the patient presented as case 2. These are a similar pattern as those described by Shuker, attributed to the cemento-enamel junction being a point of weakness to the blast front.9
Immediate management and role of the maxillofacial Dental Core Trainee (DCT)
Many patients with maxillofacial injuries were treated at CMFT. Immediate management was to prioritise and assess referrals in both RMCH and MRI and liaise with senior colleagues regarding further steps. This was difficult as many patients had not yet been identified, and situations changed quickly.
Patients were assessed in conjunction with other teams. Initial assessment was then reported to senior members of the oral and maxillofacial surgery (OMFS) team and investigations arranged. Most had CT scans to assess the position and penetration of shrapnel and foreign bodies as well as plain films for assessment of fractures. As referrals to OMFS were mainly after a secondary or tertiary survey, patients often had imaging of other areas already so it was vital to discuss with other teams what further imaging was required before sending patients for scans, in order to prevent further delay and unnecessary transport of patients. This was while simultaneously attending surgical planning meetings and MDT meetings in both RMCH and MRI, involving all surgical teams, anaesthetists, ED and critical care staff.
OMFS were operating on patients in three theatres across the two hospitals, therefore organisation was required to make sure staff were in the correct place and patients were ready for theatre.
As patients had other critical injuries, it was crucial to coordinate with other teams regarding timing of surgeries and availability of surgeons and anaesthetists to keep anaesthetic time to a minimum and utilise resources efficiently. Elective patients were also cancelled and emergency patients not related to the arena attack were reprioritised to ensure the correct treatment precedence was given.
Patients with maxillofacial injuries came under all three priorities: two P1 patients, three P2 patients and one P3 patient. Immediate management in theatre in conjunction with other teams included:
-
Wash outs of all wounds
-
Primary closure of facial wounds
-
Reduction of fractures
-
Removal of foreign bodies and shrapnel
-
Extraction of teeth and tooth fragments.
Involvement of paediatric dentists in acute management
Paediatric dental consultants were asked for opinions on the dento-alveolar injuries in paediatric patients. This was critical in deciding which teeth could be saved and in planning the dental rehabilitation of adolescent victims. Two had sustained complex dental trauma to permanent teeth and the long-term management was complicated by their age and continued growth. Following initial assessment, the paediatric dental team then assisted in the surgical removal of fragments of teeth under general anaesthetic alongside surgeons working on other injuries. This helped to ensure that all teeth were fully assessed and extractions were as atraumatic as possible to preserve bone. It also helped to reduce the number of anaesthetics required and to minimise pain and discomfort from dental injuries, aiding eating and nutrition; key to the children's recovery.
Case 1
Presentation and immediate management
-
A 14-year-old girl was admitted to RMCH ED at 01:16
-
She was conscious on arrival but had recieved several doses of morphine. The lead anaesthetist reported that her main concern on arrival was the loss of her teeth
-
Investigations included CT head, neck, thorax, abdomen and pelvis and radiographs of both upper arms and lower legs (Fig. 1). She had sustained multiple injuries as listed in Table 1 and was transferred straight to critical care for assessment and then to theatre
Figure 1 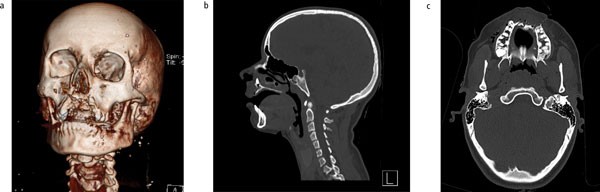
CT scans of the head showing extensive damage to the premaxilla and avulsions/coronal fractures of 12, 11, 21, 22, 23 with a root fragment through the floor of the nose
Table 1 Injuries sustained by Case 1 -
During 10.5 hours under anaesthetic, maxillofacial surgeons and paediatric dentists debrided her facial and oral lacerations, closed wounds with resorbable sutures, removed root remnants from the maxillary fracture and extracted the 24 which had sustained a vertical crown-root fracture
-
She also underwent debridement and superficial closure of the shrapnel wounds on her limbs, external fixation of her left humerus, casts on her lower legs and a laparotomy to investigate possible shrapnel in the stomach which was found to be ingested teeth fragments.

Intermediate management
-
The patient was reviewed by the paediatric dental team on the high dependency unit ten days after the incident. She had undergone three further surgeries to debride wounds and dress burns in this period. She had been kept sedated for five days following initial surgery to allow recovery. She was fed by a nasogastric tube and was still drowsy
-
Conversation with her parents revealed that 'she had had a good set of teeth' and was very keen to have the missing teeth replaced. Examination revealed many difficulties to achieving this including the number of teeth lost, the bony defect already apparent and the fact she was still both growing and healing (Fig. 2)
Figure 2 
Intra-oral photographs showing the extent of dental injuries and bone loss in Case 1, 28 days after the incident
-
The plan was to produce a partial denture as an intermediate measure until growth was complete. On hearing this plan the patient and her family were upset; the wait for a fixed prosthesis felt like an eternity to a 14-year-old girl
-
Reassurance that the dentures would look as natural as possible was given and a deal was made that the process could only start when she was taking food orally. This was sufficient incentive to start eating and the nasogastric tube was removed two weeks later
-
Intensive prevention was reinforced at this stage, as often dental hygiene can be neglected with so many other things to tackle. Oral hygiene advice was given and a 2,800 ppm fluoride toothpaste prescribed as well as chlorhexidine gel for the intra-oral lacerations
-
Her parents provided photographs of her teeth before the incident, and these were used by the laboratory technician to produce a natural looking denture. The process started on the ward and was completed in the clinic when the patient was mobile enough to attend. The dentures were fitted in time for her discharge from hospital, just over five weeks after the incident (Fig. 3).
Figure 3 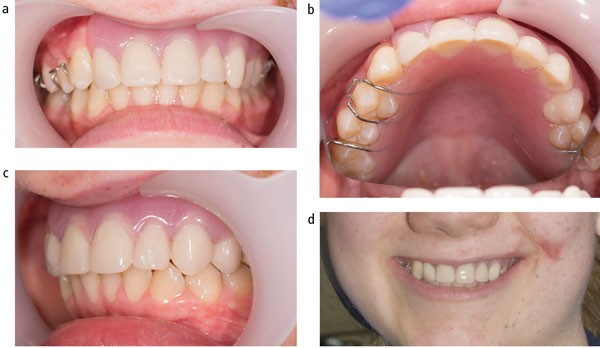
Case 1 with dentures in situ (35 days after incident)
-
Sensibility tests of adjacent teeth, an orthopantogram and intraoral radiographs were taken when she was able to attend the dental department (Figs 4 and 5). These show the extent of bone lost in the anterior maxilla and also reveal root remnants 12, 23 and 24 regions. All adjacent teeth responded positively to sensibility tests and will be monitored regularly for signs of loss of vitality or resorption, a complication described after a blast incident in Pakistan.8 The root remnants will be left in situ as they are helping to preserve bone in the anterior maxilla.
Figure 4 
Orthopantogram of Case 1 taken 30 days after the incident
Figure 5 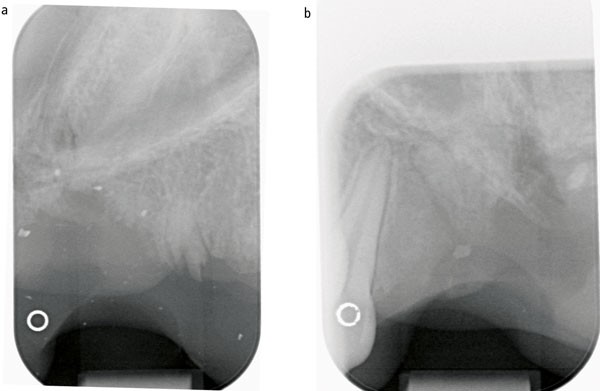
Intra-oral radiographs of the anterior maxilla and upper left quadrant, showing root remnants 12, 23 and 24




Dentures were a key part of her discharge and helped to build her confidence. She had set herself the goal of returning to school and giving a speech to the whole school at the end of term. The dentures therefore had to look natural but she also had to be able to speak with them in. She succeeded in both of these aspects.
Future treatment needs
This young lady is understandably very keen to have permanent replacement of her anterior teeth. Restorative dental consultants were therefore involved from an early stage to ensure that she gets the best long-term cosmetic and functional result. Once further bony healing has occurred, oral and maxillofacial surgeons in conjunction with the restorative dentists are planning to place implants at an earlier age than normal, that is, before growth is completed, to help prevent further loss of bone, particularly in a vertical dimension. It is hoped this will also help with the patient's physical and emotional rehabilitation.
Case 2
Presentation
-
A 15-year-old boy was admitted to RMCH ED at 02:45 am
-
He was conscious on arrival but was sedated with a Glasgow Coma Scale of 13
-
Clinical examination revealed a 16 mm × 14 mm through and through laceration of his right cheek, a foreign body in his right eye, a large submental and a scalp laceration as well as an implanted foreign body in his posterolateral neck. Puncture wounds were also noted on his lower limbs
-
Intra-orally there was extensive damage to his 27, 37 and upper and lower teeth on the right side, and lacerations to both lateral borders of his tongue
-
Investigations included CT head, facial bones, C spine, chest and abdomen and lower limb radiographs (Figs 6, 7, 8) and confirmed multiple injuries as listed in Table 2
Figure 6 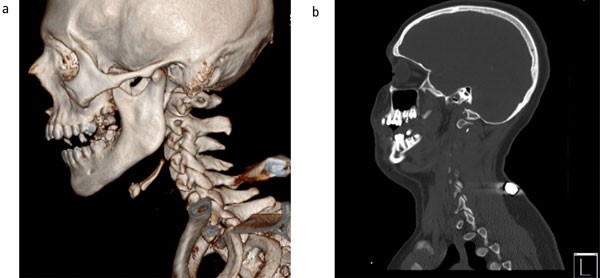
CT head scans showing fractures of 27 and 37 and foreign body in neck
Figure 7 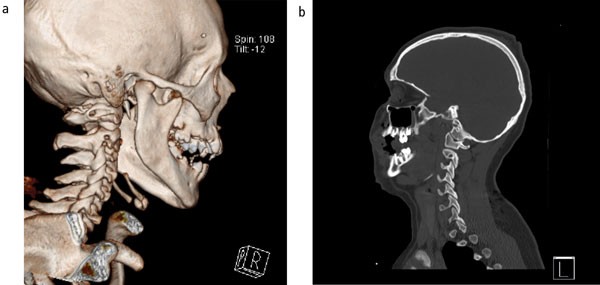
CT head scans showing fractures of 24, 25, 26 and 45, 46, 47
Figure 8 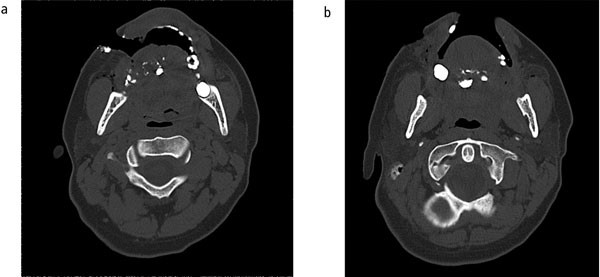
CT head scan showing through and through laceration of right cheek and ventral surface of tongue with radiopaque foreign bodies in tongue (tooth fragments)
Table 2 Injuries sustained by Case 2 -
His parents gave a past medical history of Asperger's syndrome and depression. They also reported regular attendance at the dentist and a good standard of oral health.



Immediate management
-
The patient was transferred to paediatric theatres as soon as space was available. He underwent surgical removal of shrapnel and debridement of puncture wounds from multiple sites including his right eye and cheek. An elective tracheostomy was performed to secure his airway in light of potential significant swelling of his tongue. A cast was placed on his left leg
-
The paediatric dental, plastics and maxillofacial teams worked together to surgically remove 16, 15, 14, 27, 47, 46, 45 and 37 which had comminuted coronal fractures. The tooth fragments were also removed from his tongue and lacerations to the left retromolar pad were sutured along with the mucosal layer of the wound on his right cheek. In addition the buccal mucosa was advanced over the sockets in the right maxilla to stabilise the dentoalveolar fracture
-
The submental wound was into subcutaneous tissues only and was debrided and dressed.
Intermediate management
-
The patient was reviewed by the paediatric dental team on the high dependency unit ten days after the incident; he was doing extremely well. He had been to theatre on two more occasions for further debridement and dressing of facial, oral, leg and neck wounds
-
He was able to speak through the tracheostomy and was starting to take food orally. He reported difficulty eating as he had no teeth on the right side and his tongue was painful on the left side where the shrapnel exited
-
Examination revealed the cheek wound had healed well intra and extra-orally, the sockets were granulating and the tongue was healing but was ragged on the left lateral border with evidence of trauma from his teeth. His oral hygiene was very good despite the stay in critical care
-
He requested replacement teeth on the right side as soon as possible to aid eating. It was explained that the sockets and tongue required further healing before impressions could be taken for partial dentures. He asked how he could speed up the healing process. This opportunity was taken to advise good oral hygiene including the use of chlorhexidine gel and 2,800 ppm fluoride toothpaste and to start eating soft foods initially
-
A goal was set for him to be sufficiently mobile to attend the dental health unit before the process of making dentures began. He was so motivated that he was actually discharged within three weeks of the incident before the appointment in the dental health unit was made
-
He was seen in the dental health unit 24 days after the incident and all sockets were healing well. His cheek and tongue were still tender and there had been loss of the sulcus in the upper right quadrant where the mucosal flap had been advanced (Fig. 9)
Figure 9 
Intra-oral photos of Case 2, 24 days post incident showing healing and loss of buccal sulcus in the upper right quadrant
-
An orthopantogram was taken (Fig. 10) which showed no root remnants remaining and no other pathology. Sensibility tests were carried out on the adjacent teeth and all responded positively. The patient was not able to tolerate impressions at this stage due to the discomfort in his cheek and tongue so a further appointment was made to coordinate with a plastic surgery outpatient appointment the following week
Figure 10 
OPG of Case 2, 24 days post incident
-
Over several appointments, all coordinated with other outpatient appointments, upper and lower partial dentures were fabricated. These were fitted two months after the initial injury (Fig. 11) and the patient was happy with the appearance but admitted that he was now used to eating without teeth on the right side.
Figure 11 
Photographs of Case 2 showing partial dentures in situ



Future treatment needs
The patient has recovered remarkably well from his injuries and has now been discharged from the majority of specialities involved in his care at RMCH. He will be followed up by the paediatric dental team with respect to the fit of his partial dentures and monitoring of the adjacent teeth in conjunction with his general dental practitioner. He appears to be managing both functionally and cosmetically despite the missing teeth but will be offered consultation with restorative dentists and implant-retained prosthetic teeth may be considered if he requests them.
Discussion
Although the maxillofacial team are not part of the major trauma team at CMFT this incident highlights the important role they play in managing the complex injuries sustained in an attack of this nature. As many of the patients in this incident were under 16 years old the paediatric dentist was vital in assessing dental injuries, deciding whether teeth could be saved and providing long-term rehabilitation and monitoring. For the two cases presented, replacement of the lost teeth was a significant step in their overall recovery and rehabilitation. Case 1 was not happy for others to see her without her front teeth . The promise of replacement teeth was also good motivation to get her eating. Case 2 was struggling to eat due to the loss of eight teeth and trauma to his tongue and cheek, the provision of partial dentures helped with function, although he has adapted well to life without these teeth.
Traumatic dental injuries are more difficult to manage in paediatric patients as they are still developing, so any restorations must be able to adapt to the changing oral environment. Permanent restorations, for example with implants, are not usually considered until growth has completed at approximately 16–21 years. Removable prostheses, which can be adjusted or replaced as the child grows and their occlusion changes, were therefore used as an interim measure in these cases. Movement of adjacent teeth and over-eruption of opposing teeth into the spaces were prevented by use of partial dentures with metal clasps and stops.
For teenage patients who had previously taken good care of their teeth, had not required orthodontic treatment and had little experience of dental treatment, wearing removable partial dentures for many years was not appealing. Both cases expressed some resentment about the situation they had been put in following the attack and the loss of their teeth had clearly had a big psychological impact on them. The role of the paediatric dental team was therefore to help with rehabilitation, regaining confidence, maintenance of the remaining teeth and managing the patient and family's expectations. Restorative dentists were involved from an early stage to give advice and reassurance to the families about the long-term options for replacement of the teeth and likely timeframes. It also allowed the teams to look at alternative options and the possibility of early placement of implants to minimise bone loss. Unfortunately, fractured teeth do not have the potential to remodel and heal as orthopaedic fractures or soft tissue wounds can. This will necessitate on-going dental management and maintenance of their edentulous spaces as they grow, long after other injuries have healed and they have been discharged from other specialities.
From a paediatric dental and maxillofacial surgery point of view, being involved in a major incident such as this has been a huge learning experience. It has enabled participation in a truly multidisciplinary team in both acute and long-term management, including trauma teams, CAMHS, plastic surgery, maxillofacial surgery, oral surgery, restorative dentistry, dietetics, physiotherapy, general surgery, orthopaedic surgery and anaesthetics. The importance of teeth and dental care, especially in paediatric patients, has been highlighted to all specialities and was demonstrated by presentation of these cases at an RMCH debrief two months after the incident.
Providing care for these young people from initial presentation onwards has been extremely rewarding. They both sustained multiple complex physical injuries requiring several prolonged surgeries under many different specialities. Moreover, they also have the profound psychological impact of being involved in such an incident and living with their life-changing injuries. Seeing them for regular appointments post-operatively, it is inspiring to witness their resilience both physically and mentally and this in turn helped to reinforce our own coping mechanisms following the incident.
Conclusion
The response to this incident has demonstrated that in such circumstances the inputs of paediatric dentistry are invaluable, not only in a remedial sense but also proactively promoting recovery in aspects not directly dentistry related – for example, psycho-socially and physically enabling nutrition. Despite other significant morbidity and injuries, dental health remained a constant concern for patients which highlights the importance of dental outcomes to people themselves. The work itself demonstrated the effectiveness of early intervention to mitigate potential longer term issues. The long-term management required for paediatric patients emphasised the need for effective planning to minimise GA exposure and out-patient appointment burden. Each patient suffered unique injuries requiring completely holistic and individual treatment plans. These had to take into account unusual injuries, growth and development, multiple other surgeries, life impact and time pressure as well as psychosocial trauma. As expected the incident in its scale and severity reinforced the need for effective MDT function to produce a coordinated holistic approach. Such teams therefore need to be prepared to accept dental input. While dental practitioners need to help them recognise the importance of dental health to their patients and recovery, and be able to integrate into teams where perhaps they are not normally present.
References
BBC. Manchester attack: What we know so far. 2017. Available from http://www.bbc.co.uk/news/uk-england-manchester-40008389 (accessed April 2018).
Telegraph Reporters. Manchester bomb made to kill as many as possible, inquest hears. The Telegraph, 2017. Available at https://www.telegraph.co.uk/news/2017/06/09/manchester-bomb-made-kill-many-possible-inquest-hears/ (accessed April 2018)..
Shuker S T . Facial Skin-Mucosal Biodynamic Blast Injuries and Management. J Oral Maxillofac Surg 2010; 68: 1818–1825.
Thompkins A . Blast Injuries. Royal College of Emergency Medicine. 2013. Available from https://www.rcemlearning.co.uk/references/blast-injuries/# (accessed April 2018).
Department of Health. NHS Emergency Planning Guidance 2005: Planning for the management of blast injured patients. Department of Health, 2007. Available at http://webarchive.nationalarchives.gov.uk/20080817111327/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081506 (accessed April 2018).
Katz-Sagi H, Gozal D, Ram D . Dental treatment of a 2 year old victim of a suicide bomb attack. Dent Traumatol 2007; 23: 318–321.
Gataa I S, Muassa Q H . Patterns of maxillofacial injuries caused by terrorist attacks in Iraq: restrospective study. Int J Oral Maxillofac Surg 2011; 40: 65–70.
Shuker S T . Maxillofacial blast injuries. J Craniomaxillofac Surg 1995; 23: 91–98.
Shuker S T . The effect of a blast on the mandible and teeth: transverse fractures and their management. Br J Oral Maxillofac Surg 2008 46: 547–551.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Timms, L., May, J. Bones heal, teeth don't! The involvement of dentists in the acute and long-term management of patients injured in the Manchester Arena Bomb. Br Dent J 224, 681–688 (2018). https://doi.org/10.1038/sj.bdj.2018.353
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2018.353
This article is cited by
-
Clarification
British Dental Journal (2018)
