
Key Points
-
The management of injuries is based on fast and accurate diagnosis.
-
General dental practitioners are likely to encounter traumatic injuries at any time.
-
This article acts as an aide-memoire for use in the acute setting to ensure that the correct initial management is carried out, thus ensuring the best possible long-term prognosis.
Abstract
The aesthetics of the mouth are important in determining overall facial attractiveness. People with a relatively normal dental appearance are perceived as more attractive, more intelligent and more desirable as friends.1 Although the oral region comprises only 1% of the body area it accounts for 5% of all bodily injuries, and of facial injuries, dental injuries are the most common.2 A US survey among people aged 6-50 years showed that 1 in 4 had evidence of dental trauma.3
Similar content being viewed by others



Introduction
The aetiology of dentoalveolar trauma in adults can be categorised as: accidental trips and falls; sports injuries; and road traffic accidents. The energy of the impact is of great significance in terms of the extent of the damage caused. Low-velocity blows are more likely to cause more damage to the supporting structures with less incidence of tooth fracture. In contrast, high-velocity impacts deliver greater energy to the crown, resulting in crown fractures with less effect on the supporting tissues. The surface area of contact, and the shape and resilience of the traumatic object can also affect the pattern of injury. Sharp objects deliver a particularly concentrated force, often resulting in crown fractures. Conversely, blunter objects with overlying soft tissue tend to deliver dissipated forces, resulting in root fractures, luxation injuries or injury to the supporting tissues.4
History
A thorough history is paramount to understand the injury and deliver the correct care within a suitable time frame. This is especially relevant in patients with avulsed or pulpally exposed teeth. Table 1 shows the relevant questions dentists should ask when taking an acute trauma history, and highlights their clinical value.1
Examination
A patient involved in a traumatic episode must be thoroughly checked for any evidence of serious concomitant injuries, including head and cervical spine injuries. If there is any doubt as to whether the patient has lost consciousness or if the patient is displaying any associated signs (eg loss of memory, drowsiness or nausea) an immediate referral to an accident and emergency department is indicated.
A detailed examination is needed together with accurate recording of the information obtained. Radiographs and clinical photographs are invaluable to record the injuries and assess follow-up treatment in the long term, and may provide forensic evidence if there are any medico-legal consequences.
Extraoral examination
A diagrammatic representation of any abrasions, bruises, lacerations, sutured lacerations, circumorbital ecchymosis and subconjunctival haemorrhages evident extraorally should be documented with a sketch or using a preprinted outline, as shown in Fig. 1, as well as taking clinical photographs if possible.

Diagrammatic representation of injuries on the face
Soft tissue injuries include:1
-
Abrasions – injuries to the skin that remove the epithelial layer, and may be bleeding and painful owing to the exposed nerve endings.
-
Bruising – an area of haemorrhage caused by the leakage of blood from ruptured subcutaneous vessels into surrounding tissues, following a blunt impact; there is no break in the overlying skin, but it may be associated with an underlying bone fracture.
-
Lacerations – splitting or tearing of the skin caused by sharp objects and should be noted even if they have already been sutured in an accident and emergency department.
Wounds need to be examined with care and accuracy for foreign bodies such as tooth fragments, glass and grit. Cleaning the wound will aid visualisation and may be carried out using gauze and saline. In some circumstances, more vigorous cleaning under local or general anaesthetic may be necessary. Residual debris in the soft tissue can result in disfiguring scarring and tattooing.
Circumorbital ecchymosis and subconjunctival haemorrhages may be signs suggestive of facial fractures, and the infraorbital margins should be assessed for a step deformity. If present or if in doubt, an appropriate referral should be made to an oral and maxillofacial team.
Intraoral examination
The 2003 UK Child dental health survey5 found 5% of 8-year-olds had sustained some trauma to their upper permanent teeth. The degree of overjet increases the risk of trauma to the upper incisors. Forty-five percent of UK children with an overjet of greater than 9 mm had experienced dental trauma by the age of 12 years.
After assessing the facial soft tissues, the lips and oral mucosa should be examined in detail, beginning with a general examination and working to a specific assessment of the injured areas.
Soft tissue assessment
Injuries to the lips
The dentition is protected by the lips, which act to absorb trauma energy, thus reducing injuries to the teeth. A through-and-through defect in the lip sulcus may be indicative of retained tooth fragments. The tooth or teeth are thought to penetrate the full thickness of the lip, and then fracture on impact against a hard surface. The resulting broken fragments re-enter the exit wound and are retained in thesoft tissue of the lip.4
It is imperative for the clinician to carefully inspect all wounds and lacerations of the perioral region and determine whether any foreign bodies are present. Through-and-through lacerations are easily overlooked, as are small foreign bodies and tooth fragments. Soft tissues should be systematically examined and explored, under local anaesthesia if needed. Cleaning and debridement of the lips is important to prevent infection, fibrosis and tattooing.
Soft tissue radiographs taken at a reduced exposure may be indicated to identify tooth fragments or foreign bodies within the soft tissues. Figure 2a shows a lateral radiograph taken at a reduced exposure of a patient's lips, showing tooth fragments present, and Fig. 2b shows the tooth fragment removed from the lip.

(a) Lateral soft tissue view showing tooth fragments in the upper lip; (b) Retrieved fragment of tooth
All missing teeth and fragments need to be accounted for wherever possible. Occasionally, this is not possible and the clinician must then make a judgement as to whether to refer the patient for a radiograph of the chest.
Injuries to the buccal mucosa
Most lacerations and abrasions of the buccal mucosa heal quickly and do not require suturing. Large lacerations (>1–2 cm) should generally be repaired using resorbable 4-0 sutures. If deep, a two-layer closure can be performed. Through-and-through lacerations can be more difficult to manage. In cases where extensive lacerations are present and may involve the salivary ducts (Wharton's and Stensen's) or the facial nerve, an urgent referral to an oral and maxillofacial team should be made.
Injuries to the gingiva
Bleeding around the gingival margins (Fig. 3) may indicate damage to the periodontal ligament, for example, with a subluxation injury. Figure 3 shows tooth 21 with visible bleeding at the gingival margin.

Gingival bleeding associated with tooth 21, suggestive of a subluxation injury
Small lacerations over the maxillary or mandibular gingiva usually heal uneventfully without intervention. If the laceration is large and gaping, or there is bone exposed or a flap present, the edges should be approximated with 4-0 resorbable sutures. Occasionally, difficulty is encountered repairing gingival tears owing to a shortage of tissue; in such cases, the adjacent teeth can be used as 'anchors' by wrapping the suture around them. Gingival lacerations may also overlie bone fractures, as discussed later in this chapter.
Injuries to the fraenum
The maxillary fraenum rarely requires sutures for simple lacerations, but more complex lacerations extending into the surrounding mucosa or gingiva should be approximated with absorbable suture material. These wounds are painful and, even if suturing is not required, analgesia may need to be prescribed in many cases. The lingual fraenum is very vascular in nature and may require suturing to control the bleeding.
Injuries to the tongue
Most tongue lacerations <1 cm without gaping wound edges may not require repair. Lacerations that gape need suturing, as the cleft left by the non-repaired wound can re-epithelialise, leaving a grooved or bifid appearance for some time after the injury, although these defects virtually always regress spontaneously with the passage of time. Immobilisation of the tongue by an assistant allows easier repair.
As with all procedures, explaining the procedure to the patient in detail before proceeding is important for consent as well as for managing patient expectations and ensuring cooperation. Repair should be carried out under anaesthesia by local infiltration, which also aids haemostasis. Deep lacerations require a layered closure with deep stitches approximating the muscle layer with buried knots, followed by sutures on the surface of the tongue. Full-thickness lacerations should be managed in layers from both the dorsal and ventral surface of the tongue.
Hard tissue assessment
The teeth are better assessed after cleaning away any blood and debris. As mentioned earlier, it is important to remember that soft tissue injuries can often overlie bony injuries. Figure 4 shows extensive haemorrhage lingually associated with a dentoalveolar fracture.

Extensive haemorrhage lingually associated with a dentoalveolar fracture
Luxation
Injuries to teeth rarely occur in isolation and polytrauma is often seen in individual teeth. The following luxation (displacement) injuries can occur and are described in greater detail at www.dentaltraumaguide.org. The position of displaced teeth should be noted accurately and can be noted in relation to adjacent teeth.
A concussion injury is a mild injury to the periodontal ligament without any loosening or displacement of the tooth, and the tooth may be tender. The long-term prognosis should be good with vitality maintained.
Subluxation is a mild–moderate injury to the periodontal ligament without displacement but with some loosening of the tooth. The long-term prognosis should be good with vitality maintained. Bleeding around the gingival margin is indicative of this injury, as seen in Fig. 3.
Extrusive luxation (Fig. 5a) is the partial displacement of a tooth out of the socket in an axial direction. These teeth may maintain their vitality depending on whether the neurovascular bundle is severed or not. It is therefore advisable to review them and only start root canal treatment if there are two signs or symptoms of non-vitality, such as periapical rarefaction, discoloration or lack of response to sensibility testing.

d: Avulsion of teeth 31 and 32 presenting 2 days after injury
Lateral luxation (Fig. 5b) involves displacement of the tooth palatally or labially and is almost always associated with a dentoalveolar fracture. With this type of injury, there is a high risk of pulp necrosis. Again, it is advisable to review them and only start root canal treatment if there are two signs or symptoms of non-vitality.
Intrusive luxation (Fig. 5c) involves displacement of a tooth further into the socket in an axial direction. Crushing of the neurovascular bundle occurs, resulting in the loss of vitality in teeth with closed apices. Severe damage usually also occurs to the bony alveolar socket.
Avulsion injury (Fig. 5d) is the total displacement of a tooth out of the socket, which may be associated with damage to the alveolar bone and adjacent teeth. With closed apices, pulp extirpation within 7–10 days is essential. For more details, visit www.dentaltraumaguide.org.
Fractures
Damage to the teeth can vary from a crack in the enamel (infraction), to a complicated root fracture with exposure of the pulp. Infractions (Fig. 6a) are incomplete fracture lines that may be visible on the surface of the tooth, particularly when viewed under transillumination. They can be asymptomatic; however, they can lead to bacterial ingress owing to the difficulty in predicting the depth of the fracture lines.

(a) Enamel infractions visible on 12, 21 and 22, as well as an enamel–dentine fracture and the mesial aspect of the 12 and 22; (b) Enamel fracture of tooth 41 and 42; (c) Enamel–dentine (uncomplicated) crown fractures of 21
Enamel fractures (Fig. 6b) are confined within the enamel and are usually asymptomatic, but resultant sharp edges can result in soft tissue irritation. Despite being asymptomatic the appearance of these injuries usually prompts treatment by patients.
Enamel–dentine uncomplicated fractures (Fig. 6c) involve the sensitive dentine layer. Rapid coverage of the dentine layer will prevent bacterial invasion into the dentinal tubules, which can lead to pulpal necrosis. Although composite is the ideal restorative material, if multiple injuries are present a glass ionomer bandage may be applied for coverage in the emergency management. Deeper fractures may show the pulp shining through as pink if a thin layer of dentine remains over the pulp.
Enamel–dentine–pulpal fractures (Fig. 6d) involving the pulp and pinpoint exposures can be treated by pulp capping; however, larger exposures will require a pulpotomy (traditionally called a Cvek pulpotomy).
Crown–root fractures vary in presentation depending on the level of the root fracture and whether there is pulpal exposure or not.
If tooth mobility is detected, this may be due to a subluxation injury, a root fracture, a crown–root fracture or a dentoalveolar fracture, particularly when a group of teeth move en bloc when one tooth is examined. Crown–root fractures are usually caused by direct trauma in the anterior teeth, with the fracture lines often extending obliquely from the labial surface into the palatal gingival crevice (Fig. 6e). Posterior crown–root fractures occur due to forced biting together by a blow to the chin, for example, and may result in fractured cusps. These are often not displaced owing to the fractured segment being held in place by periodontal fibres, and on first examination can be missed.
Root fractures are a relatively uncommon dental injury, especially in younger age groups, owing to the elasticity of the alveolar bone. Clinical presentation is dependent on the level of the root fracture, which can be apical, middle (Fig. 7a) or cervical (Fig. 7b), and may present with varying mobility. Accurate diagnosis is based on radiographic assessment using periapical and upper occlusal views.

(a) Middle root fracture of tooth 12 and apical fracture of tooth 21; (b) Cervical root fracture of tooth 22
Assessment of the occlusion
A change in the occlusion is often associated with displaced teeth. If further examination reveals mobility in a whole tooth-bearing segment, rather than individual teeth, a dentoalveolar fracture should be suspected. Smaller alveolar fractures can occur around the sockets, especially of avulsed teeth, and this can make replantation difficult. Gentle pressure on the socket wall labially using finger pressure will help reposition the fragment prior to replantation of a tooth.
In an acutely traumatised patient, there is little benefit in tapping the teeth to check for tenderness to percussion. This sign is important at follow-up appointments when assessing the sensibility status of the teeth. On rare occasions when it is not possible to decide whether a tooth has been intruded, light tapping may help diagnosis if a metallic sound is elicited.
It is important that fractured teeth are restored as soon as possible and avulsed teeth replanted immediately, otherwise in the longer term, secondary changes to the occlusion may occur through over-eruption of the opposing teeth.
Sensibility tests
These act as a baseline for assessing pulpal status, not especially at the time of injury but more in the longer term. While electric and thermal testing assess the response of the nerve supply of the tooth, it is important to understand that neural regeneration occurs more slowly than vascular regeneration (which is more important) and on occasion may not occur at all.6,7 In an ideal world laser Doppler flowmetry, which assesses the blood supply of the pulp, would be a more significant test but it is not readily available and therefore not yet routinely used.
Radiographs
Radiographs are essential in the assessment of traumatised teeth to aid diagnosis. Multiple views at different angles may be indicated, particularly in cases of extensive trauma and involvement of multiple teeth. The International Association of Dental Traumatology (IADT) recommends radiographs be taken based on the clinical assessment, and the views that may be helpful are:
-
Periapical radiograph with a 90° horizontal angle with central beam through the tooth in question
-
Periapical radiograph with lateral angulations from the mesial or distal aspect of the tooth in question
-
Occlusal view (particularly useful in root fractures).
Root fractures are often not obvious on periapical radiographs. As seen in Fig. 8, the fracture line is only clearly observed when the central beam passes through the fracture line. If the central X-ray beam is within 15-20° of the fracture line, fractures may not be detected at all,8 so if a root fracture is suspected, a second view may be indicated.
Radiographs should be evaluated for:
-
Stage of root development
-
Increase or decrease in the periodontal ligament space (widening in extrusion and loss of space in intrusion injuries)
-
Root fractures (position and direction)
-
Pulp canal obliteration (indicative of previous trauma)
-
Bone fractures
-
Displacement injuries
-
Foreign bodies in the soft tissues.
Radiographs are also invaluable in the long-term monitoring of traumatised teeth. The use of cone-beam CT scanning technology is an exciting alternative to two-dimensional views to aid diagnosis and guide subsequent management of dental trauma.
Management
Early treatment of traumatic injuries helps maximise long-term outcomes. Rapid replantation of avulsed teeth and correct storage of tooth fragments and avulsed teeth can aid long-term outcomes. Dental trauma is often complex, with concurrent injuries to other teeth and multiple injuries to teeth. Patients often arrive in pain and can be distressed. Reassurance, good anaesthesia and debridement of soft tissue wounds help manage the situation. The practitioner must be vigilant for non-dental injuries, including head injuries, and must be able to identify signs of non-accidental injuries. Prescription of antibiotics should be done with care, and depends on the clinical situation and the patients' medical status.
The IADT has published guidelines for the management of a variety of traumatic dental injuries9,10 and a comprehensive account can be found at www.dentaltraumaguide.org.
Luxation injuries
Luxation injuries are the result of tearing of the periodontal fibres on one side of the socket and compression of the fibres on another side. Pulpal necrosis is reported in 15–59%1 of cases, and depends primarily on the type of injury and the stage of root development. The greatest incidence of necrosis is seen in intrusion injuries, followed by lateral luxation and extrusion injuries. The management of luxation injuries is detailed extensively on the IADT website and is summarised in Table 2.
Avulsion injuries
Avulsion has been reported in 1-16% of dental injuries.11 Outcomes are largely dependent upon the storage medium of the avulsed tooth, the extraoral dry time, the stage of root formation and the time from the incident to re-implantation. Prompt treatment of this dental emergency is required for best outcomes. Replantation is the treatment of choice for permanent teeth, as soon as possible after the injury. Figure 9a shows avulsion of tooth 11 and lateral luxation of tooth 12. Replacement of the 11 can be seen in Fig. 9b, avoiding any handling of the root and support is provided by placement of a composite wire splint as seen in Fig. 9c. Table 3 shows the treatment recommended by the IADT for avulsed teeth.10

(a) Avulsion of tooth 11 and lateral luxation of tooth 12; (b) replantation of avulsed tooth, handled by the crown only; (c) repositioned teeth stabilised with a wire and composite splint
Replantation of mature teeth that have an extraoral dry time >60 minutes is to promote alveolar bone growth. Bony encapsulation of the tooth is desirable, followed by ankylosis and resorption. The crown can be removed when the tooth shows evidence of submergence at 1 mm, the aim being to maintain the alveolar contour.
Alveolar fractures
Fractures of the alveolar bone usually occur in combination with other tooth tissue trauma. Alveolar fractures can be classified as:
-
Fracture of the socket wall
-
Comminuted fracture of the socket
-
Segmental dentoalveolar fracture
-
Fracture of the mandible or maxilla.
Dentoalveolar fracture lines crossing the roots of teeth may simulate a root fracture and can be difficult to discern on a radiograph. The use of different radiographic views can allow clinicians to trace the continuity of root canals and root surfaces, allowing the fractured tissue to be identified.
Dentoalveolar fractures can be seen associated with the following signs:
-
Disruption in the occlusion
-
Bruising of the attached gingiva
-
Mobility of one or more teeth, with en bloc movement of a few teeth when checking the mobility of a single tooth
-
Laceration of the gingivae overlying the fracture line.
Dentoalveolar injuries are often complex, with concurrent displacement injuries to the teeth contained within the fracture. Thus gingival, pulpal and periodontal injuries may also be present.
Treatment guidelines for dentoalveolar fractures are shown in Table 4. Repositioning of the teeth should be carried out under local anaesthetic. The root apices are often locked into the bone and need to be disengaged using digital pressure. Correct positioning of the teeth will also correctly position the alveolar bone fragment. If the fracture is open and comminuted, with loose fragments unattached to the periosteum, these may have to be removed to aid repositioning. If extractions are needed, they should be delayed until after bone healing. The presence of teeth provides stability to the fragment, and early removal can risk further damage to the already mobile segment. As with all trauma cases, infection is a risk when the periodontal ligament, bone and dental pulps are exposed. Antibiotics are usually prescribed in these cases along with strict oral hygiene advice and a soft diet. Sequestration of bone and teeth is rare but can occur in cases of dentoalveolar fracture.
Crown fractures
Immediate treatment is targeted towards maintenance of pulpal vitality and prevention of bacterial ingress into the dentinal tubules. Table 5 shows the recommended treatment for these injuries depending on the depth of fracture and whether pulp tissue is exposed or not. In complicated crown fractures, partial (Cvek) pulpotomy can be successful, with hard tissue barrier formation in up to 96% of cases.12 If possible, fracture segments should be retained and reattached as soon as possible.
Root fracture injuries
A root fracture is a fracture confined to the root of the tooth involving cementum, dentine and the pulp. Root fractures are classified by location and may be in the horizontal or oblique plane in the apical third, mid-third or cervical-third (see Fig. 7). They are caused by a high impact blunt trauma to the crown of a tooth and often can be difficult to visualise radiographically. The traumatic incident results in separation of the periodontal ligament and exposure of the root surface. The diagnosis, clinical features and management of root fracture injuries is summarised in Table 6.
Prognosis for traumatised teeth
The long-term prognosis for injured teeth is dependent on various factors at the time of the incident:
-
Age of patient and degree of root formation and apical closure
-
Amount of exposed dentine and pulp
-
Time interval between injury and treatment
-
Degree of contamination
-
Periodontal injury
-
Level of patient cooperation.
Pulpal necrosis and periapical infection are related to the time between injury and fixation. Teeth repositioned within 1 hour are less likely to undergo pulpal necrosis.13 If more than 48 hours elapse between injury and treatment, then the incidence of later pulpal necrosis is greater.14 If the apex of the tooth is in the line of the fracture, the risk of pulpal necrosis is also increased. Open reduction and internal fixation of dentoalveolar fractures also increases the risk of necrosis of the teeth in the fracture segment and adjacent teeth. Thus composite and wire splinting or arch bar placement is preferred. Root canal obliteration is a more common sequel in people aged under 20 years, and marginal bone loss is seen if the bone segments are not properly aligned.
Splinting
Splinting of traumatised teeth stabilises the teeth and provides comfort for the patient. Splints should be flexible (semi-rigid) to allow normal physiological movements of the tooth within the periodontium in all cases except cervical-third root fractures. The lengths of time recommended by the IADT for splinting various injuries are shown in Table 7.
Many types of splint and techniques are available:
-
Acid-etched orthodontic wire and composite splinting is the most common: the authors use 018 stainless steel wire for flexible splinting, as shown in Figure 10
Figure 10 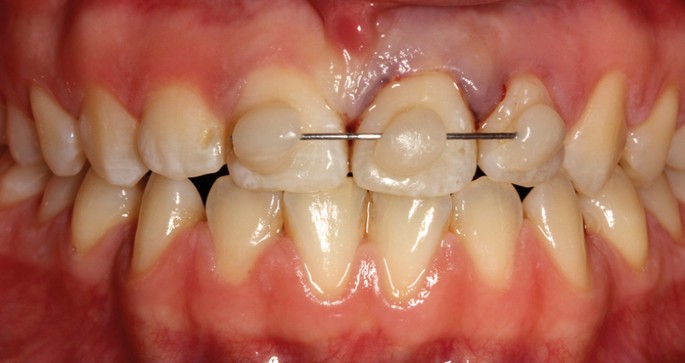
Orthodontic wire and composite splint extending from 11 to 22
-
A titanium trauma splint is an alternative, pre-fabricated splint with ease of manipulation over the surfaces of the teeth and is shown in Figure 11.
Figure 11 
Titanium trauma splint and composite splint extending from 12 to 21


In all cases of dental trauma, a soft diet is indicated for up to 2 weeks. Toothbrushing after every meal is recommended with a soft toothbrush, as well as twice-daily mouth washing with 0.1% chlorhexidine in the presence of soft tissue damage. All traumatised teeth need to be monitored in the long term.
Prevention
Prevention is always better than cure, and the American Dental Association recommends that anyone who participates in a sport that carries a significant risk of injury should wear a mouth guard for protection. These must not only fit well and stay securely in the mouth during activity but also should be comfortable and allow the wearer to breathe and talk. There are three types:
Over-the-counter mouth guards
These come ready to wear and are relatively inexpensive, but do not give a perfect fit and protection is therefore compromised. As a result, they are not suitable for contact sports.
'Boil and bite' mouth guards
These are marginally better than the previous type as the fit is slightly better, but they do not confer adequate protection.
Dentist-made mouth guards
These are made to fit the wearer's mouth and teeth with adequate soft and sometimes hard acrylic to make them most effective at protecting the oral cavity during contact sports. They can be single jaw or bimaxillary in design, and bimaxillary mouth guards have been shown to be the most effective.15 Dentist-made mouth guards are more expensive but considering the biological cost often seen in traumatic dental injuries, the extra cost is probably worth the investment.
In conclusion, the aetiology of dentoalveolar trauma is multifactorial and not seen often enough to develop confidence and expertise in its management. Early intervention is essential for optimising the long-term outcome and improving the prognosis for the teeth affected.
References
Andreasen J O, Andreasen F, Andreasen L . Textbook and colour atlas of traumatic dental injuries to the teeth. 4th ed. pp. 197–206. Oxford: Munksgaard, 2007.
Petersson E E, Andreasen L, Sorensen S . Traumatic oral vs non-oral injuries. Swed Dent J 1997; 21: 55–68.
Kaste L M, Gift H C, Bhat M, Swango P A . Prevalence of incisor trauma in persons 6 to 50 years of age: United States, 1988-1991. J Dent Res 1996; 75: 696–705.
Andreasen J O . Aetiology and pathogenesis of traumatic dental injuries. A clinical study of 1298 cases. Scand J Dent Res 1970; 78: 339–342.
Office of National Statistics. Children's dental health in the United Kingdom, 2003. http://www.ons.gov.uk/ons/guide-method/method-quality/specific/health-methodology/dental-health/dental-health-of-children. ONS, 2008 (accessed 25 November 2014).
Schendel K U, Schwartz O, Andreasen J O, Hoffmeister B . Reinnervation of autotransplanted teeth. A histological investigation in monkeys. Int J Oral Maxillofac Surg 1990; 19: 247–249.
Cvek M, Granath L, Cleaton-Jones P, Austin J . Hard tissue barrier formation in pulpotomized monkey teeth capped with cyanoacrylate or calcium hydroxide for 10 and 60 minutes. J Dent Res 1987; 66: 1166–1174.
Bender I B, Freidland J B . Clinical considerations in the diagnosis and treatment of intra-alveolar root fractures. J Am Dent Assoc 1983; 107: 595–600.
Flores M T, Andersson L, Andreasen J O et al. Guidelines for the management of traumatic dental injuries. I. Fractures and luxations of permanent teeth. Dent Traumatol 2007; 23: 66–71.
Flores M T, Andersson L, Andreasen J O et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol 2007; 23: 130–136.
Andreasen J O . Fractures of the alveolar process of the jaw. A clinical and radiographic follow-up study. Scand J Dent Res 1970; 78: 263–272.
Cvek M . A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endodont 1978; 8: 232–237.
Oikarinen K, Lahti J, Raustia A M . Prognosis of permanent teeth in the line of mandibular fractures. Endod Dent Traumatol 1990; 6: 177–182.
Glendor U, Halling A, Andersson L, Eilert-Petersson E. Incidence of traumatic tooth injuries in children and adolescents in the county of Västmanland, Sweden. Swed Dent J 1996; 20: 15–28.
Jagger R G, Milward P J . The bimaxillary mouthguard. Br Dent J 1995; 178: 31–32.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Tagar, H., Djemal, S. Oral surgery II: Part 1. Acute management of dentoalveolar trauma. Br Dent J 223, 407–416 (2017). https://doi.org/10.1038/sj.bdj.2017.805
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.805
