
Key Points
-
Investigates the areas for improvement in the information given to patients requiring emergency dental care during out of hours periods.
-
Suggests essential information to be included in practice websites or voicemails.
-
Suggests future research could benefit from surveying patients attending A&E with dental problems.
Abstract
Objective To perform an evaluation of the information given to patients seeking emergency dental services during out-of-hours periods in Greater Manchester.
Method This is a cross-sectional study. A list of all NHS dental practices in Greater Manchester was obtained from the NHS website. The investigators then accessed websites and voicemails of all practices to assess the information given to patients.
Results The study shows that most practices have voicemail, which includes varying information on how to access emergency dental services during out-of-hours periods. Few of those included advice on the management of common dental emergencies. On the other hand, the majority of practices did not have websites. From those who included advice on how to access emergency dental services during out-of-hours periods on how to manage common dental emergencies on their websites, the information was easy to find.
Conclusion The current information could be improved by ensuring the inclusion of essential details. Websites would help by including more details. In turn, this could help to reduce the number of inappropriate presentations to A&E departments.
Similar content being viewed by others

Introduction
Emergency dental services (EDS) could be defined as 'care that cannot be foreseen or planned in advance of contact with the relevant healthcare and the patient is assessed as requiring immediate treatment'.1 Most patients using this service present with pain due to pulpal pathology, facial swelling and pericoronitis.1,2 Common treatments offered in such services include: dental extractions, temporary dressings and a prescription for antibiotics.3 This service is available for both regular and irregular attendees.
In terms of accessibility, previous research has demonstrated that most patients found out about the service from family and friends; however, only a few were advised by the receptionist in their regular practice.4 The lack of publicity has resulted in more patients seeking help from their general practitioner (GP) or accident and emergency (A&E) department in their local hospital, which could significantly waste resources.5,6,7,8 This inappropriate presentation could also be attributed to the fact that patients are not charged for their visits to the GP or A&E, compared to the charged service when visiting the dentist. In a previous study, it was shown that 40% of patients found it difficult to contact their dentist or find the out-of-hours dentist number when the surgery was closed. They thought that this area could be improved.9 This has been shown to be the main cause of patients' dissatisfaction with the service.5 To improve the efficiency of this service and avoid inappropriate visits to the GP or A&E, the EDS should be clearly publicised.10 A practical means of achieving such efficiency would be to enrich the website with relevant out-of-hours information and/or to record a clear and understandable voicemail message.
The following is a cross-sectional study investigating the adequacy and clarity of information given to patients using voicemail and website on the dental practice's out of hours services and protocols.
Materials and methods
A list of all NHS dental practices in Greater Manchester was obtained from NHS choices website (http://www.nhs.uk) using the 'Services near you' option and searching for dentists with Greater Manchester as the location for the search criteria. The list was accessed on 26 March, 2016 and saved to avoid any alterations during the time of data collection. Two data collection sheets were designed, one for over-the-phone information and the other for online information. All practices were called on Saturday or Sunday between 22.00 and 00.00 as this is considered an out-of-hours period. The investigator listened to the voicemail and recorded the information given to patients during out-of-hours periods. The websites, on the other hand, were accessed at random times at the researcher's convenience. This was carried out over the course of ten weeks.
All collected data were transferred to SPSS and analysed.
Results
The search yielded 916 NHS practices in Greater Manchester. All practices had a phone number available on the NHS choices website. With regards to the websites, multiple branches of the same practice were accounted for, only 605 practices out of the 916 were analysed.
Of the practices, 18.6% (N = 170) did not have voicemail, while 64.2% (N = 389) did not have websites. Different pieces of information given by voicemail are summarised in Table 1, Table 2 and Table 3.
The majority of practices (90.2%, N = 195) included their opening hours on their website. This is also true for out-of-hours contact details, which was included in 69.9% (N = 151) of the websites.
Of the practices, 73.5% (N = 111) that included out-of-hours contact details on their website placed them following one hyperlink, while 21.1% (N = 32) had them on the main page. The remaining practices (5.2%, N = 8) used two hyperlinks to reach the out-of-hours contact details.
Out-of-hours contact details given over voicemail and websites are summarised in Table 4 and Table 5, respectively.
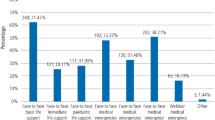
Out of the 18 dental practices that offered advice on common dental emergencies via voicemail, 12 practices had advice on management of post-operative haemorrhage. Of these, two gave advice on fixing loose brackets and three offered advice on pain management. The remaining six practices gave advice on pain management only. None of the practices gave advice on trauma.
On the other hand, this advice was included in 16.6% (N = 36) of the websites out of the total 216 practices that actually had websites. Those pieces of advice were easy to find on 75% (N = 27) of websites by following one hyperlink. The remaining 25% is split equally between finding the information on the main page or following two hyperlinks. Table 6 summarises the advice given for common dental emergencies on the websites.
Some websites or voicemails will have multiple out-of-hours contact details and various advice on management of common dental emergencies. Therefore, the total number in the table will exceed the number of practices offering out-of-hours contact or emergency advice.
Discussion
The results show that information given to patients via out-of-hours voicemail or on websites varies between practices. Websites showed far more detailed advice, than voicemail and it was relatively easy to find. Unfortunately, most practices did not have websites. Another finding was that some practices need to update their details on the NHS choices website as their phone number was incorrect.
Although the dental 'registration' process has been abolished since the introduction of the 2006 dental contract, patients might prefer to contact their regular dentist for an emergency. Some patients might be willing to wait until the practice next opens if they knew that they would be able to speak to or even be seen by a clinician soon. Therefore, details of the practice's opening hours are important to include in out-of-hours advice. Patients might also need reassurance or be unaware of simple management measures. This could be incorporated in the voicemail and website. This is especially important for post-operative bleeding or pain, as some patients might not be aware of such complications following dental treatment. As such, websites would be more helpful if they were more informative. Some pieces of given advice could potentially reassure patients and help them manage the situation until they see their dentist or emergency dentist. Unfortunately, some practices advise patients to seek help from A&E or 999 in case of an emergency without specifying which emergency requires urgent medical attention. As a result, this could lead to an unnecessarily long waiting time in the emergency department. Advertising the NHS non-emergency number (111) might help reduce the pressure on A&E departments. Experienced nurses and paramedics would be able to assess patients over the phone and advise them on management, direct them to out of hours EDS, or instruct them to visit an A&E department if deemed necessary. The NHS Choices website also has a dedicated page on accessing urgent dental care (http://www.nhs.uk/chq/pages/1776.aspx?categoryid=74).
The authors hereby suggest the inclusion of the following in voicemail messages and on websites for effective management of out-of-hours dental emergencies:
-
Practice's opening hours
-
Number of regional out of hours EDS
-
The NHS non-emergency number (111)
-
Management of post-operative bleeding, pain of dental origin and avulsion
-
When to seek immediate medical advice
-
Nearest A&E department.
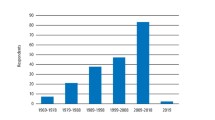
One limitation of this study is that it only surveyed practices in one region at a particular point of time. Another consideration is the effect of the 2006 contract on the number of inappropriate presentation to A&E for dental problems. Most of the studies quoted in this article were conducted before the introduction of the 2006 NHS General Dental Services contract. The new contract has capped the charge for dental emergency services to a fixed amount, rather than a fee per item of service basis. Therefore, this may have influenced patients' attitude towards seeking A&E for dental emergencies. More recently, a single-centre retrospective study attempted to investigate the effect of this contract. They found that in the period between 2004–2013, there was a significant increase in the number of dental-related issues presenting to A&E.11 It was not clear, however, if this increase was in true emergencies, which may be the result of irregular dental visits, or an increase in inappropriate presentations owing to the lack of awareness of the EDS. Future research could also survey the reason of A&E presentation for dental problems rather than the EDS, from the patients' perspective.
Conclusion
In conclusion, this study implicates the need for and benefit of improving information supplied by NHS dental practices in Greater Manchester on out-of-hours emergency dental services; this includes both voicemail- and website-accessed advice. Inappropriate presentation to A&E with dental-related problems is a multifactorial issue, exploration of the reasons leading to such presentation is out of the scope of this article. Nevertheless, adequate and accurate information given to patients on the management of out-of-hours dental emergencies is one of the contributing factors that could help in the reduction of such problems. Subsequently, this may aid in curtailing waiting times in the department.
The authors suggest relaying certain information through different means to patients as a minimum requirement for effective management of out-of-hours dental emergencies.
References
SDCEP, Emergency Dental Care. Scottish Dental Clinical Effectiveness Programme: Dundee, 2007.
Sinclair J, Wilson N H . An emergency dental service for students: 4year findings. Community Dent Hlth 1997; 14: 89–91.
Rehman K.U . Emergency dental services: review of the Community Heath NHS Trust Service in Birmingham between 1997 and 2000. Prim Dent Care 2003; 10: 93–96.
Austin R, Jones K, Wright D, Donaldson N, Gallagher J E . Use of the outofhours emergency dental service at two south-east London hospitals. BMC Oral Health 2009; 9: 1.
Anderson R . and D W. Thomas . Public Dental Health: Outofhours dental services: a survey of current provision in the United Kingdom. Br Dent J 2000; 188: 269–274.
Dickinson T M . and P G. Guest . An audit of demand and provision of emergency dental treatment. Br Dent J 1996; 181: 86–87.
Pennycook A, Makower R, Brewer A, Moulton C, Crawford R . The management of dental problems presenting to an accident and emergency department. J Royal Soc Med 1993; 86: 702–703.
Anderson R, Richmond S, Thomas D W . Patient presentation at medical practices with dental problems: an analysis of the 1996 General Practice Morbidity Database for Wales. Br Dent J 1999; 186: 297–300.
Anderson R, Thomas D W, Phillips C J . The effectiveness of outofhours dental services: II. patient satisfaction. Br Dent J 2005; 198: 151–156.
Anderson R, Thomas D W, Phillips C J . The effectiveness of outofhours dental services: I. pain relief and oral health outcome. Br Dent J 2005; 198: 91–97.
Patton C . and A. Dickenson . Acute Dental Conditions Attending A&E: Is there an epidemic of surgical admissions for dental infections? Br J Oral Max Surg 2014; 52: e102.
Acknowledgements
The authors acknowledge the guidance of Dr Lesley Taylor, Postgraduate Tutor, Welsh Deanery and a Dento-legal Adviser, Dental Defence Union.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Aldallal, S., Aldallal, F. & Khajah, A. Adequacy and clarity of information on out-of-hours emergency dental services at Greater Manchester NHS dental practices: a cross-sectional study. Br Dent J 222, 463–465 (2017). https://doi.org/10.1038/sj.bdj.2017.270
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.270
