
Key Points
-
Highlights that there has been little change in reported attendance patterns since the 2003 survey.
-
Highlights oral health inequalities in the survey population that require continued action.
-
Notes that family deprivation negatively influenced dental attendance for regular check-ups.
-
Emphasises that most parents reported overall satisfaction with the last dental practice their child had visited.
Abstract
Background The 2013 Children's Dental Health survey is the fifth in a series of national surveys.
Aims This paper describes children's reported use of dental services, their experience of receiving dental treatment and parental satisfaction with services.
Methodology A representative sample of children (aged 5, 8, 12 and 15 years) in England, Wales and Northern Ireland were invited to participate in dental examinations. Older children and all parents were invited to complete a questionnaire about oral health behaviours and attitudes.
Results Over 80% of 12- and 15-year-olds reported attending for a check-up. According to parents, 9 in 10 children of all ages had visited a dentist in the last year and 9 in 10 parents reported they were satisfied with the last dental practice their child had visited. There was some variation by country with respect to children's experiences of fillings and extractions.
Conclusions There has been little change in the reported attendance patterns of children since the 2003 survey. Family deprivation (measured by children's eligibility for free school meals) negatively influenced dental attendance for regular check-ups, attendance within the last 12 months and the likelihood of having experienced difficulties accessing NHS dental services for children.
Similar content being viewed by others
Background
The 2013 Children's Dental Health (CDH) Survey, commissioned by the Health and Social Care Information Centre, is the fifth in a series of national children's dental health surveys that have been carried out every ten years since 1973.1 The 2013 CDH survey provides statistical estimates on the dental and oral health of children in England, Wales and Northern Ireland as well as providing information on children's related experiences, perceptions and behaviours. Children's parents or guardians (hereafter referred to as 'parents' for brevity) were asked to provide this information through self-completion questionnaires, and for the first time in the CDH survey series, older children aged 12 and 15 years of age were also asked to complete a questionnaire at the same time as the dental examination.
Since the 2003 CDH survey, there have been significant changes to the organisational structure of primary care NHS dental services particularly in the devolved countries of England and Wales. In April 2006, a new General Dental Services (nGDS) contract was introduced in England and Wales and funding for these services became overtly 'cash-limited'2 when the responsibility for resources was transferred to the former Primary Care Trusts (PCTs) in England and Local Health Boards (LHBs) in Wales alongside the introduction of local dental commissioning. Amongst many related developments at that time, a new contract currency the 'unit of dental activity' (UDA) was introduced in these countries which measured dentists' performance within a 12-month period for an agreed contract value. Following an independent review of NHS dental services in England,3 the Department of Health is currently piloting and testing prototypes for a 'reformed' contract built around a care pathway approach and incorporating key elements including disease prevention, treatment quality and continuing care.4
Regular dental attendance is important as it provides opportunities to prevent as well as treat dental disease. Children's dental attendance patterns also have implications for NHS resources and how NHS dental services are provided. Following the 2003 CDH survey, the National Institute for Health and Care Excellence (NICE) issued a guideline on dental checks: intervals between oral health reviews.5 The guideline is based upon the best available evidence and its purpose is to assist clinicians to select appropriate recall intervals between oral health reviews based upon their patient's needs. The guideline states that for children (below 18 years of age) the longest recall interval between reviews is 12 months and the shortest interval is three months.
In recent years, key documents such as Delivering Better Oral Health: an evidence-based toolkit for prevention6 have provided the dental team with a comprehensive and readily accessible source of information relating to advice and preventive interventions for patients at all levels of disease risk. One of the key philosophies adopted by this document is 'proportionate universalism' which aims at reducing health inequalities and the steepness of the social gradient in health by providing preventive actions to all, but with a scale and intensity that is proportionate to the level of disadvantage.7 Related to these challenges, commissioning better oral health for children is an area of current focus and interest.8
This paper aims to describe children's reported use of dental services, their experience of receiving dental treatment and parental satisfaction with different aspects of dental services across England, Wales and Northern Ireland.
Methodology
Full details of sampling, response, examination protocols and statistical methods can be found elsewhere.9 However, as a brief overview, the 2013 survey was based on a representative sample of children aged 5, 8, 12, and 15 years, attending government maintained and independent schools in England, Wales and Northern Ireland. The survey was conducted by a consortium led by the Office for National Statistics (ONS) and it involved 775 primary schools and 219 secondary schools.
Pupil questionnaire
An innovation for the 2013 survey was the introduction of a pupil questionnaire for 12- and 15-year-olds to complement the questionnaires sent to parents. The rationale for introducing the pupil questionnaire was to include the self-reported perceptions and behaviours of older children about their oral and general health in order to allow for the analysis of more accurate data than would have been possible via parents alone. Similarly, analysis of the data generated by both participant groups is important as it contributes towards a more complete picture of oral health in these age groups as well as our understanding of the demand for, and utilisation of dental care services.
Topics covered in the parent questionnaire included: child's ethnicity; child's dental anxiety; parent's educational qualifications; pattern of dental visits; and the occupation of the family reference person, although this list is not exhaustive. The pupil questionnaire was designed to be completed within ten minutes and it was presented at the same appointment as the clinical dental examination. The pupil questionnaire included topics such as: satisfaction with appearance of teeth; tooth brushing behaviour; smoking and drinking behaviour and self-rated dental and general health.
Data analysis
In view of the complexity of the sampling design and resultant weighting procedures, sampling errors were quantified using statistics programme STATA,10 and were calculated using a design factor (deft) to take account of the complex sampling and weighting procedures. The statistical significances in means and percentages between sub-groups were tested by calculating the confidence interval for the differences observed, based on the standard errors calculated using the design factor. This ensured that sampling error was taken into account in the testing procedure. Where significant differences are reported in the text, these are statistically significant at the 5% threshold (P <0.05) unless otherwise stated.
Ethical approval
The survey was ethically reviewed (University College London, Project ID: 2000/003) following changes made as a consequence of piloting and it received a favourable ethical opinion.
Results
A total of 13,628 children were sampled within participating schools and 9,866 children were examined, with a response rate of 72.4%.
Questionnaire response
The pupil questionnaire distributed to 12 and 15-year-olds achieved a response rate of 99.6%. The overall response rate for the parent questionnaire was 43%. Item non-response in both the parent and pupil questionnaires was generally below 2% for most question formats.
Dental attendance
Age of first visit
There was little evidence of much change in the proportion of children in England, Wales and Northern Ireland reportedly attending the dentist by two years of age in 2013 compared to 2003. In 2003, 29% of 5-year-olds and 32% of 8-year-olds had attended by the age of two. In the 2013 survey the figures were similar, with 30% of 5-year-olds and 34% of 8-year-olds having attended the dentist by the same age. In previous CDH surveys when the whole of the UK had been surveyed, the youngest age group (5-year-olds) had the highest proportion of non-attendance at a dentist compared to the other age groups. Across the whole of the UK, non-attendance of 5-years-olds was reportedly 14% in 1983, 10% in 1993, 6% in 2003 and in England, Wales and Northern Ireland in 2013, this figure remained at 6%. However, non-attendance in this youngest age group remains higher than the reported non-attendance in each of the older age groups (≤1%) in 2013.
Self-reported dental attendance
Just over 80% of all 12- and 15-year-olds reported attending for a check-up although this means that approximately one fifth of this age group did not. Children in England were less likely to report attending for a dental check-up than those in Wales and Northern Ireland and this difference was greater in 12-year-olds than 15-year-olds. In 2013, 3% of 12-year-olds and 2% of 15-year-olds reported that they had never been to a dentist. Furthermore, older children living in rural areas were more likely to report attending the dentist for a check-up than children living at a home address in an urban area.
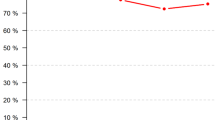
The 2013 CDH survey used children's eligibility for free school meals (FSMs) as a proxy for income deprivation for those living in low income families. It is important to note that only children living in low income families were eligible for FSMs at the time the survey was conducted. Within the 12- and 15-year-old age groups, income deprivation negatively influences dental attendance (Fig. 1). Two thirds of 12-year-olds receiving FSMs reported attending for a check-up compared to 86% of the same age group from less deprived families. Similarly, 27% of children eligible for FSMs reported going to the dentist only when they had trouble with their teeth, but the figure was just 12% in children from less deprived families. The self-report data for 12- and 15-year-olds show that between one quarter and one third of the more deprived adolescents do not benefit from a dental check-up.

Self-reported dental attendance of 12- and 15-year-olds by free school meal (FSM) eligibility
Parent-reported dental attendance
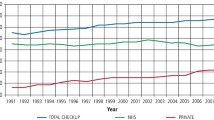
Since 2003 there has been little change in reported dental attendance patterns across England, Wales and Northern Ireland. Over nine in ten parents reported that their 12- and 15-year-old children attended the dentist for a check-up. However, the same question in the pupil questionnaire found just over eight out of ten children of the same ages reporting this directly.
In the 2013 survey, 95% of parents reported that their children's dental treatment was free. Only 5% of parents reported paying at the point of use or and/or using dental insurance. Differences between countries were negligible.
Across all age groups, a higher proportion of children not eligible for FSMs were reported to have visited the dentist in the last 12 months than those who were eligible.
A comparison was made of the parental reports and children's self-reports of dental attendance. Where children aged 12 and 15 years old reported that they attended for a check-up, 99% of parents independently agreed. However, where these older children reported that they only attended when having trouble (or had never been), over one third (37%) of parents still indicated that their child had attended for a check-up. Unsurprisingly, as parents' self-reported attendance at the dentist reduced, so did that of their children across all age groups (Table 1).11
Access to NHS dental services
There was little variation reported in the figures relating to access to NHS dental services by age of the child. Table 2 shows that over eight out of ten parents reported that they never had difficulty finding an NHS dentist and parents in Northern Ireland reported this more than parents in England and Wales.11 However, since the 2003 CDH survey there was a slight increase in the proportion of all parents reporting they had experienced difficulty finding an NHS dentist, rising from 9% in 2003 to 12% in 2013.
A higher proportion of parents of children eligible for FSMs reported that they had difficulty finding an NHS dentist compared to parents of children not eligible for FSMs. Over two thirds of parents who had experienced difficulty cited that this was because of local dentists not taking on NHS patients. A further 28% of all parents stated that the dentist had made it a condition that the parent (or parents) registered privately at the same practice.
Satisfaction with dental services
For the first time, the 2013 CDH survey asked parents how they would rate different aspects of the last dental practice they attended with their child. Overall satisfaction with dental services was high with over nine in ten parents reporting that they were satisfied with the last dental practice that their child visited (Table 3).11 In the 5-year-old age group, whilst 76% of parents in England were satisfied with the wait for an urgent appointment, satisfaction was higher in Wales (83%) and Northern Ireland (88%). In relation to 12-year-old children receiving FSMs, 68% of these parents were satisfied with the wait for an urgent appointment compared to 84% of parents of 12-year-old children not eligible for FSMs.
Dental care received
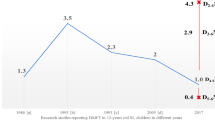
Unsurprisingly, children's lifetime experience of dental care increased with age although there were variations between countries (Table 4).11 By the age of 12 years, one quarter of children in England were reported to have had a permanent tooth filled, whilst in Wales and Northern Ireland the figures were 30% and 36%, respectively. By the age of 15 years, one in four children had experienced a filling or extraction of their primary teeth, 38% of children had received a filling in a permanent tooth and 21% had experienced an extraction of a permanent tooth.
The 2013 questionnaire asked parents if their child had ever had a general anaesthetic (GA) before dental treatment. In England, 9% of parents of 12-year-olds reported this compared to 21% of parents in Wales and 19% of parents in Northern Ireland. The reported use of sedation before dental treatment was broadly similar across ages and between countries.
There was a relationship between children experiencing some forms of dental care and income deprivation as measured by children's eligibility to receive FSMs. At ages 8 and 12, 14% and 22% of children eligible for FSMs were reported to have received a general anaesthetic before dental treatment. However, at the same ages for children not eligible for FSMs, their reported experience of general anaesthesia before dental treatment was 6% and 7%, respectively.
Discussion
There was little evidence of change since 2003 with respect to children's first reported attendance at the dentist or in the proportion of children reported to have attended the dentist in the last twelve months. Whilst the majority of older children reported that they attended the dentist for a check-up, one fifth of 12- and 15-year-olds did not report attending. Attendance for a dental check-up varied considerably by level of deprivation. Much higher proportions of older children not eligible for FSMs reported attending for a check-up than those who were eligible. The parents of children eligible for FSMs were also more likely to report having experienced difficulty finding an NHS dentist than those children not eligible. Overall, however, a high proportion of parents were satisfied with the last dental practice that their child had visited, and almost all of the children who had received dental care were reported by their parents to have done so through the NHS.
The 2013 CDH survey revealed interesting findings regarding parent-reported child dental attendance pattern and older children's self-reported dental attendance. Where dental attendance was favourable, the responses of children and their parents revealed a high level of agreement. However, there was less agreement where children reported they only attended when they had trouble or had never been to the dentist. The findings highlight that parents' and children's recall and reporting of dental attendance patterns may not always agree.
In general, there was little variation between boys and girls with regard to the dental care received. Children eligible for FSMs were more likely to have received a GA than those not eligible.
When interpreting data from the 2013 CDH survey, it is important to highlight changes in the consent methodology for participants. Prior to 2013, negative (opt-out) consent was used, but for 2013 the survey methodology changed to accommodate guidance which now requires positive (opt-in) parental/guardian consent.12 Whilst consent is not the only factor that may influence participation rates, the number of children examined in the CDH survey series has fallen since 1973. The impact and difficulties associated with introducing positive consent for dental epidemiological surveys are real and many of these issues have been previously highlighted.13,14
Fewer than half of parents completed the parental questionnaire in 2013, whereas the newly-introduced pupil questionnaire generated a near total response as this was completed on the day of the dental examination. Participant and parent non-response may lead to systematic changes (bias) in the data collected. Furthermore, if there is bias in the parental questionnaire data, the direction of this bias is likely to result in an overestimation of positive behaviours including participants' reported attendance at the dentist for a check-up. Both the parental and pupil questionnaires acted as self-report measures. Consequently, what children and adults say about their oral health behaviours and attitudes may not be an accurate reflection of what they actually do.
Conclusions
Whilst there have been changes to the geographic coverage, consent methodology and content of the 2013 CDH survey, there has been little change in the reported attendance patterns of children since 2003. The survey highlights apparent oral health inequalities in the survey population. Income deprivation (measured by children's eligibility for FSMs) was associated with a lower prevalence of attendance for a check-up at age five, a greater likelihood of a primary tooth having been filled at the same age and dental treatment under general anaesthesia at certain ages. There were country variations including a higher reported prevalence of general anaesthesia use for dental treatment at different ages in Wales and Northern Ireland compared to England.
Preventing dental disease is a priority, yet in the younger age groups only around half of parents reported their children had received advice on oral care (diet and tooth brushing) despite the fact that dental caries and many other oral conditions are almost entirely preventable.
These findings have a number of implications for dental services. There is a need for wider adoption of evidence-based clinical preventive guidelines as this paper has described. This action could be strengthened through the use of appropriately-trained dental care professionals under direct access arrangements and the leadership of dentists. The issue of reduced dental attendance with family income deprivation suggests there is a need for more focus upon encouraging relatively deprived families with very young children to attend for dental care. This could be progressed through the adoption of a more targeted population approach (proportionate universalism) which would require partnership working, community engagement and continued monitoring via the NHS dental epidemiological programme.
References
Todd J E . Children's dental health in England and Wales 1973. London: HMSO, 1975.
Freeman R . Reforming NHS dentistry. Br Med J 2008; 336: 1202–1203.
Department of Health. NHS dental services in England: An independent review led by Professor Jimmy Steele. London: Department of Health, 2009.
Department of Health. Dental Contract Reform: Prototypes. Overview document. London: Department of Health, 2015.
National Institute for Health and Care Excellence. Clinical Guideline 19. Dental checks: intervals between oral health reviews. 2004. Available online at https://www.nice.org.uk/guidance/cg19 (accessed July 2015).
Public Health England. Delivering Better Oral Health: an evidence-based toolkit for prevention. Third edition. 2014. Available online at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/367563/DBOHv32014OCTMainDocument_3.pdf (accessed August 2015).
Marmot M . Fair society, healthy lives: strategic review of health inequalities in England post-2010. Available online at http://www.instituteofhealthequity.org/projects/fair-society-healthy-lives-the-marmot-review (accessed August 2015).
Public Health England. Local authorities improving oral health: commissioning better oral health for children and young people. 2014. Available online at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/321503/CBOHMaindocumentJUNE2014.pdf (accessed August 2015).
Anderson T, Thomas C, Ryan R, Dennes M, Fuller E . Children's Dental Health Survey 2013. Technical Report- England, Wales and Northern Ireland. Health and Social Care Information Centre, 2015.
StataCorp. Stata Statistical Software: Release 11. 11 Ed. College Station, TX StatCorp LP, 2009.
Tsakos G, Hill K, Chadwick B, Anderson T . Children's Dental Health Survey 2013. Report 1: Attitudes, Behaviours and Children's Dental Health. England, Wales and Northern Ireland, 2013. London: Health and Social Care Information Centre, 2015.
Department of Health. Consent for school inspections and dental epidemiological surveys. Gateway Reference 6673. 2006. Available online at http://webarchive.nationalarchives.gov.uk/20070402085944/http://dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4135529 (accessed July 2015).
White D A, Morris A J, Hill K B, Bradnock G . Consent and school-based surveys. Br Dent J 2007; 202: 715–717.
Dyer T A, Marshman Z, Merrick D, Wyborn C, Godson J H . School-based epidemiological surveys and the impact of positive consent requirements. Br Dent J 2008; 205: 589–592.
Acknowledgements
The authors wish to thank the children and young people who took part in the research as well as their parents and guardians. In addition, the authors express gratitude to the dental examining teams, field workers from the Office for National Statistics, staff in the schools visited and the individuals involved in the consortium for their invaluable contributions. The 2013 CDHS was commissioned by the Health and Social Care Information Centre (HSCIC) and the research was carried out by a consortium led by the Office for National Statistics. We particularly extend our thanks to Tom Anderson of the ONS Social Survey Division and the wider ONS research team.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Holmes, R., Porter, J., Devapal, L. et al. Patterns of care and service use amongst children in England, Wales and Northern Ireland 2013. Br Dent J 221, 509–514 (2016). https://doi.org/10.1038/sj.bdj.2016.781
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2016.781
This article is cited by
-
Trends and inequalities in realised access to NHS primary care dental services in England before, during and throughout recovery from the COVID-19 pandemic
British Dental Journal (2023)
-
Providing sealants at the general anaesthetic assessment visit for children requiring caries-related dental extractions under general anaesthetic: a pilot randomised controlled trial
British Dental Journal (2021)
-
Outcomes and costs of pre-school and school-based fluoride varnish pilots
British Dental Journal (2017)
