
Key Points
-
Highlights that pre-operative anxiety related to dental implantology procedures is directly related to gender and age.
-
Suggests that well-administered IV sedation using midazolam in titrated doses produces an overwhelming positive response from patients with regard to the acceptance of further procedures being carried out under IV sedation.
Abstract
Objectives The aim of this three-year study was to evaluate whether elective comprehensive dental implant procedures involving guided bone and soft tissue regeneration carried out under intravenous sedation (midazolam) would be influenced by patient self-reported pre-operative anxiety levels; age and gender; effect the level of sedation with respect to the amount of sedative administered and the time taken in the procedures; effect patient intra-operative cooperation, and post-operative levels of patient satisfaction; influence further acceptance of dental implant surgical procedures; effect intra-operative surgeon satisfaction and consequently his/her post-operative sense of achievement.
Design Single centre general dental practice, open study as a clinical audit.
Method One hundred and seventy-three consecutive patients undergoing prolonged surgical procedures involving dental implantology with the adjunctive facility of intravenous sedation were monitored with respect to self-reported levels of anxiety. Vital signs of heart rate, mean systolic and diastolic blood pressure and arterial oxygen saturation were recorded and monitored pre-intra- and post-surgery. A post-operative questionnaire was completed as to the perceptions of the level of sedation.
Results A distinct relationship between self-reported pre-operative anxiety levels, age and gender were recorded - the younger the age, the higher the anxiety, with females dominating. Females required more midazolam than males. However, the analysis of the data as a whole, incorporating both genders, revealed a non-significant correlation result. The correlation between the midazolam dosage and the Corah anxiety score produced a p value result of: r (161) = 0.008, p <0.01. Forty-four percent of the patients described themselves as having 'high anxiety and fear of the dentist', however, 99.4% of the patients answered 'yes' to having sedation again in the future. For the purpose of this study, detailed consideration was given to the gender specific results in order to reveal a wider understanding of who poses as a 'cooperative patient'.
Conclusions The results should prompt a rethink as to who a cooperative patient is, and whether the self-assessed level of anxiety will influence further acceptance of dental implant surgical procedures under intravenous sedation.
Similar content being viewed by others

Introduction
The sensation of apprehension, stress, feeling of worry, nervousness or unease of events with uncertain outcome and fear of a threat of danger,1 combined with the activation of the autonomous nervous system is that emotional reaction commonly referred to as anxiety.2
It is widely recognised that dental procedures will elicit anxiety responses from patients. The degree of anxiety the patient experiences tends to be related to the scale of the proposed dental procedure.
When considering dental implants specifically, the overall procedure can prove difficult, not due to the possible advanced techniques that may be required of the surgeon, but because of the patient's tendency to acknowledge and respond to discomfort. Anxious patients can be very uncooperative during implant surgery and therefore, complicate the procedure. Where long dental implant procedures are anticipated, local anaesthesia may well be inadequate, and conscious intravenous (IV) sedation should become a viable and logical tool, so providing the patient with decreased perceptions or sensations of intra-operative pain and apprehension. The result should be the control of patient anxiety and the production of a cooperative patient.
The use of IV midazolam as a pre-medication for elective medical surgical procedures has often been investigated. Sun et al.3 investigated the use of IV midazolam as a pre-medication, demonstrating that age and gender have a clinically relevant effect on the dose of midazolam pre-medication that was administered. They found a higher level of pre-operative anxiety was more often apparent with females than men and that female or younger patients appeared to profit from the anxiolytic effects of midazolam. This significant decrease in anxiety levels for patients undergoing general surgery has also been reported by others.4 Research suggests that dental anxiety in the younger population is more severe when compared to the older patient.5 Where positive age effects are concerned, Jacobs et al.6 postulated that the increased pharmocological effect of midazolam in the elderly shows that ageing increases the pharmacodynamic sensitivity to midazolam.
The cooperation and eventual satisfaction with advanced dental procedures will vary, being dependant on the dosage of the administered sedative.7 Patients who are administered midazolam while engaging in dental procedures have been shown to have a lower heart rate and therefore, less anxiety symptoms at the intra-operative and post-operative stage. An optimal induction dosage of intravenous midazolam together with titrated additional doses will provide sufficient sedation and anxiolysis, so avoiding adverse effects but provide the surgeon with an optimised scenario for comprehensive implant surgery.
The aim of this 'open-ended' study was to investigate whether a patient's self-reported pre- and post-operative anxiety levels would:
-
Be influenced by age and gender
-
Have an effect on the level of sedation received with respect to the amount of sedative administered and the time taken in the operative procedures
-
Effect the level of patient intra-operative cooperation
-
Influence the post-operative levels of satisfaction experienced by the patient
-
Influence further acceptance of dental implant surgical procedures
-
Effect the level of intra-operative satisfaction experienced by the surgeon and his/hers post-operative sense of achievement
Materials and methods
One hundred and seventy-three consecutive patients presenting at a private practice dedicated to periodontics, dental implants and advanced restorative techniques were monitored in this continuous study. Where teeth were determined to be beyond further conservative therapy, the patients were offered the options of further treatment that included extraction and dental implant replacement therapy. All patients were provided with comprehensive and extensively written treatment plans that fully described the individual dental problems, the diagnosis of those problems and the proposed treatment and methodology. In this way they were able to give full informed consent. All treatment plans involved a comprehensive surgical treatment scenario that had varying combinations of:
-
The extraction and immediate placement of dental implants into vacated sockets
-
Dental implant placement into edentulous sites
-
Hard tissue grafting
-
Soft tissue grafting
-
Fitting of prosthetic devices.
-
All such surgery being projected as requiring a minimum of 60 minutes of active surgery.
The only exclusion criteria were: mental imbalance, known to be pre-existing (diagnosed), whether being treated or not; and patients suffering from recorded cardiovascular disorders whether under treatment or not. All patients had a review appointment to ensure ample opportunity was given to ask the surgeon any pending questions. Interim, preparatory appointments were arranged for the construction of prosthetic aids. Immediate to the anticipated surgery (usually seven to ten days) the patient's heart rate, systolic and diastolic blood pressure were recorded to ensure suitability for the projected intravenous sedation procedure.
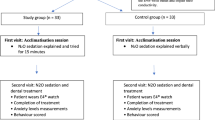
On the date of surgery, patients signed further informed consent for the administration of sedation and also completed a questionnaire to self-report on their pre-operative anxiety state on a five-point Likert scale, the Corah Dental Anxiety Scale, with answers ranging from 'not anxious' to 'extremely anxious' (Table 1).
The sedation was administered by an experienced dental sedationist (AMR), while all surgery was carried out by a single surgeon (SJM). The heart rate, systolic and diastolic blood pressure of each patient was measured immediately before the procedure to check, once again, their suitability for the sedation. Each patient was administered intravenous midazolam via a suitable vein in the method known as 'titration', whereby, after an initial titrated dos, at varying intervals (dependant on the patient's responses), additional titrants were injected. No fixed dosage of midazolam was used. The initial dosage and subsequent additions varied according to the patient's individual requirements. All sedation/surgery was carried out in a clinic appropriately equipped to provide advanced dental treatment and intravenous sedation. All operative sites were anaesthetised using 4% Articaine as both local and peri-ligamentary injections, and no inferior dental block injections were used.
It is to be noted that the pre-operative anxiety questionnaire and post-operative questionnaire are part of the normal clinical procedures in this practice.
Monitoring
Vital signs that included the heart rate (HR), mean systolic and diastolic blood pressure (MBP) together with arterial oxygen saturation (SpO2) were continuously monitored using a commercial device MEDEXCEL 3300ME. SpO2 was obtained by a sensor clipped to the finger tip of the patient. All readings were recorded throughout the sedation/surgical procedure. Any administrator-perceived complications, including apnoea, cardiac arrhythmias, hypotension were to be recorded.
The intra-operative and post-operative surgeon satisfaction was recorded immediately on departure of the patient following an appropriate observation period.
Patients attended a review appointment seven days after the treatment, at which time the individual patient's post-operative perceptions of overall experience, normality rating and memory rating was recorded. The patients' answers were recorded for statistical analysis, using both Pearson's correlation and the Student's t-test. All results where p <0.05 were considered as statistically significant.
Results
One hundred and seventy-three patients undergoing dental implant surgery under conscious intravenous sedation with varying combinations of the adjunctive 'techniques' of extractions, GBR and GTR were included in this study. A total of 395 dental implants were placed (average of 2.24). Three hundred and forty eight extractions before dental implant placement were carried out. Soft tissue grafting was performed in 119 of the cases and bone grafting, whether autogenous or allogenic, was carried out in 168 of the cases.
Only patients on the American Society of Anaesthesiologist's scale one or two were included in the study. All statistical tests were evaluated using SPSS statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA).
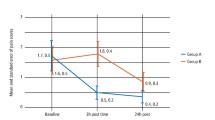
The pre-operative anxiety score was systematically evaluated (Fig. 1, Table 2), giving an average 10.95 out of a possible score of 25 on the five-point Likert Corah scale (SD ± 5.45). Gender specific results with regard to age and length of procedure are illustrated in Table 1.

Overall midazolam dosage and Corah anxiety correlation representation
The specific gender differences are shown in Table 3 and show a higher level of reported pre-operative anxiety present in female patients, the difference being measured as 2.67 on the pre-operative anxiety scale. Table 4 shows that there is a distinct relationship between self-reported pre-operative anxiety levels, age and gender: The younger the age, the higher the anxiety when compared to the 60+ age group. Of note, is to compare these results to the post-operative questionnaire results to the question 'reason for sedation' shown in Table 5, where patients could have multiple responses: 44% described themselves as having 'high anxiety and fear of the dentist'; 3% described themselves as having had a 'bad experience'; 1% a 'gag reflex'; 88% agreed to the intravenous sedation because of the 'length of the procedure and being advised'; 0.57% had 'other' reasons'.
The systolic and diastolic readings together with the individual heart-rate at the initial assessment and again on the date of surgery just before the procedure were measured and recorded for comparison (Table 6). The female patients had, on average, increased systolic and diastolic blood pressure and heart rate both at initial assessment and on the date of surgery when compared to the males. A Student's t-test was conducted to measure the difference in the results from initial assessment stage to date of operation. The results displayed a significant difference for the systolic reading with p = 0.007; no significant differences were present for the diastolic pressure and the heart rate.
The average dose of IV midazolam given to patients was 7.677 mg (SD ± 2.492). Male patients were administered, on average 7.52 mg of midazolam. Female patients averaged a total dose of 7.74 of midazolam. The total dosage difference between genders is shown in Table 2, representing an increase of 0.22 mg for the female patients. Of particular note here, females required more midazolam than males, regardless of the shorter operative times they were subjected to, which then relates to their increased level of reported anxiety.
A Pearson's correlation was conducted on the entire data set to establish the relationship between pre-operative anxiety and the total dosage of midazolam, the result verified the non-significant relationship: r (171) = 0.008, p <0.01 (Fig. 1). A Pearson's correlation was conducted on the male data set revealing another non-significant result: r (62) = 0.009, p <0.01. Similarly a Pearson's correlation conducted on the female data set produced a nonsignificant relationship: r (107) = 0.022, p <0.05.
The female patients demonstrated an increased memory rating despite being subject to an average increased dosage of midazolam (Table 7). The mode result for both male and female normality rating following their procedure was two on a five-point Likert scale. Ninety-seven percent of patients indicated 'just right' when questioned, post-procedure, on their perception regarding the level of sedation received (Appendix C).
To the question 'Did you receive adequate sedation information before the operation?', four patients answered 'no', resulting in 97% answering yes. When questioned following their implant surgery, 172 (99.4%) of the patients answered 'yes' to having sedation again in the future. Of note here, only one patient (female, aged 20 years) answered 'no'.
A five-point Likert scale was used to evaluate the surgeon's satisfaction with the intra-operative and post-operative sense of achievement: unacceptable, poor, satisfied, very satisfied and excellent. In the present study, the surgeon considered the intra-operative level of sedation, patient cooperation and ease of operation to be excellent in 91.33% of the cases under consideration; 7.52% to be very good; and 1.15% to be satisfactory.
To allow for the variation in the cohort numbers between the female and male cohorts, Levene's homogeneity test of equality of error variances was used. This tests whether the null hypothesis error variances of the dependent variable (gender) are equal across groups.
The variances of the total dosage of midazolam are the same across both male and female patients and the total midazolam dosage, producing a non-significant result (F (1,174) = 1.212, p >0.05 (0.272)).
The variances of Corah anxiety are not the same across both male and female patients and the total Corah anxiety score, producing a significant result (F (1,174) = 10.858, p <0.05 (0.001)).
Discussion
Anxiety in response to anticipated dental procedures has been well-recorded.5,8,9 Ellis found that where patients were undergoing third molar surgery with the aid of intravenous midazolam, 49% of the patients described themselves as having high anxiety and were less cooperative during the procedures. The mean value of Corah's scale recorded in our study was 10.95 (SD ± 5.45). Our results are much higher than those recorded in other studies: Brazil 9.8 (SD ± 3.7),10 Germany 8.6 (SD ± 3.7),11 and in Norway 7.9 (SD ± 3.5).12 This may well be explained by the pre-operative amount of descriptive information given to the patients in this present study to allow them to give full informed consent to the prospective procedures.
Gender influence remains one of the most frequently analysed variables in medicine; its relationship to dental anxiety has been well-recorded. This current study records that women have higher anxiety than men where dental implant surgery is concerned (Table 4). This is in agreement with González et al.10 and the Frazer and Hampson study,13 but disagrees with Hashem et al.2 Once again, the reason behind this could well be the extent of pre-operative information given to the patients to allow them to give full informed consent to the surgical procedure. Pre-operative anxiety was recorded in this study in multiple modes – via the Corah's Anxiety and Informative scoring and further in the post-operative questionnaire where 44% described themselves as having 'high anxiety and fear of the dentist'. However, this pre-operative reporting had very little effect on the level of surgeon satisfaction. The surgeon considered the intra-operative level of sedation, patient cooperation and ease of operation to be excellent in 91.33% of the cases under consideration. With those results in mind, 97% of patients indicated 'just right' when questioned, post-procedure, on their perception regarding the level of sedation received and 99.4% of the patients answered 'yes' to having sedation again in the future. These figures are in contrast to the study by González et al.10 who recorded 23.3% of patients having an agreeable experience, 28.9% as having neither a pleasant or unpleasant experience, while 36.7% reported their experience as slightly uncomfortable and 10% reporting the experience as disagreeable.
For surgeon satisfaction, the present results are much more positive than those recorded by González et al.:10 There, the level of surgeon satisfaction was 'adequate' at 87.8%. In two previous studies where third molar surgery was carried out under IV sedation, the surgeon's level of satisfaction with the procedures had been evaluated, showing vast variation - 85.8% satisfaction (evaluated on a visual analogue scale),14 and 55% excellent satisfaction (evaluated with unacceptable, poor, satisfactory, good and excellent). The more positive results obtained in this present study may well be attributed to the partnership between the surgeon and an experienced dental seditionist (AMR), administering the midazolam in individually titrated doses, as required by that patient. Other studies have anaesthetists using standard doses dependant on weight and standard time periods before the next dose.3,7,10,14
Anxiety is the result of a collection of individual psychological characteristics and the dose administered should be based on that individuals psychological needs. The results of this study promote the teaming together of an experienced dental sedationist with the surgeon when prolonged surgical procedures are being planned. This will allow the attainment of a high sense of patient well-being and high levels of surgical achievement during complex dental implantology procedures.
References
Kring A, Neale J M, Davison G C, Johnson S . Abnormal psychology. 12th ed. Toronto: Wiley, 2008.
Hashem A A, Claffey N M, O'Connell B . Pain and anxiety following the placement of dental implants. Int J Oral Maxillofac Implants 2006; 21: 943–950.
Sun G C, Hsu M C, Chia Y Y, Chen P Y, Shaw F Z . Effects of age and gender on intravenous midazolam premedication: a randomized double-blind study. Br J Anaesth 2008; 101: 632–639.
Fredman B, Lahay M, Zohar E, Golod M, Paruta I, Jedeikin R . The effect of midazolam premedication on mental and psychomotor recovery in geriatric patients undergoing brief surgical procedures. Anesth Analg 1999; 89: 1161–1166.
Liddell A, Locker D . Dental anxiety in the elderly. Psychol Health 1993; 8: 175–183.
Jacobs J R, Reves J G, Marty J, White W D, Bai S A, Smith L R . Ageing increases pharmacodynamics sensitivity to the hypnotic effects of midazolam. Anesth Analg 1995; 80: 143–148.
Garip H, Gürkan Y, Toker K, Göker K . A comparison of midazolam with remifentanil for patient-controlled sedation during operations on third molars. Br J Oral Maxilofac Surg 2007; 45: 212–216.
Eli I, Schwartz-Arad D, Baht R, Ben-Tuvim H . Effect of anxiety on the experience of pain in implant insertion. Clin Oral Implants Res 2003; 14: 115–118.
Ellis S . Response to intravenous midazolam sedation in general dental practice. Br Dent J 1996; 180: 417–420.
González-Lemonnier S, Bovaira-Forner M, Peņ˜arrocha-Diago M, Peņ˜arrocha-Oltra D . Relationship between preoperative anxiety and psot-operative satisfaction in dental surgery with intravenous conscious sedation. Med Oral Patol Oral Cir Bucal 2010; 15: e379–382.
Kunzelmann K H, Dünninger P . Dental fear and pain: effect on patient's perception of the dentist. Community Dent Oral Epidemiol 1990; 18: 264–266.
Neverlien PO . Normative data for Corah's Dental Anxiety Scale (DAS) for the Norwegian population. Community Dent Oral Epidemiol 1990; 18: 162.
Frazer M, Hampson S . Some personality factors related to dental anxiety and fear of pain. Br Dent J 1988; 165: 436–439.
Ganzberg S, Pape R A, Beck F M . Remifentanil for use during conscious sedation in outpatient surgery. J Oral Maxillofac Surg 2002; 60: 244–250.
Acknowledgements
To my dental sedationist colleague, Dr Ana-Marie Roman, MSc, MSc, MFDS, BDS, Dip Dental Sedation and registered Specialist in Oral Surgery. Sara Maher, School of Social Sciences, Southampton Solent University, UK, for collating all the statistical information.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
McCrea, S. Intravenous sedation as an adjunct to advanced comprehensive dental implantology: the patient's perspective and operator satisfaction. Br Dent J 218, E11 (2015). https://doi.org/10.1038/sj.bdj.2015.192
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2015.192
This article is cited by
-
Less stress, better success: a scoping review on the effects of anxiety on anesthetic and analgesic consumption
Journal of Anesthesia (2022)
-
Sedierung in der Zahn‑, Mund- und Kieferheilkunde
wissen kompakt (2021)
