
Key Points
-
Many members of staff did not know if their practice had a website or what the website address was.
-
Items of essential information were frequently absent.
-
Tooth whitening was promoted on 89% of websites despite legality issues.
-
Many websites advertised Botox injections despite the illegality of advertising prescription-only medications.
Abstract
Aims and objectives To investigate the quality and content of dental practice websites by constructing an audit framework based on regulations, guidance and expert advice, and applying this framework to a random sample of UK dental practices' websites.
Methods An audit framework was constructed and in-depth data collected from a random sample of 150 UK dental practices.
Results Thirty-five percent of dental practices in this study were found to have websites. Compliance with rules and regulations regarding dental practice websites was generally poor. Use of advised content for practice promotion was variable. Many websites were poorly optimised. Eighty-nine percent of the websites advertised tooth whitening, despite the issues surrounding its legality; 25% of the websites advertised Botox even though advertising of prescription only medicines is illegal. Some websites gave misleading information about the specialist status of their dentists.
Conclusions Those responsible for dental practice websites need to be aware of a wide range of regulations and guidance, and are advised to follow expert advice on content and optimisation in order to maximise the potential of their websites.
Similar content being viewed by others

Introduction
At a time where internet access is increasingly widespread, more and more dental practices are developing websites to attract new patients and provide information and marketing to existing ones. A recent study1 showed that nearly 70% of patients attending clinics at a dental hospital in Cork, Ireland, were using the internet on a daily basis and that 34.5% of patients (or friends/family) researched their present dental condition. Websites also help develop professional branding, which can increase competitive advantage and ensure a more predictable flow of patients.2 Estimates of the value of a website are variable. Dental-design.co.uk, a dental marketing firm, claims on its website that 'on average, clients receive between 5-10 patient contacts per month and in excess of 2,500 page views'. In order to maximise the potential use of a website it is essential to market the website and ensure it is well optimised.
Regulations and guidance that must be considered include the 'Code of Conduct for Dentists for Electronic Commerce in the EU',3 the General Dental Council guidance Standards for dental professionals,4 the Disability Rights Commission report The web: access and inclusion for disabled people,5 the Web Content Accessibility Guidelines (WCAG 1999),6 the Health On the Net Foundation Code of Conduct (HON code),7 and the Freedom of Information Act 2000.8 A study by Addy et al.9 used a survey of 101 websites from dental practices in major towns and cities in England to investigate the compliance with the Electronic Commerce Regulations (2002) and found that no practices were compliant with these regulations.
Several papers10,11,12,13 give advice on creating a practice website. The British Dental Association also offers advice14 and suggest a practice website is a 'vital marketing tool'.
Chestnutt et al.15 found that only 12% of a sample of UK dentists had a practice website, though a further 23% were considering having one. This study also looked at the general impact of the internet on dentistry and concluded that this was generally positive but that there was a long way to go before its full potential was realised.
The aim of this study was to investigate the quality and content of dental practice websites by constructing an audit framework based on regulations, guidance and expert advice, and applying this framework to a random sample of UK dental practices' websites.
Method
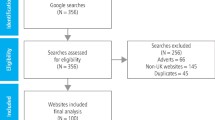
An audit framework was devised to identify first what proportion of UK dental practices had websites and then to collect in-depth information about the quality, content, usability, and optimisation of the websites. (This can be seen in completed form in the results section.) There were five subsections: presence of a website, compliance with rules and regulations, content for practice promotion, website optimisation, and additional comments. The aim was to use the most complete possible sampling frame of UK dental practices, as no comprehensive database exists. This is likely to be listings for 'dentist' in the Yellow Pages as it can reasonably be expected that virtually every dental practice in the UK would be listed here. Such a search on Yell.com gives a listing of 12,476 'dentists' where 'dentist' refers to dental practices. A pilot exercise estimated that approximately four in ten dental practices have websites. A sample size of 150 was chosen in order to yield a minimum of 50 websites for the in-depth audit.
Practices were chosen at random from the Yell.com listing. Unfortunately, although Yell.com lists over 12,000 dentists, only the first 100 items from any search can be displayed. Therefore 15 postcode areas were selected from an alphabetically ordered list of all UK postcodes areas (for example, LU, KT). These were selected at random using the random number generator on www.random.org. A Yell.com search was carried out for 'dentist' with each of these postcode areas in the area search box, and from each of these search listings, ten entries were chosen at random again using the random number generator.
Each of the 150 dental practices was telephoned. An inquiry was made as to whether or not the practice had a website. All the practice website addresses gathered were then visited in order to carry out the in-depth audit. All pages of the website were scrutinised and the audit framework completed. In cases where a specialist was referred to it was necessary to visit the General Dental Council website to verify if the dentist was indeed on the specialist register. Each practice was also checked on the NHS find-a-dentist service to verify whether the practice had an NHS contract.
Results
From the initial phone calls it was established that 53 of the 150 practices (35%) had websites. The results of the in-depth audit of these websites are shown in Table 1.
Discussion
On phoning the practices, many members of staff did not know whether the practice had a website or what the web address was. Some gave an email address unaware that this was not the same as a website address. In view of this it is possible that more than 53 (35%) of the 150 practices had websites, but that some members of staff were unaware of their existence.
Essential information such as dentists' names, qualifications, and GDC numbers was frequently absent. Only 19% of websites had a link to the GDC website and 4% displayed the GDC contact details. Just four websites (8%) made reference to the fact that the dentists adhere to the rules governing to profession.
The EC regulations3 specify that the time the website was last updated must be stated. This is important as it relates to the accuracy of the information. It may be that if a website has not been updated for many months important information may be incorrect such as the dentists working at the practice, or the treatment fees. Only four websites (8%) displayed the time since the site was last updated.
Guidance from the General Dental Council4 stipulates that only dentists who are on the specialist register may advertise as specialists. Of seven practices advertising specialists four were on the specialist list, and one advertised having specialists but these were not named. One site claimed a dentist who 'specialises in complex endodontics' and another that a dentist had a 'Specialist Diploma in Dental Implantology' but neither was on a specialist list. Such phrases would be considered by the GDC to contravene its guidance as it may mislead a patient into believing that the dentist was a qualified specialist. It is possible that contraventions are by dentists who have considerable expertise, which they feel they have a right to promote. Due to the practice-based nature of the profession, many dentists develop high levels of expertise in a particular field without following the structure required for a specialist list. Not only does this cause dissatisfaction among some dentists, but it does not give patients a satisfactory opportunity to judge the skill level of dentists practicing in specialist areas within practice.
A third stipulation is that practice advertising must not breach patient confidentiality. There is no breach of confidentiality if the patient has consented to their images being used on the website. It was not possible to establish this so this question in the study was flawed. There is also a grey area regarding which images require consent. A patient may understandably take issue with full face photos being used without consent but would be unlikely to recognise images of a single molar as their own. Use of testimonials also requires consent. A patient may be happy to provide a testimonial in which they discuss details of their treatment but may not want their name displayed with it. If the testimonial has arisen as part of a patient feedback process in the practice the patient could be unaware that the practice then intended to display it publicly.
The guidelines from the Disability Rights Commission5 cover complex areas of website coding which could not be investigated within the scope of this study. However, it is important to be aware of these guidelines and they should be considered when developing a website. Examples include having sufficient contrast between foreground and background, and having a text equivalent for every non-text element. Only 11% of the websites were found to comply with the Web Content Accessibility Guidelines (1999) (produced by the World Wide Web Consortium) to a recommended level of AA (on a scale of A, AA, or AAA where AAA is the highest rating).
Sacchetti et al.16 found that 'although the medical information available on the Web has proliferated at a remarkable rate, the number of websites providing complete, non-biased information continues to represent only a small portion of the total'. The Health on the Net Foundation Code of Conduct (HON code)7 provides guidance for basic ethical standards in the presentation of information to standardise the reliability and credibility of health information on the internet. Any claims made by a particular dentist must be supported by evidence, and evidence presented to patients should be balanced. Only two websites (4%) made claims that were considered relevant to these guidelines. One claimed 'gum disease is linked as a causative factor in heart disease and strokes'. Another claimed they could help 'reduce your risk of gum disease and other problems that have been associated with low birth weight babies'. Neither had a source cited, or any further explanation.
Information about fees was given on 49% of the websites investigated. Patients may feel reassured by a set fee list and gain confidence by the transparency of the fee structure. On the other hand patients may be put off by what they consider a high fee if they do not appreciate what is involved. By encouraging patients to phone the practice, or attend to discuss costs, the practice is given more opportunity to explain the fees, and also give advice on staging treatment, or use of payment plans. Fees, where quoted, are usually quoted as a 'from' price. This allows the practice to charge more depending on the complexity of a case. However, this can also diminish the transparency of the fees and leave patients none the wiser as to what the true cost of their treatment may be. The decision whether or not to display fees on the website will be a tactical decision for each individual practice based on what they feel will most suit their practice style and potential patients.
Details of the services offered were noted in the study. Although 87% of the websites offered cosmetic dentistry, 23% used terms such as 'smile design', 'smile makeover', 'smile enhancement', or 'smile lift' to promote further the special cosmetic skills of their dentists.
Tooth whitening was widely promoted, featuring on 89% of the websites. As of January 2011 it is illegal in the UK to supply a product for the purpose of tooth whitening if that product contains or releases more than 0.1% hydrogen peroxide. However, this law is largely ignored by dentists who feel that tooth whitening is a safe treatment, frequently in the best interests of their patients when an alternative may be a much more invasive procedure. The GDC supports dentists in their practice of tooth whitening procedures. However the 'position statement' of Dental Protection17 (a leading UK dental indemnity insurer) advises to 'avoid advertising the use of tooth whitening products as this may constitute intent to supply beyond an individual therapeutic decision' and that 'it is also likely to attract unfavourable attention from the local Trading Standards Officers'. It is likely that a risk-benefit analysis is being carried out by dentists. The risk of prosecution is small, and the benefits in terms of patient care and practice profitability are large. The legal situation is the subject of ongoing debate and it is hoped that the current unsatisfactory situation will eventually be resolved.
Under the Medicines (Advertising) Regulations 1994 it is illegal to advertise any prescription medication, including Botox, to the public. This study shows that a quarter of practice websites are openly advertising such treatment. The Medicine and Healthcare Regulatory Agency advise the service may be promoted as 'treatment for lines and wrinkles' but must not mention Botox. One website advertised 'muscle freezing injections' which the Medicine and Healthcare Regulatory Agency argue implies the use of Botox and should not be used. Others advertised 'anti-wrinkle injections' and 'muscle relaxing injections'. Many practitioners are knowingly or unknowingly breaking the law by advertising the treatment. Again it may be that practitioners have decided the risk of prosecution is small and the potential gain in terms of revenue for their business outweighs this. However, prosecutions do occur. The first such case was in 2005 and was brought by the Department of Health.18 In this case the offender was eventually fined £75 plus court costs after repeated warnings to remove the advertisement.
Another service promoted on some websites was a treatment coordinator (6%). This idea is relatively new to UK dentistry although this study shows that some practices have adopted the service. An excellent discussion of the role and benefits of a treatment coordinator can be found on the Advanced Dental Education Institute website.19
Creating a dental practice website can represent a considerable investment. To ensure this is worthwhile it is important that this website is well optimised. However, only 66% of the websites were listed in the first 20 results of a UK Google search where 'dental practice' and the relevant area or town was entered into the search box. Only 28% of the websites investigated were listed in Yell.com. There are different techniques for website optimisation which can be complex. Specialist services can be purchased to enhance website optimisation and these may be a worthwhile investment.
Conclusion
This study demonstrates that very few of the dental practice websites in this study fully conform to all the necessary regulations and very few incorporate all the expert advice on website content. Many are poorly optimised. Although there is a limitation in the small sample size of this study, it still acts to highlight areas where practices may be falling foul of legislation and guidelines and is important for all practitioners who have or are planning to have practice websites. Further research on a larger scale may further reinforce these findings. It is hoped that this study will help practitioners to understand what content is both required and advisable for their websites, for the current time at least.
References
Ní Riordain R, McCreary C . Dental patients' use of the internet. Br Dent J 2009; 207: 583–586.
Neely M H. Branding your practice: twelve practical steps to creating lifelong patient relationships. J Med Pract Manage 2005; 20: 266–270.
HM Government. The Electronic Commerce (EC Directive regulations) 2002. London: The Stationery Office, 2002. http://www.opsi.gov.uk/si/si2002/20022013.htm.
General Dental Council. Standards for dental professionals. London: General Dental Council, 2005.
Disability Rights Commission. The web: access and inclusion for disabled people. London: The Stationery Office, 2004.
W3C. Web Content Accessibility Guidelines 1.0. http://www.w3.org/TR/WCAG10/.
Health On the Net Foundation. The HON code of conduct for medical and health websites (HONcode). http://www.hon.ch/HONcode/Conduct.html.
National Health Service. NHS Freedom of Information website. http://www.foi.nhs.uk. Accessed 5 May 2009.
Addy L D, Uberoi J, Dubal R K, McAndrew R . Does your practice website need updating? Br Dent J 2005; 198: 259–260.
Downes P K. Creating a practice website. Br Dent J 2007: 202: 597–604.
Miller S A, Forrest J L . Dental practice websites: creating a web presence. Dent Clin North Am 2002; 46: 463–475.
Brandt C. Web marketing for oral and maxillofacial surgeons. Oral Maxillofac Surg Clin North Am 2008; 20: 91–100.
Coates J. Don't get left behind. BDA News 2009; April: 12–13.
British Dental Association. Advice leaflet A6: Promoting your practice. London: British Dental Association, 2007.
Chestnutt I G, Reynolds K . Perceptions of how the internet has impacted on dentistry. Br Dent J 2006; 200: 161–165.
Sacchetti P, Zvara P, Plante M K . The internet and patient education – resources and their reliability; focus on a select urologic topic. Urology 1999; 53: 1117–1120.
Dental Protection. Position statement on tooth whitening. http://www.dentalprotection.org/uk/positionstatements/toothwhitening.
Department of Health, Social Services and Public Safety for Northern Ireland. Beauty clinic owner fined for Botox advertisement. http://archive.nics.gov.uk/hss/051101l-hss.htm.
Jupp A. What is a treatment coordinator? http://www.learndental.com/articles/article_treatment_coord.html.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nichols, L., Hassall, D. Quality and content of dental practice websites. Br Dent J 210, E11 (2011). https://doi.org/10.1038/sj.bdj.2011.242
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2011.242
This article is cited by
-
Evaluation of the information provided by UK dental practice websites regarding complications of dental implants
British Dental Journal (2021)
-
Advertising and facial aesthetics in primary care: how compliant are practice websites and social media with published guidance?
British Dental Journal (2021)
-
The informative value and design of orthodontic practice websites in The Netherlands
Progress in Orthodontics (2020)
-
Compliance of NHS dental practice websites in Wales before and after the introduction of the GDC document 'Principles of ethical advertising'
British Dental Journal (2016)
-
The quality of orthodontic practice websites
British Dental Journal (2014)
