
Abstract
Study design:
Cross-sectional, observational.
Objectives:
To investigate the association of conflicts between work and family life with indicators of health and to examine the antecedents of those conflicts in employees with spinal cord injury (SCI) and their caregiving partners.
Setting:
Community, Switzerland.
Methods:
Data from employed persons with SCI (n=79) and caregiving partners (n=93) who participated in the pro-WELL study were used. Logistic and tobit regressions were performed to assess the association of work–family and family–work conflicts with health indicators, namely mental health (36-item Short Form Health Survey (SF-36)), vitality (SF-36), well-being (WHOQoL BREF) and positive and negative affect (Positive and Negative Affect Scale short form (PANAS-S)). Own and partners’ engagement in productive activities and socioeconomic circumstances were evaluated as potential antecedents of work–family and family–work conflicts using logistic regression.
Results:
Work–family conflicts were related to reduced mental health (caregiving partners only), vitality and well-being. Family–work conflicts were linked to reduced mental health, vitality, well-being and positive affect in SCI and to reduced vitality in caregiving partners. Persons with lower income (SCI only) and lower subjective social position reported more conflicts than persons with higher income and higher subjective position. Higher workload increased work–family conflicts in caregiving partners and decreased family–work conflicts in SCI. Education, amount of caregiving, care-receiving and partners’ employment status were not associated with the occurrence of conflicts.
Conclusion:
The optimal balance between work and family life is important to promote mental health, vitality and well-being in employees with SCI and their caregiving partners. This is especially true in employees perceiving their social position as low and in caregivers with a high workload.
Similar content being viewed by others

Introduction
Employees with spinal cord injury (SCI) and their caregiving partners are particularly vulnerable to conflicts between work and family life, given the cumulative burden of engagement in paid work and coping with the disabling condition. Work and family conflicts may arise as individuals are involved in different social roles (e.g., being an employee, a partner, a caregiver) that are linked to different role expectations.1 An involvement in a diversity of social roles may produce recurrent inter-role conflicts contributing to chronically stressful experiences for the individual.2 Evidence from general population studies confirms that work and family conflicts have serious consequences on an individual’s work and home life, general health and well-being.3, 4, 5, 6 For example, a meta-analytic review reported that employees suffering from work and family conflicts are at an increased risk for depression, anxiety, negative feelings, physical health problems and reduced well-being.6 To date, the potential impact of these conflicts has not been investigated in employees with SCI and their caregiving partners.
While it is certainly of interest to know whether inter-role conflicts are linked to health, it is of similar importance to explore potential antecedents of work and family conflicts in employees with SCI and their partners with caregiving obligations. We investigate two specific aspects that may have a role in the occurrence of conflicts, namely the amount of engagement in productive activities (e.g., paid work, caregiving) and socioeconomic circumstances (e.g., level of income, education).7 Conflicts between work and family life presumably result from an interplay between one’s own and one’s partners’ involvement in productive activities.8, 9 For instance, the engagement of both members of a couple in paid work may exacerbate inter-role conflicts as both have less time resources for family life. Furthermore, the occurrence of inter-role conflicts likely varies according to people’s socioeconomic circumstances. Although the assumption of a higher occurrence of conflicts in groups with adverse socioeconomic circumstances seems plausible, evidence is inconclusive.4, 7, 10, 11 Part of this inconsistency may be due to the use of inadequate indicators measuring socioeconomic circumstances in previous research. So far, education,4, 10 income7, 10 or occupational status11 were assessed, whereas complementary measures, such as subjective social position,12 have not been included. Subjective social position captures the individuals’ perception of its place in a hierarchically structured society.12 Again, the prevalence and impact of inter-role conflicts with regard to socioeconomic circumstances was mainly explored in general populations4, 7, 10, 11, 13 and not so in persons with disabilities or caregivers.
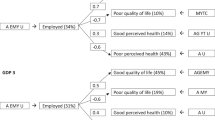
This is the first study that investigates the link between inter-role conflicts and health and explores potential antecedents of inter-role conflicts in employees with SCI and their caregiving partners. As inter-role conflicts are a potential source of stress,2 it is conceptually meaningful to study their association with stress-related health indicators such as mental health and well-being. We hereby differentiate between two forms of inter-role conflicts, namely conflicts that arise because work obligations impact on family life (work–family conflict) and conflicts that arise because family obligations impact on work life (family–work conflict). In summary, the primary aim of this study is to investigate the association of work–family and family–work conflicts with self-reported health indicators, namely mental health, vitality, well-being and positive and negative affect. The secondary aim of this study is to examine potential antecedents of inter-role conflicts by studying the association of own and partners’ engagement in paid work and caregiving and three distinct indicators of socioeconomic circumstances with work–family and family–work conflicts (Figure 1).

Study aims.
Materials and methods
Sampling frame and participants
We used data from the pro-WELL study,14 a nested study within the community survey of the Swiss Spinal Cord Injury Cohort Study (SwiSCI).15, 16 The sampling frame of pro-WELL included a representative population of 1922 Swiss residents aged over 16 years with a diagnosis of traumatic or nontraumatic SCI.15, 16 The pro-WELL study only involved couples. Therefore, persons with SCI were only eligible if they lived in a stable relationship (irrelevant whether married or not) and could only be included if their partner agreed to participate as well. Whether a person was in a stable partnership or not was assessed based on self-report of the person with SCI during the recruitment procedure. Of the 1922 SwiSCI participants, 676 persons were eligible for pro-WELL and 133 persons with SCI and their caregiving partners participated in the baseline assessment (response rate 19.7%). Details on inclusion criteria, recruitment outcomes, participation rates and nonresponse are reported in the pro-WELL cohort profile.14
Study design
Pro-WELL is a longitudinal study with three measurement waves (baseline; month 6; month 12) that aims to investigate associations of availability and quality of close social relationships and productive activities with well-being in persons with SCI and their caregiving partners.14 Data were collected using standardised telephone interviews and paper–pencil or online questionnaires. Here, we use cross-sectional data from employed persons who participated in the baseline assessment carried out between May 2015 and January 2016. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. The study protocol and all measurements were approved by the Ethical Committee of Northwest and Central Switzerland (document EKNZ 2014-285).
Measurements
Work–family and family–work conflicts
Work–family and family–work conflicts are related but distinct constructs that should be analysed separately, as different causes and effects on health have been observed.6, 7 These inter-role conflicts were assessed with two strain-based items from the Work–Family Conflict Scale.17 We used items assessing strain-based inter-role conflicts, which commonly display stronger associations with well-being than time- or behaviour-based conflicts.17 Work–family conflicts are assessed with the item ‘when I get home from work I am often too frazzled to participate in family activities’ and family–work conflicts were assessed with the item ‘Tension and anxiety from my family life often weakens my ability to do my job’. Both items were rated on a four-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’.
Health indicators
To measure health, we used the five-item mental health and four-item vitality subscales from the 36-item Short Form Health Survey (SF-36, version 1.0),18 a five-item selection of WHOQoL BREF19 and the Positive and Negative Affect Scale short form (PANAS-S).20 The SF-36 mental health and vitality subscales evaluated the frequency of specific mental and vital states on a six-point scale ranging from ‘all of the time’ to ‘none of the time’.18 A sumscore ranging from 0 to 100 was computed according to the established scoring algorithms for both subscales,21 with higher scores indicating better mental health and vitality. In line with conventional definitions,22 subjective well-being was conceptualised as containing a cognitive and an affective component. The cognitive component was assessed on a five-point scale with five selected items of the WHOQoL BREF, specifically validated for SCI.23 These items cover people’s perception of the overall quality of life and domain-specific life satisfaction, that is, satisfaction with health, social relationships, activities of daily living and living conditions. A sumscore ranging from 0 to 20 was calculated, with higher scores indicating higher well-being. The affective component of well-being was measured by the PANAS-S,24 including two subscales (five items positive, five items negative affect), assessing the strength of emotions on a five-point scale.20
Socioeconomic circumstances
Years of education, net-equivalent household income and subjective social position were used as individual-level indicators of socioeconomic circumstances. Education was assessed according to the International Standard Classification of Education as total years of formal education, including school and vocational training.25 Net-equivalent household income in Swiss Francs was calculated by including information on disposable household income, weighted by number of adults and children living in a household according to OECD criteria.26 The continuous income variable was divided by 1000 to receive legible effect sizes. The MacArthur Scale of subjective social status12 was used to capture the subjective evaluation of one’s position in society, represented by a 10-rung ladder. Participants were instructed to imagine those with the highest social status at the top and those with the lowest status at the bottom, and they were then asked to cross the rung on which they would place themselves.
Engagement in productive activities
Engagement in productive activities was defined as hours of paid work and amount of daily caregiving, which was assessed only for caregiving partners.
Potential confounders
Age, gender and lesion severity (classified as incomplete paraplegia; complete paraplegia; incomplete tetraplegia and complete tetraplegia) were introduced as confounding variables in multivariable models. Data on lesion severity were collected in the SwiSCI community survey 2012 and have not been repeatedly assessed for the pro-WELL study. Self-report data from the SwiSCI survey 2012 have shown good reliability when compared to data from medical records of participants (κ 0.89).16
Statistical analyses
Analyses were conducted using STATA version 14.0 for Windows (College Station, TX, USA). For all variables, the crude distribution is described and compared between persons with SCI and caregiving partners using χ2 statistics for dichotomous and Mann–Whitney U-tests for ordinal variables. To evaluate within-dyad dependency of inter-role conflicts in couples where both members were employed (n=60 couples), Pearson's correlation was used.27
Regression models were performed separately for persons with SCI (n=79) and caregivers (n=93). We applied a dyadic perspective, including information from both members of a couple in regression analysis. To each individual, data from his or her partner were added as predictor variables. More specifically, data on lesion severity, employment status (paid work yes/no) and care-receiving of the person with SCI were added to the data of the caregiving partner; hours of caregiving and employment status of the caregiving partner was added to the data of the person with SCI.
To explore the relationship of work–family and family–work conflicts with health indicators, tobit and logistic regressions were applied. To account for censoring effects in continuous outcomes (mental health, vitality, well-being and positive affect), tobit models were used.28 To account for the negative binominal distribution in the negative affect, logistic regression was applied. The negative affect subscale ranging from 5 to 25 was dichotomised using the upper quintile as a cutoff (<10: lower negative affect; ⩾11: upper quintile of a negative affect). Three subsequent models were computed: Model 1 was unadjusted; Model 2 was adjusted for age, gender, lesion severity, net-equivalent household income and subjective social position and Model 3 was adjusted for all covariates of Model 2 and partners’ engagement in productive activities (hours of caregiving, paid work yes/no).
To investigate own and partners’ engagement in productive activities and socioeconomic circumstances as potential antecedents of work–family and family–work conflicts, logistic regressions were applied. The conflict items were used as separate binary outcomes. Owing to low sample size and therefore small numbers of individuals within each category, ordinal responses of the conflict items were dichotomised into ‘some conflict’ (responses ‘agree’ and ‘strongly agree’) and ‘no conflict’ (responses ‘disagree’ and ‘strongly disagree’). Hours of paid work, education, income and subjective social position were introduced as continuous variables and information on daily hours of caregiving and partners’ employment status was used as dichotomous variables (caregiving less than an hour vs an hour or more; partner in paid work vs partner not in paid work). Following an unadjusted model, we adjusted the estimates for age, gender and lesion severity.
In the respective tables, β-coefficients (for tobit regressions) and odds ratios (for logistic regressions), 95% confidence intervals and P-values from the equal fraction missing information test are presented.29 The equal fraction missing information test is a likelihood ratio test suitable for multiplying imputed data sets.
Item nonresponse was addressed using multiple imputation. Multiple imputation by chained equations were applied to impute different types of variables, including categorical, ordinal and linear variables.30 All missing values of covariates except those in health indicators were imputed. For each model, imputations were carried out for 10 data sets.
Results
The basic characteristics of the employed pro-WELL baseline sample are displayed in Table 1. The majority of persons with SCI were male and the majority of caregiving partners were female. The mean age was 48 years in both groups. Over 75% of participants with SCI had a paraplegia, mostly of traumatic aetiology. The mean duration of education was about 14 years in both groups, and persons with SCI had a tentatively higher household income than caregivers. The subjective social position was around 6 out of 10 for both groups, indicating that persons perceive themselves as being about average in terms of social status. Persons with SCI indicated working about 4.7 h less per week than caregiving partners. About 60% of caregivers reported at least 1 h of caregiving per day. In three-quarters of employees with SCI and in two-third of caregivers, the partner was also engaged in paid work. More than half of the employees with SCI received at least 1 h of care per day. Work–family conflicts were more prevalent in caregivers, while family–work conflicts were slightly more common in SCI. Caregivers indicated on average better health in all indicators than persons with SCI; however, differences were nonsignificant except for well-being (P=0.02).
Correlations of inter-role conflicts within couples were low (work–family conflicts: r=−0.14; family–work conflicts: r=−0.16), indicating that there was no consistent association in the reporting of inter-role conflicts within couples.
Primary study aim: inter-role conflicts and health
Figure 2 depicts the adjusted effect sizes from multivariable models on the association of inter-role conflicts and health indicators. The details on these models are provided as Supplementary Information. Work–family conflicts were consistently associated with reduced mental health, vitality and well-being in caregivers, and with reduced vitality and well-being in persons with SCI. These associations remained stable after adjustment for potential confounders, such as gender, age, lesion severity, socioeconomic circumstances, hours of caregiving and partner’s employment status. Family–work conflicts were related to reduced mental health, vitality, well-being and positive affect in SCI in adjusted models. In caregivers, family–work conflicts were associated with reduced vitality in the final models. Work–family and family–work conflicts were tentatively associated to a lower positive affect and a higher negative affect (P>0.05).

Adjusted effect sizes (with 95% confidence intervals) for the associations of inter-role conflicts with health outcomes. Open circles indicate persons with SCI and closed circles indicate caregiving partners. The dashed line depicts the relative effect in the reference group with no conflict (i.e., 0 for continuous outcomes, 1 for a binary outcome). The grey areas in the top graphs for mental health and vitality indicate the accepted minimum clinically relevant differences of 5 points.
Secondary study aim: antecedents of inter-role conflicts
Hours of paid work were positively related to the occurrence of work–family conflicts in caregiving partners and negatively related to the occurrence of family–work conflicts in SCI. We observed trends towards reduced occurrence of work–family conflicts but increased family–work conflicts in caregivers with high involvement in caregiving. Persons with SCI who received at least 1 h of care showed slightly more inter-role conflicts. We detected a trend of reduced occurrence of family–work conflicts if the partner was also engaged in paid work, however, we observed no association between partners’ employment status and work–family conflicts.
Household income and subjective social position showed consistent negative associations with inter-role conflicts in persons with SCI, indicating that persons with lower income and lower subjective social position had a higher likelihood of experiencing work–family conflicts and family–work conflicts. In caregivers, lower subjective social position was related to the occurrence of family–work conflicts. Years of education were not related to either form of conflict (Table 2).
Discussion
Our study provides robust evidence on the associations between inter-role conflicts and health, as employees who encounter conflicts between work and family life reported poorer mental health, lower vitality and lower well-being than employees with well-balanced work and family obligations. Furthermore, we observed that income and subjective social position play an important role in the occurrence of inter-role conflicts. However, education, the amount of caregiving, care-receiving and partners’ employment status were not associated with the occurrence of conflicts.
Inter-role conflicts and health
The observed association of inter-role conflicts with health and well-being is in line with previous findings documented in a systematic review.6 Of the 14 included studies on general psychological strain, 13 studies reported significant associations between work–family conflicts and psychological strain, with a weighted mean correlation of 0.29 over studies. A consistent relationship between work–family conflicts and depression was observed in all included studies (k=11; weighted mean correlation 0.32) and a negative correlation of work–family conflicts and life satisfaction was reported in 16 out of 18 studies (weighted mean correlation −0.28).6 Findings on the association of family–work conflicts and health are less numerous; however, available evidence supports the associations observed for work–family conflicts and health.8, 31 For example, family–work conflicts were related to reduced mental health in a large sample of employees from the United Kingdom, Finland and Japan.31 Potential explanations for the observed health effects of inter-role conflicts are again based on findings from general populations, while research on persons with disabilities is currently unavailable. General population data suggests that the burden of inter-role conflicts may be related to adverse health behaviours, such as little physical activity,5 poor nutrition32 or enhanced alcohol intake6 that may chronically affect health. Further, persons who experience recurrent inter-role conflicts may encounter poor social support,33 and the chronic stress experiences due to inter-role conflicts may lead to negative emotions and subsequent psychobiological stress reactions that negatively impact on health.34 Summarising, our study suggests that inter-role conflicts may not be strongly moderated by the burden of caregiving or the disabling condition, as our findings are largely in line with findings from general populations. However, additional studies in the context of disability are warranted.
The stronger link between family–work conflicts and health outcomes in persons with SCI as compared to caregiving partners may be explained by the additional investments in time and energy to accomplish everyday routines in persons with SCI. These inevitable investments may have rendered persons with SCI more vulnerable to the negative impact of homegrown tensions on mental health, vitality and well-being. Interestingly, this heightened negative impact of family–work conflicts in SCI existed despite being frequently engaged in part-time positions.35 This finding indicates that employees with SCI may profit from interventions that strengthen their ability to cope with the remaining challenges of balancing family and work life in the face of the disabling condition rather than a further reduction in workload. Furthermore, we found that mental health, vitality and well-being were more strongly linked to inter-role conflicts than positive and negative affects. While the measures of mental health, vitality and well-being reflect integral assessments over a period of time (e.g., they last for 2 weeks), positive and negative affects assess momentary mood states subject to short-term variations.
Antecedents of inter-role conflicts
The role of own and partners’ engagement in productive activities in the occurrence of inter-role conflicts was inconclusive. Hours of paid work was the only variable that seemed to relate to inter-role conflicts; however, patterns of relationships were inconsistent across the type of conflict and group of persons, leading to the suspicion that other non-measured variables such as bodily capacity or coping skills may have confounded the observed association.
In contrast, we found evidence for social inequality in the occurrence of inter-role conflicts. We found that self-evaluated social position, a more proximal indicator of socioeconomic circumstances, was a better predictor of inter-role conflicts than traditional indicators, such as income or education. Similar observations were reported in an earlier study of persons with SCI,36 where self-reported financial hardship was more closely associated with health than conventional, more distant socioeconomic indicators. Proximal indicators of social disadvantage may reflect the disparities of social resources that are needed to cope with the stressful conflicts of everyday life more accurately.37
Strength and limitations
This study is the first to analyse inter-role conflicts among employees with SCI and caregiving partners, by focussing on two directions of conflicts, work–family and family–work conflicts. We used a comprehensive set of self-reported health indicators, measured by validated instruments. Furthermore, we took partners’ engagement in productive activities into account, thus providing a dyadic perspective on the occurrence of inter-role conflicts. In addition to the conventional measures education and income, we introduced subjective social position as a rarely studied indicator of socioeconomic circumstances into analysis.
The cross-sectional design provides a major limitation of this study, as reverse causation cannot be excluded and persons with poorer health might be more susceptible to experience inter-role conflicts. Another study limitation is the use of single items to measure work–family and family–work conflicts. As argued in a systematic review, the tradition of measuring these constructs with few items is a general methodological problem and calls for more comprehensive assessments in future studies.6 Further, our sample is relatively small and a lack of statistical significance might be the result of a small sample size.38, 39 For example, we found relatively large odds ratios for work–family and family–work conflicts and a negative affect (see Figure 2), but we also found large confidence intervals and, as a consequence, P-values above 0.05. The low response rate also rendered the pro-WELL study at a risk of sampling bias, although the sample that represented the larger population was included in the SwiSCI study quite well in terms of sociodemographic and lesion characteristics.14
Implications
In light of our findings on the link of inter-role conflicts with mental health and well-being, it is important to support employees in their ability to balance work and family life, especially if employees face the double burden of coping with the disabling condition and employment. In addition, persons with low subjective social positions or low income deserve special attention, given their high prevalence of inter-role conflicts. However, our findings provide limited evidence on additional targets for intervention, as findings on other potential antecedents of inter-role conflicts were inconclusive. Future studies may investigate the role of psychological resources (e.g., coping skills, self-efficacy), social relationships (e.g., social support, partner-relationship quality and family functioning) or bodily capacity (e.g., independence in activities of daily living) as individual-level antecedents of inter-role conflicts.
At the organisational level, a number of conflict-reducing interventions have been implemented and evaluated in general40, 41, 42 and in caregiving populations.43 The findings showed that organisational and supervisor support,40 more flexible work arrangements, increased control over work time41 and strengthening peoples’ resources towards better coping with competing obligations from work and family present promising measures to reduce work–family conflicts.42 Although evidence on specific needs of employees with disabilities and caregivers is limited, we presume that specific interventions that involve the management of disability-related health issues or caregiving tasks need to be included in interventions to account for the specific challenges of this potentially vulnerable group of employees.
Conclusion
This study provides evidence that conflicts between work and family obligations are linked to health in employees with SCI and caregiving partners. Labour market policies, supervisor interventions and strengthening the individuals strategies to cope with multiple obligations and disability-related health issues should therefore be of high priority to minimise inter-role conflicts. As inter-role conflicts were subject to social inequality, interventions may pay special attention to employees in lower socioeconomic positions.
Data archiving
There were no data to deposit.
References
Biddle BJ . Recent developments in role theory. Ann Rev Sociol 1986; 12: 67–92.
Greenhaus JH, Beutel NJ . Sources of conflict between work and family roles. Acad Manage Rev 1985; 10: 76–88.
Okechukwu CA, El Ayadi AM, Tamers SL, Sabbath EL, Berkman L . Household food insufficiency, financial strain, work–family spillover, and depressive symptoms in the working class: the Work, Family, and Health Network Study. Am J Public Health 2012; 102: 126–133.
Notten N, Grunow D, Verbakel E . Social policies and families in stress: gender and educational differences in work–family conflict from a European perspective. Soc Indic Res 2016; 132: 1281–1305.
Lee B, Lawson KM, Chang PJ, Neuendorf C, Dmitrieva NO, Almeida DM . Leisure-time physical activity moderates the longitudinal associations between work–family spillover and physical health. J Leis Res 2015; 47: 444–466.
Allen TD, Herst DE, Bruck CS, Sutton M . Consequences associated with work-to-family conflict: a review and agenda for future research. J Occup Health Psychol 2000; 5: 278–308.
Byron K . A meta-analytic review of work–family conflict and its antecedents. J Vocat Behav 2005; 67: 169–198.
Shimazu A, Kubota K, Bakker A, Demerouti E, Shimada K, Kawakami N . Work-to-family conflict and family-to-work conflict among Japanese dual-earner couples with preschool children: a spillover-crossover perspective. J Occup Health 2013; 55: 234–243.
van Steenbergen EF, Kluwer ES, Karney BR . Work–family enrichment, work–family conflict, and marital satisfaction: a dyadic analysis. J Occup Health Psychol 2014; 19: 182–194.
Grzywacz JG . Work–family spillover and daily reports of work and family stress in the adult labor force. Family Relat 2002; 51: 28–36.
Holmes Moyser M How Socioeconomic Status Shapes Individuals’ Experiences of the Work–Family Interface in Canada. University of Toronto: Toronto, Canada, 2015.
Adler N, Stewart J . The MacArthur Scale of subjective social status, 2007. Available at: http://www.macses.ucsf.edu/research/psychosocial/subjective.php.
Siegrist J, Theorell T. Socio-economic position and health: the role of work and employment. In: Siegrist J, Marmot M (eds). Social Inequalities in Health. Oxford University Press: Oxford, UK, 2006, pp 73–100.
Fekete C, Brinkhof MWG, Tough H, Siegrist J . Cohort Profile: a longitudinal study of social participation and wellbeing among persons with spinal cord injury and their partners (pro-WELL). BMJ Open 2017; 7: e011597.
Fekete C, Segerer W, Gemperli A, Brinkhof MW . Participation rates, response bias and response behaviours in the community survey of the Swiss Spinal Cord Injury Cohort Study (SwiSCI). BMC Med Res Methodol 2015; 15: 80.
Brinkhof MW, Fekete C, Chamberlain JD, Post MW, Gemperli A . Swiss National Community Survey on functioning after spinal cord injury: protocol, characteristics of participants and determinants of non-response. J Rehabil Med 2016; 48: 120–130.
Carlson DS, Kacmar KM, Williams LJ . Constructuion and initial validation of a multidimensional measure of work–family conflict. J Voc Behav 2000; 56: 249–276.
Ware JE Jr, Sherbourne CD . The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–483.
WHO The World Health Organization Quality of Life (WHOQOL)-BREF. WHO: Geneva, Switzerland. 2004.
Thompson ER . Development and validation of an internationally reliable short-form of the positive and negative affect schedule (PANAS). J Cross Cult Psychol 2007; 38: 227–242.
Ware JE, Snow KK, Kosinski M, Gandek B . SF-36 Health Survey. Manual and interpretation guide 1993, 26 April 2017. Available at: http://czresearch.com/info/SF36_healthsurvey_ch6.pdf.
Diener E, Suh EM, Lucas RE, Smith HL . Subjective well-being: three decades of progress. Psychol Bull 1999; 125: 276–302.
Geyh S, Fellinghauer BA, Kirchberger I, Post MW . Cross-cultural validity of four quality of life scales in persons with spinal cord injury. Health Qual Life Outcomes 2010; 8: 94.
Watson D, Clark LA, Tellegen A . Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol 1988; 54: 1063–1070.
United Nations Educational, Scientific and Cultural Organization International Standard Classification of Education (ISCED) 2011. UNESCO Institute for Statistics: Montreal, QC, Canada. 2012.
Hagenaars AK, de Vos K, Zaidi MA . Poverty Statistics in the late 1980 s: Research Based on Micro-data. Communities Office for Official Publications of the European Community: Luxembourg. 1994.
Cook WL, Kenny DA . The actor–partner interependence model: a model of bidirectional effects in developmental studies. Int J Behav Dev 2005; 29: 101–109.
Tobin J . Estimation of relationships for limited dependent variables. Econometria 1958; 26: 24–36.
Li K-H, Raghunathan T, Rubin D . Large-sample significance levels from multiply imputed data using moment-based statistics and an F reference distribution. J Am Stat Assoc 1991; 86: 1065–1073.
White IR, Royston P, Wood AM . Multiple imputation using chained equations: issues and guidance for practice. Stat Med 2011; 30: 377–399.
Chandola T, Martikainen P, Bartley M, Lahelma E, Marmot M, Michikazu S et alDoes conflict between home and work explain the effect of multiple roles on mental health? A comparative study of Finland, Japan, and the UK. Int J Epidemiol 2004; 33: 884–893.
Devine CM, Stoddard AM, Barbeau EM, Naishadam D, Sorensen G . Work-to-family spillover and fruit and vegetable consumption among construction laborers. Am J Health Promot 2007; 21: 175–182.
Grzywacz JG, Marks NF . Reconceptualizing the work–family interface: an ecological perspective on the correlates of positive and negative spillover between work and family. J Occup Health Psychol 2000; 5: 111–126.
Cohen S, Herbert TB . Health psychology: psychological factors and physical disease from the perspective of human psychoneuroimmunology. Annu Rev Psychol 1996; 47: 113–142.
Reinhardt JD, Post MW, Fekete C, Trezzini B, Brinkhof MW . Labor market integration of people with disabilities: results from the Swiss Spinal Cord Injury Cohort Study. PLoS ONE 2016; 11: e0166955.
Fekete C, Siegrist J, Reinhardt JD, Brinkhof MW . Is financial hardship associated with reduced health in disability? The case of spinal cord injury in Switzerland. PLoS ONE 2014; 9: e90130.
Kristenson M. Socio-economic position and health: the role of coping. In: Siegrist J, Marmot M (eds). Social Inequalities in Health. Oxford University Press: Oxford, UK, 2006, pp 127–151.
Altman DG, Bland JM . Absence of evidence is not evidence of absence. BMJ 1995; 311: 485.
Hackshaw A . Small studies: strengths and limitations. Eur Respir J 2008; 32: 1141–1143.
Kossek EE, Pichler S, Bodner T, Hammer LB . Workplace social support and work–family conflict: a meta-analysis clarifying the influence of general and work-family-specific supervisor and organizational support. Pers Psychol 2011; 64: 289–313.
Moen P, Fan W, Kelly EL . Team-level flexibility, work-home spillover, and health behavior. Soc Sci Med 2013; 84: 69–79.
Versey HS . Managing work and family: Do control strategies help? Dev Psychol 2015; 51: 1672–1681.
Li A, Shaffer J, Bagger J . The psychological well-being of disability caregivers: examining the roles of family strain, family-to-work conflict, and perceived supervisor support. J Occup Health Psychol 2015; 20: 40–49.
Acknowledgements
We are grateful to all the participants of the pro-WELL study for their time and effort spent in responding to our questions and to the research assistants for their great work in recruitment and data collection. This study has been financially supported by the Swiss National Science Foundation (SNF; Grant Number 100017_153256/1; to MWGB and CF) and by the Swiss Paraplegic Foundation, Nottwil, Switzerland. We also acknowledge the support from the Steering Committee of the SwiSCI cohort study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on the Spinal Cord website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Fekete, C., Siegrist, J., Tough, H. et al. Work and family conflicts in employees with spinal cord injury and their caregiving partners. Spinal Cord 56, 63–70 (2018). https://doi.org/10.1038/sc.2017.100
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2017.100
