
Abstract
Objective:
To assess the effect from maximal bench press strength training (MST) on wheelchair propulsion work economy (WE).
Study design:
Pretest–posttest case–control group design.
Setting:
St Olavs Hospital, Trondheim, Norway.
Methods:
Seventeen male individuals with spinal cord injury (SCI) paraplegia were allocated to either MST bench press (n=11) or the control group (CG) (n=7). The MST group trained bench press three times per week, for 6 weeks, starting at 85–95% of their pretest bench press one-repetition maximum (1RM). For calculation of WE during wheelchair propulsion, oxygen uptake (VO2) measurements were collected during wheelchair ergometry (WCE) at submaximal workload of 50 W. Similarly, peak oxygen uptake (VO2peak) and peak power output (W) were measured during WCE.
Results:
Individuals in the MST regimen significantly improved WE compared with the CG by 17.3 % (mean between-group differences: 95% confidence interval) of 2.63 ml kg−1 min−1: (−4.34, −0.91) (P=0.007). Between pretest and posttest, the increase in bench press 1RM was by 17% higher in the MST group compared with the CG. At peak testing, the MST group generated significantly higher peak power compared with the CG. All other physiological variables were comparable within and between groups.
Conclusions:
A 6-week MST bench press regimen significantly improved WE during wheelchair propulsion at 50 W workload. These preliminary data support a possible beneficial role for MST to reduce the energy cost of wheelchair propulsion for SCI individuals.
Similar content being viewed by others


Introduction
Poor endurance for able-bodied individuals and those with a spinal cord injury (SCI) is related to low force production, low maximal oxygen uptake (V02max) and high oxygen costs at standardized submaximal workloads. As a consequence of paralysis, SCI individuals are dependent on manually propelled wheelchairs for mobility and using their arms during activities of daily living. Compared with the legs, arm work is less efficient and results in a lower physical capacity and consequent limited endurance.1 In addition, because of reduced amount of muscle mass and an impaired sympathetic nervous system, individuals with an SCI have lower physiological responses and metabolic energy expenditure during both rest and training compared with the able-bodied population.2 This, together, equates to a low-peak oxygen uptake (V02peak), low force production and high oxygen costs at standardized submaximal workloads, that is, a poor work economy (WE). Previous studies in able-bodied individuals have shown that maximal strength training (MST) can enhance WE, by lowering the oxygen cost for a given work output.3
The goal of MST is to increase muscle motor unit recruitment and neural drive; this activates more muscle fibers, which links to a stronger muscle contraction.4 Using a MST regimen of high load/few repetitions, with maximal velocity of contraction in the concentric action, the present study aimed to investigate the effects of MST in terms of altering WE for individuals with an SCI. A recent study showed that, for a small cohort of able-bodied individuals, a MST conditioning regimen was more effective than conventional strength training in terms of improving WE and maximal strength.5 The underlying basis for this improvement was reduced oxygen uptake (VO2) during submaximal exercise, attributable solely to skeletal muscle.6 MST of the legs has also been shown to be of therapeutic value for the work inefficiency seen in patients with chronic obstructive pulmonary disease.7 In contrast to these studies, there have been comparatively few attempts to establish whether similar benefits could be achieved for individuals with an SCI. The reliance on upper body strength for individuals with paraplegia may, for example, influence their performance following MST training relative to able-bodied individuals. Recent studies for individuals with such injuries have demonstrated significantly increased strength and arm power after bench press training8, 9 or general strength exercises9, 10 but without the measurements of WE performed during wheelchair ergometry (WCE), which are regarded as a critical functional metric for the mobility of SCI individuals.
Training specificity implies that the neuromuscular system will adapt only to those demands placed on the body by the exercise program.11 Interestingly, however, Turbansky and Schmidtbleicher8 have shown that bench press exercises increase wheelchair sprint performance in SCI individuals even though bench pressing does not mimic hand-rimmed wheelchair propulsive movements. Ordinarily we would presume that any ‘carryover’ effects from bench press MST would be unlikely to influence WE and peak power output during wheelchair propulsion.
Given that it remains unclear as to whether bench press MST exercises in SCI individuals may improve WE during wheelchair propulsion, we designed this study in order to investigate this possibility, by comparing performance after MST training versus no formalized exercise routine. The primary outcomes were designated as WE and strength development (one-repetition maximum (1RM)); the secondary outcomes included VO2peak, blood lactate concentration ([La−]b), ratings of perceived exertion, heart rate, power output (W) and body mass (kg).
Materials and methods
Study design and population
A pretest–posttest, case–control, group design was used. Seventeen male paraplegics with American Spinal Cord Association Impairment Scale A to D were allocated to MST (n=11) and control (n=7) groups. The eligible participants were assigned to each group, open label. Participants were recruited from our departmental patient list and assigned to either MST or the control group (CG) based on the assessor’s judgment and a participant interview. The participants were diagnosed to be in stable neurological recovery. Individual characteristics are shown in Table 1.
Candidate SCI individuals with pacemakers, cancer, severe autonomic dysreflexia, a prior history of lung disease, respiratory failure, gross joint contractures, decubital ulcers, acute shoulder girdle or shoulder joint tendonitis were excluded. None of the included participants were actively participating in systematic strength training and experienced weight lifters or wheelchair racing athletes. One candidate was a Paralympic ice sledge-hockey athlete for the Norwegian National team, however, not experienced with MST bench press.
We certify that all applicable institutional and governmental regulations concerning the ethical study of human volunteers were followed during the course of this research. Our study was approved by the Regional Committee for Medical and Health Research Ethics; all participants provided signed informed consent prior to their participation.
Test equipment and measurements
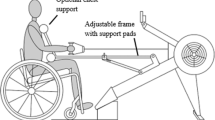
Strength tests (1RM) and training were performed using an adjustable bench press and calibrated Eleiko Olympic (Eleiko AB, Halmstad, Sweden) version sports barbell (20 kg, 2.85 cm diameter, 2.20 m long) with weights. All participants lifted while lying supine on a plinth strapped with a Velcro band around their waist for stability. Power in Watt (W), force in Newton (N) and velocity (m s−1) were recorded using the MuscleLab model 4000e, V.8.10 (Ergotest Innovation a.s., Porsgrunn, Norway) connected to a personal computer. A linear encoder (ET-Enc-02, Ergotest Innovation a.s.) with a resolution of 0.07 mm (smallest detectable motion) and sampling frequency of 100 Hz was strapped to the barbell to measure vertical displacement and velocity. The maximal measurement error of the MuscleLab system is less than 0.3, 0.9 and 1.2% for force, velocity and power, respectively. A VP100 Handisport (Medical Development, Varces-Allières-et-Risset, France) was used for WCE.12 Prior to testing, all equipment was calibrated. The WCE measures were calibrated by recording the total frictional rolling resistance (residual torque/moment of inertia) of zero loads with the SCI individuals in their personal rigid-frame wheelchairs fixed to the VP100 Handisport. SCI individuals propelled their wheelchair on the wheelchair ergometer for 5−10 min prior to testing to become accustomed to the test equipment and to limit carryover effects.
Ventilation parameters and pulmonary gas exchange measurements were performed by using the portable Metamax II Cortex system (Cortex Biophysik GmbH, Leipzig, Germany). The volume range and accuracy were 0.01−14.0 l s−1 and 1.5%, respectively; the oxygen concentration range and accuracy were 0−25 volume % and <0.1 volume %, respectively. Carbon dioxide was analyzed using an infrared sensor with a range from 0 to 10 volume % and an accuracy of <0.1 volume %. A facemask mounted with the volume transducer and assembly tube for the O2 and CO2 sensors was fitted to the individuals during all tests.
Hemolyzed blood lactate concentration ([La−]b in mmol l−1) was measured within 1 min after the termination of VO2peak tests using the Lactate Pro Analyzer LT-1710 (Arkray Factory, Inc., KDK Corp., Tokyo, Japan), which has an accuracy (CV) of 3%. Heart rate was measured using a Polar monitor (Polar Electro, Oy, Finland), accurate to ±1 heartbeat per minute (Polar Operation manual, Polar Electro, 1997). The Borg scale from 6 to 20 (Borg 1970) was used for subjective rating of perceived exertion during WCE50w and VO2peak.
Determination criteria for VO2peak
Combined with a respiratory exchange ratio of ⩾1.1, [La−]b ⩾7 and rating of perceived exertion ⩾15 (Borg 6−20), VO2peak was considered achieved. In the upper body mode, a VO2 plateau (a VO2 plateau, despite an increase in power output and pulmonary ventilation) is rarely reached, and therefore VO2peak is used to denote maximal effort. If these criteria were met, the average of the highest VO2 values within three consecutive 10 s measurements was calculated as VO2peak.
Protocol for testing 1 RM strength and power:
-
i)
Before testing, the participants warmed up for 10 min on an arm crank ergometer, followed by barbell lifts with no added weight, for optimizing the bench press technique. To secure a grip at the same position, the fifth finger was placed at the circular barbell markings (91 cm marks). The investigator assisted in the preload phase until the individuals had fully extended their arms. The barbell was then lowered in a controlled tempo. The barbell was lifted with emphasis on intended maximal velocity, and movement range, in the concentric phase. Bouncing the barbell at the chest was prohibited.
-
ii)
To determine each participant’s 1RM, load was added (three to five times) with intervening 5-min rest periods, until the 1RM value was reached. The 1RM value was accepted when completion of the entire lift was performed in a controlled way, without assistance (as described above).
-
iii)
To measure power, a load of 70% of 1RM was used with the best of the three trials recorded for data analyses. As considerable progression was expected, a value of 70% of 1RM was chosen to allow for the predicted increase in maximal power following training. Moreover, 70% of 1RM ought to optimize the relative trajectory on which the peak instantaneous power output curve is reached3 (force–velocity curve), even during a dynamic bench press.
Protocol for testing WE and VO2peak during WCE:
-
i)
4 min at a submaximal load of 30 W directly followed by
-
ii)
4 min at 50 W; when VO2 values were unchanging within three consecutive 10-s measurements, average VO2 values were calculated.
-
iii)
6−10-min peak test consisting of increasing 10−20 W in 1-min increments until volitional fatigue.
Training protocol
MST group: Nine SCI individuals trained bench press 3 days per week for 6 weeks, with four sets of four repetitions (4 × 4) at 85−95% of individual pretest bench press 1RM. The emphasis on maximal mobilization of force in the concentric phase was stressed. The sets were interspersed with 30-s brakes. When individuals managed four repetitions in four sets, the load was increased by approximately 2.5−5.0 kg for the next training session. In total, the bench press training took approximately 60 min per week. The CG performed no formalized exercise routine.
Statistical analyses
After an initial analysis of equality of variance, two-sample t-tests were used to compare the differences between groups prior to testing followed by analyses (posttest–pretest) within and between the MST and CG. Non-parametric Wilcoxon signed-rank tests were used for ordinal scale values. Values are expressed as mean (s.d.), median (range) or mean difference between groups, after test (95% confidence interval (CI)). Significance was accepted at P<0.05.
Results
WE during WCE at 50 W (Table 2) improved by 17.3% for the MST group, as indicated by a reduction in VO2 consumption. The mean (95% CI) reduction and difference in oxygen consumption between groups was −2.6 ml kg−1 min−1 (−4.3, −0.9) in favor of the MST group (P=0.007) (Table 2).
After 6 weeks of training, the mean (s.d.) 1RM force increased significantly in the MST group from 70.8 (16.0) to 82.4 (17.3) kg (P=0.001). For the 1RM variable, the difference in the mean (95% CI) between groups was 11.6 (6.7, 15.4) kg. No differences were observed in the CG. The mean difference (95% CI) of peak power (W) during WCE between groups was significantly (P=0.001) improved for the MST group, that is, 8.1 (3.7, 12.5) (Table 3). No changes within and between groups in VO2peak, (ml kg−1 min−1, l min−1), heart rate (beats min−1), body mass (kg) and [La−]b (mmol l−1) were observed following training in the MST group or after the equivalent pretest−posttest measurement delay in the CG.
At baseline, there were no significant differences between the MST and CG in terms of demographics or physiological characteristics (Tables 1, 2, 3, 4). Of the 11 initially included in the MST group, two participants withdrew because of shoulder pain from latent shoulder joint tendonitis. The MST group completed >95% of the 18 training sessions.
Discussion
The novel finding in this preliminary study is that 6 weeks of maximal bench press strength training at 85−95% of 1RM with focus on maximal mobilization of force in the concentric phase significantly improved wheelchair propulsion WE. This was reflected by a lower oxygen cost (2.63 ml kg−1 min−1) at a standardized submaximal workload of 50 W. In terms of tangible benefits, the improvement in WE may translate to the potential of performing significantly more work, or the same amount of work, with less effort. Thus a training regimen with high loads and few repetitions can lead to functional improvements in wheelchair propulsion, which is a critical activities of daily life determinant for the quality of life for SCI individuals.2, 3, 4 The 17% improvement in WE, achieved from a 16% increase in the 1RM value, agrees with previous data collected for chronic obstructive pulmonary disease patients.7 Although Barrett-O'Keefe et al.6 suggested that an improved WE was the result of reduced oxygen uptake by working muscle, the actual intramuscular mechanism responsible for the improved WE has yet to be proven.
Individuals with an SCI require strength and power training to improve their mobility. This study revealed significant strength, power and velocity improvements following MST (Table 4). Strength gains from resistance exercise are twofold and include both muscular and neural adaptations. The initial improvement in strength achieved by progressive MST is characterized primarily by neural and then muscular adaptations.13, 14, 15 Thus heavy loading contributed to maximizing strength, power and velocity gains. These performance criteria are likely to be distinct from those that arise from conventional training, which may instead favor endurance adaptations.
The significant increase in peak power (POpeak) in the MST group indicated an improved working capacity at peak performance. We also concluded that SCI individuals were able to perform at a higher POpeak because of their increased 1RM. This conclusion was based on the non-significant difference in heart rate, or blood lactate concentration [La−]b, and VO2peak between and within groups between pretest and posttest. [La−]b did not change after training, indicating that these SCI individuals were able to perform at higher POpeak because of their increased 1RM. Thus the strength gains associated with this MST regimen appear transferable to WCE at 50 W and also to WCE at POpeak. This is a novel finding, especially as bench press training does not authentically mimic the demands of wheelchair propulsion. Therefore, the general concept of the specificity of resistance training would appear to be challenged by these findings.
Aerobic upper body arm exercise is limited by the relatively small and less powerful muscle mass, limited capillary density, reduced mean blood transit time and smaller oxidative capacity compared with muscles of the lower extremities.16 Individuals who are dependent on their arms for mobility may therefore struggle to achieve sufficient strength and power for functional independence. In a recent prospective 1-year follow-up multicenter study, Haisma et al.17 documented an increase in mean peak power output of 10 W, associated with an almost four-point improvement in the functional independence measure (FIM) motor score. POpeak was therefore suggested to be an objective measure, with positive predictive value for the rehabilitation of wheelchair-dependent SCI individuals. The same authors also found that FIM was significantly associated with VO2peak and muscle strength. Our study documented a 16% increase in muscle strength (1RM) and a 7% increase in peak power output (POpeak). Although determining the basic activities of daily life via FIM scores was not the objective of the present study, it is possible that the documented improvements in both strength and peak power output could lead to greater functional independence for individuals with an SCI. However, further studies are needed to verify this conclusion.
Muscular power is the product of force generation and movement velocity and is an important testing variable. The improved strength (1RM) achieved by individuals with an SCI in this study would appear to correlate with the improved WE. Moreover, these findings are further substantiated by the significant increase in peak and mean velocities, as well as power variables, during 70%–1RM testing. The power increase achieved by MST appears to have lowered the standard submaximal load at WCE 50 W. Previous SCI studies10, 18 reported increased muscle strength and power by circuit resistance training programs. However, there were corresponding increases in both VO2peak18 and endurance,10 as circuit resistance training programs employ a wide variety of strength and endurance exercises. Thus, when combining resistance and aerobic exercises, an increase in VO2peak is expected. In contrast, VO2peak is not expected to change when using MST alone.
Two of the 11 SCI individuals in the MST group were forced to withdraw because of shoulder pain due to latent shoulder joint tendonitis at the beginning of the study. In such case, the MST protocol should be initiated at a lower intensity, with loading at inclusion, to accommodate for any latent shoulder disease.
Conclusion
In comparison with the CG, a 6-week MST bench press regimen with training intensities between 85% and 95% of the 1RM value significantly reduced oxygen cost during wheelchair propulsion at a 50-W submaximal workload. These data support a possible beneficial role for MST in SCI treatment.
Study limitations
This is an open label study, where neither the participants nor the assessors were blinded. Therefore, we acknowledge that this may have introduced systematic, although inadvertent, bias. Similarly, outcome measurements may have suffered a similar bias. Cautious interpretation of our data is therefore warranted, and our findings should be regarded as preliminary. For some SCI individuals, the thrice weekly MST regimen was considered time consuming and priority to participate was given different among respondents. The effects of MST on work physiology, and VO2 dynamics during wheelchair propulsion, should now be repeated using blinded, high-quality trials, before MST for individuals with an SCI can be widely encouraged.
Data archiving
There were no data to deposit.
References
Bergh U, Kanstrup IL, Ekblom B . Maximal oxygen uptake during exercise with various combinations of arm and leg work. J Appl Physiol 1976; 41: 191–196.
Price M . Energy expenditure and metabolism during exercise in persons with a spinal cord injury. Sports Med 2010; 40: 681–696.
Hoff J, Gran A, Helgerud J . Maximal strength training improves aerobic endurance performance. Scand J Med Sci Sports 2002; 12: 288–295.
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P . Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol (1985) 2002; 93: 1318–1326.
Heggelund J, Fimland MS, Helgerud J, Hoff J . Maximal strength training improves work economy, rate of force development and maximal strength more than conventional strength training. Eur J Appl Physiol 2013; 113: 1565–1573.
Barrett-O'Keefe Z, Helgerud J, Wagner PD, Richardson RS . Maximal strength training and increased work efficiency: contribution from the trained muscle bed. J Appl Physiol (1985) 2012; 113: 1846–1851.
Hoff J, Tjønna AE, Steinshamn S, Høydal M, Richardson RS, Helgerud J et al. Maximal strength training of the legs in COPD: a therapy for mechanical inefficiency. Med Sci Sports Exerc 2007; 39: 220–226.
Turbanski S, Schmidtbleicher D . Effects of heavy resistance training on strength and power in upper extremities in wheelchair athletes. J Strength Cond Res 2010; 24: 8–16.
Pelletier CA, Totosy de Zepetnek JO, MacDonald MJ, Hicks AL . A 16-week randomized controlled trial evaluating the physical activity guidelines for adults with spinal cord injury. Spinal Cord 2015; 53: 363–367.
Hicks AL, Martin KA, Ditor DS, Latimer AE, Craven C, Bugaresti J et al. Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord 2003; 41: 34–43.
Mooren F. Encyclopedia of Exercise Medicine in Health and Disease. Springer: Berlin, Germany, 2012..
Devillard X, Calmels P, Sauvignet B, Belli A, Denis C, Simard C et al. Validation of a new ergometer adapted to all types of manual wheelchair. Eur J Appl Physiol 2001; 85: 479–485.
Behm DG, Sale DG . Velocity specificity of resistance training. Sports Med 1993; 15: 374–388.
Almasbakk B, Hoff J . Coordination, the determinant of velocity specificity? J Appl Physiol 1996; 81: 2046–2052.
Fimland MS, Helgerud J, Gruber M, Leivseth G, Hoff J . Functional maximal strength training induces neural transfer to single-joint tasks. Eur J Appl Physiol 2009; 107: 21–29.
Shephard RJ, Bouhlel E, Vandewalle H, Monod H . Muscle mass as a factor limiting physical work. J Appl Physiol 1988; 64: 1472–1479.
Haisma JA, Post MW, van der Woude LH, Stam HJ, Bergen MP, Sluis TA et al. Functional independence and health-related functional status following spinal cord injury: a prospective study of the association with physical capacity. J Rehabil Med 2008; 40: 812–818.
Jacobs PL, Nash MS, Rusinowski JW . Circuit training provides cardiorespiratory and strength benefits in persons with paraplegia. Med Sci Sports Exerc 2001; 33: 711–717.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Tørhaug, T., Brurok, B., Hoff, J. et al. The effect from maximal bench press strength training on work economy during wheelchair propulsion in men with spinal cord injury. Spinal Cord 54, 838–842 (2016). https://doi.org/10.1038/sc.2016.27
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.27
