
Abstract
Study design:
Randomized longitudinal comparative study.
Objectives:
To compare the efficacy of lamotrigine and amitriptyline in the management of traumatic spinal cord injury (SCI)-induced neuropathic pain (NP).
Setting:
Sawai Man Singh Medical College and Hospital, Jaipur, India.
Methods:
A total of 147 individuals with NP were randomized for a 3-week trial of either amitriptyline or lamotrigine. Amitriptyline was administered orally at doses of 25, 50 and 100 mg once daily at night time, and lamotrigine was administered orally at doses of 25, 50 and 100 mg twice daily, both for 1 week by means of optional titration. Assessment of NP was done at baseline and thereafter at 1, 2 and 3 weeks using Short–form MC Gill Pain Questionnaire-2 (SFMPQ2) scores.
Results:
There was a significant difference between the mean values of the SFMPQ2 score at baseline and those at each follow-up for amitriptyline. Similar results were seen in the lamotrigine group. When the differences in mean SFMPQ2 scores at different time frames from baseline were compared with those of the other group, values were found to be nonsignificant as seen on the Mann–Whitney U-test.
Conclusions:
These findings support the use of both amitriptyline and lamotrigine in the management of NP after traumatic SCI.
Similar content being viewed by others

Introduction
Traumatic spinal cord injury (SCI) is one of the most devastating types of injury and it results in varying degrees of paralysis, sensory loss and bladder/bowel dysfunction. In SCI patients, pain has a major impact in terms of reduced quality of life, functional impairment and restrictive social participation.
The average reported figure for the prevalence of chronic SCI-induced neuropathic pain (NP) is ~70%; one-third of patients describe it as an intense pain having a negative impact on their mood and activities of daily living.1 Pain can slow down or even interrupt a rehabilitation program and be a major hurdle to a normal social life. When pain is not adequately managed or even neglected, it leads to physical and psychological disorders that are difficult to treat and can trigger a chronic pain syndrome.
Different types of pain are commonly observed in SCI patients, and taxonomy was proposed in 2012 as the International Spinal Cord Injury Pain (ISCIP) Classification.2 It has a three-tiered division: tier 1 divides pain according to pain type—that is, nociceptive, neuropathic, other pain and unknown pain; tier 2 describes the pain subtype; and tier 3 describes the primary pain source. Tier 2 subcategories for NP are: at level SCI pain, below level SCI pain and other NP (not directly related to SCI). Among all pain types, chronic NP poses real problems in terms of identification and therapeutic strategies.
NP was defined3 by the International Association for the Study of pain (IASP) as ‘pain caused by a lesion or disease of the somatosensory nervous system.’ It is present in 40–50% of individuals having SCI, usually develops within 1 year and tends to become chronic.4
Individuals with NP usually complain of spontaneous burning pain that is continuously present and may be accompanied by dysesthesias, often described as tingling or prickling, or may also describe electric shock or stabbing sensations that are intermittent. Some patients describe being hypersensitive in the area of NP, referring to the pain that is induced by light touch or moderate thermal stimuli (that is, allodynia) and to particularly severe pain elicited by normally mild nociceptive stimuli (that is, hyperalgesia).
Evidence-based symptomatic pharmacotherapy is the mainstay of the treatment of NP and it should be titrated individually according to the efficacy and possible contraindications or side-effects. NP is treated mainly with antidepressants and antiepileptics, whereas simple analgesics have not shown efficacy for this type of pain. Antidepressants have been used to treat pain in a number of populations and have been shown to have some benefit in conditions like diabetic neuropathy and fibromyalgia; however, only a limited number of studies have examined their use in post SCI NP. To our knowledge this is the first comparative study between amitriptyline and lamotrigine in the treatment of NP in persons with SCI. The objective of our study was to compare the effectiveness of amitriptyline with that of lamotrigine in NP following traumatic SCI.
Materials and methods
Subjects
Patients enrolled in the study were inpatients of the Department of Physical Medicine and Rehabilitation, SMS Medical College and hospital, Jaipur. Individuals aged 18 years and above with SCI-induced NP were eligible for the study. Written and informed consent was taken from each individual. History of cardiovascular diseases, seizures, hyperthyroidism or glaucoma or any known psychiatric illness and allergy to drugs used in this study were the exclusion criteria.
Baseline information including age, sex, education level, occupation, marital status, mechanism of injury, associated complications, dietary habits, family monthly income, family type, ASIA (American Spinal Injury Association) scale, neurological level, site, quality, time of onset and duration of NP were recorded.
The present study was approved by the ethics committee of Sawai Man Singh Medical College and Hospital Jaipur with reference number 2146/MC/EC/2016, which is in accordance with the Declaration of Helsinki.
Study design and procedure
This is a randomized, longitudinal, comparative study. Along with detailed clinical examination and radiological assessment, daily counseling for pain was also done. Motor and sensory examination was performed according to the Standards of the ASIA impairment scale and assessment of NP was made on the basis of DN4 (Douleur Neuropathic en 4 questions) score.5
Written informed consent was obtained for the study. All study patients were randomized into two groups, one for amitriptyline and the other for lamotrigine, by computer-generated randomized numbers.
DN4 was designed to discriminate between neuropathic and non-NP The tool was developed and validated in French and was translated into many languages. It consists of 10 items divided into seven symptoms and three items related to clinical examination. It includes two questions addressing symptoms:
-
1
Pain quality (presence of three symptoms assessed: burning, painful cold, electric shocks).
-
2
Non-painful symptoms (presence of four symptoms assessed: numbness, tingling, itching, pins-and-needles).
and two questions addressing sensory signs:
-
1
Assessment for mechanical hypoesthesia (two modalities assessed: touch and pinprick sensations).
-
2
Assessment for mechanical dynamic allodynia (one modality assessed: brushing).
Each of the 10 items is scored on a binary scale of ‘Yes’ or ‘No’. A total score ranging from 0 to 10 is calculated by summing the ‘Yes’ responses. A cutoff score of 4 has been identified by the developers as indicating NP.
All patients were evaluated for pain at baseline using the SFMPQ2.6 The patients in the amitriptyline group were started on an initial dose of 25 mg once daily and patients in the lamotrigine group were started on an initial dose of 25 mg twice daily. Short–form MC Gill Pain Questionnaire-2 (SFMPQ2) scores were reviewed at first follow-up (7th day), and doses were titrated to 50 mg once daily for amitriptyline and 50 mg twice daily for lamotrigine if no improvement (reduction in SFMPQ2 score values to half or more) or no adverse effects were observed by the treating physician. At the second follow-up (14th day), scores were reviewed and double the previous dose was given if no improvement or side-effects were observed. Final evaluation of SFMPQ2 scores was at third follow-up (21st day).
Outcome measure
Patients rated their average overall pain on the SFMPQ2 scale.
SFMPQ2 is composed of 22 items investigating four dimensions: continuous pain (Item 1, 5, 6, 8–10); intermittent pain (Items 2–4, 11, 16, 18); NP (Items 7, 17,19–22); and affective descriptors (Item 12–15). Each descriptor is rated on an 11-point Numeric rating scale ranging from 0=‘none’ to 10=‘worst possible’. Subscale scores are computed by calculating the mean ratings for subscale descriptors. Total score is the mean of the four subscale scores.
Statistical analysis
Intention-to-treat analysis was performed. The mean difference in SFMPQ2 scores from baseline on the 7th day (D-7), 14th day (D-14) and 21st day (D-21) was calculated for both drugs. The Friedman test was applied for D-7, D-14 and D-21 in the amitriptyline group, and post hoc analysis was done using the Wilcoxon signed rank test for each pair of follow-up time points—that is, D-7 and D-14, D-7 and D-21, D-14 and D-21. A similar assessment was made in the lamotrigine group. Comparative analysis of mean difference at various check points was done for both groups using the Mann–Whitney U-test. P-values <0.05 were taken as significant.
Statement of ethics
I certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Results
Patients
There were a total of 147 patients, of whom 136 were male and 11 were female; 109 (74%) were in the age group of 18–40 years. A total of 83 (56%) were tetraplegics and 64 (44%) were paraplegics. According to ASIA, 112 (76%) were in grade A (neurologically complete), and the remaining 35 (24%) belonged to the neurologically incomplete category (B-D).
Outcome measure
The P-value was significant for the mean difference in SFMPQ2 score from baseline at different follow-up time points—that is, 7th, 14th and 21st day—for the amitriptyline group (Table 1).
When post hoc analysis was conducted using the Wilcoxon Signed Rank test for each pair of follow-up time points, the P-value was found to be significant for each comparison (Table 2).
Significant changes were also seen in the lamotrigine group (Tables 3 and 4).
On application of the Mann–Whitney U-test between the amitriptyline and lamotrigine groups, comparing differences in mean SFMPQ2 scores from baseline on the 7th day (D-7), 14th day (D-14) and 21st day (D-21), the P-value was found to be nonsignificant at all three stages (Table 5).
Adverse events
Of the 74 studied patients on amitriptyline, only 10 reported one or more side-effects. The most common side-effects reported were dry mouth and drowsiness. Patients reported these adverse effects at doses exceeding 50 mg once daily. None of the patients on lamotrigine experienced any adverse events.
Withdrawn patients
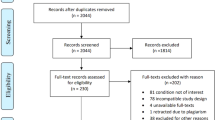
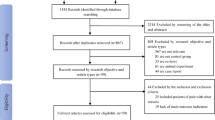
A total of 147 subjects who satisfied the inclusion criteria were enrolled for study purpose. Of them, only 140 completed the 21-day follow-up period. One case dropped out at 1st follow-up, one at 2nd follow-up and three at 3rd follow-up. Two patients died during the study.
Discussion
Different questionnaires have been developed to differentiate NP from other types of pain. In SCI patients, good reliability has been shown in particular for the DN4 questionnaire. It was developed by Didier Bouhassira et al.5 and consists of both sensory descriptors and signs related to bedside sensory examination. In a study conducted by Hallstrom et al.,7 the DN4 questionnaire was found to have maximum sensitivity (93%) and diagnostic accuracy (88%) with low specificity (75%) among the four scales used in individuals with SCI and pain.
Recent advances in identifying the mechanisms of NP and in improving its management have led to the development of new instruments designed to measure the unique aspects of pain. The SFMPQ score has been used successfully in treatment trials of NP. However, it does not contain certain descriptors that have been shown to be reliably associated with NP conditions. Dworkin et al.6 developed the SFMPQ2, an expanded and revised version of the SFMPQ, designed to measure the qualities of both neuropathic and non-NP in research and clinical settings. They found that the SF- MPQ-2 has excellent reliability and validity, and results of both exploratory and confirmatory factor analysis revealed the presence of the following four factors or subscales—continuous pain; intermittent pain; predominantly NP; and affective descriptors. The following modifications were involved in the development of the SFMPQ2: (1) inclusion of seven new descriptors relevant to NP; (2) use of an 11-point Numeric rating scale for each descriptor; (3) addition of the qualifier ‘pain’ to 13 descriptors; and (4) expansion of the instructions to take into account ‘different qualities of pain and related symptoms.
NP after SCI is characterized by loss of sensory modalities mediated by spinothalamic tract neurons, and abnormal pain perception (spontaneous continuous pain and abnormally evoked pain). Abnormal pain perception results from neuronal hyperactivity and hyper-excitability induced by abnormal impulse generation in damaged spinothalamic tract neurons. The neurochemical changes include increased excitatory glutaminergic activity involving N-methyl-d-aspartate receptor activation, changes in sodium ion channels and voltage-gated calcium channels. Other important mechanisms may be loss of endogenous inhibition, including reduced GABAergic, opioid and monoaminergic inhibition.
Lamotrigine acts at voltage-sensitive sodium channels to stabilize the neuronal membrane and inhibit sodium influx-mediated pathological release of excitatory amino-acid transmitters, principally glutamate; both are involved in neuronal hyper-excitability, which is an important mechanism of NP. Action of amitriptyline is multimodal, with contribution of monoamine reuptake inhibition and N-methyl-d-aspartate receptor and sodium channel blockade. Previously conducted studies on these drugs mentioned that there might be variable effects of drugs on NP in SCI individuals owing to a multimodal mechanism of action.
Three open studies of poor quality, two prospective (level 3) and one retrospective (level 4), suggested the efficacy of tricyclic antidepressants (mainly amitriptyline) combined with other treatments on SCI pain.8, 9, 10
More recently, two double-blind studies also compared the efficacy of amitriptyline with an ‘active’ placebo (mimicking the side-effects of tricyclic antidepressants) in patients with SCI pain. Cardenas et al.11 studied amitriptyline in 84 patients of SCI pain with dose range from 10 to 125 mg over 6 weeks and failed to show any significant superiority of it over placebo. In this study, non-neuropathic SCI pain was also included. The median maximum and week-6 dose was 50 mg per day. These negative data, which are in contrast with most study results, could be due to low dosages of amitriptyline and the poor assessment of NP. In fact, the main efficacy outcome of this study was pain in general (including musculoskeletal and visceral pain) as the trial did not compare treatment effects within subgroups of pain types.
Rintala et al.12 conducted a randomized controlled, double-blind, triple cross-over 8-week trial study in 22 patients comparing the effects of amitriptyline, gabapentin or an active control (diphenhydramine) in the treatment of NP post SCI and found a moderate efficacy of high-dosage amitriptyline (150 mg per day) compared with gabapentin and placebo, but only in a subgroup of patients with depressive symptoms, suggesting that the analgesic effect of amitriptyline was related to its antidepressant efficacy.
Tricyclic antidepressants induced several adverse effects in both studies, consisting mainly of dry mouth, constipation, along with aggravation of spasticity and dysuria, which can be a genuine concern in the context of SCI.
In the present study, amitriptyline was found to be effective in the management of NP after traumatic SCI as the mean difference in SFMPQ2 score at a different time frame from baseline was significant. Of the 74 study patients on amitriptyline, only ten reported one or more side-effects. The most common side-effects reported were dry mouth and drowsiness, and patients reported these adverse effects at doses exceeding 50 mg once daily.
One placebo-controlled study on lamotrigine13 in traumatic SCI patients (with pain at or below level) did not show efficiency in pain outcomes. However, in a post hoc analysis, lamotrigine was found effective in a subgroup of patients (n=7) with incomplete SCI and mechanical allodynia (to brush) at level. A Cochrane review on lamotrigine14 for chronic NP and fibromyalgia in adults published in 2013 included twelve studies in 11 publications (1511 participants), all with chronic NP: central post-stroke pain (1); chemotherapy-induced NP (1); diabetic neuropathy (4); HIV-related neuropathy (2); mixed NP (2); SCI-related pain (1); and trigeminal neuralgia (1). Lamotrigine did not help the pain, and was no different from placebo except in causing more side-effects. But it is important to mention here that only one study on SCI was involved in the Cochrane review with 22 participants, and in this trial lamotrigine reduced NP among incomplete SCI patients.
Lamotrigine was found to be effective in our experience in the management of NP after traumatic SCI as the mean difference in SFMPQ2 score at different time frames from baseline was significant. None of the patients on lamotrigine experienced any adverse events.
To our knowledge, this is the first study comparing the effectiveness of amitriptyline and lamotrigine in the treatment of NP in SCI patients. Earlier Jose et al.15 compared the efficacy and safety of lamotrigine and amitriptyline in controlling chronic painful peripheral neuropathy in diabetic patients in a randomized, double-blind, cross-over, active control, clinical trial with variable dose titration (n =53). This study showed similar benefits of both treatments; lamotrigine might be the first choice in peripheral NP as it is associated with fewer adverse events.
Our results showed that both amitriptyline and lamotrigine were similarly effective in the management of NP after traumatic SCI as the difference in mean SFMPQ2 from baseline at various follow-up time points was found to be significant for each drug separately. But on comparing differences in mean SFMPQ2 scores between two groups, the result was nonsignificant, suggesting that no drug was better than the other.
The prevalence of NP was not recorded, as the inclusion criteria of this study encompassed SCI patients having NP. Also denominator data for calculating prevalence were not recorded. The strength of the study was the large and complete follow-up and fewer dropouts.
In conclusion, comprehensive knowledge of the clinical characteristics of pain is important for proper management. The present study demonstrated the effectiveness of both amitriptyline and lamotrigine in SCI-induced NP; no difference in efficacy was noted between the two drugs. Because different mechanisms underlie SCI pain, it emphasizes the need for mechanism-based classification of patients with NP. Further large clinical studies are needed for established and novel management options.
Data archiving
There were no data to deposit.
References
Felix ER . Chronic neuropathic pain in SCI: evaluation and treatment. Phys Med Rehabil Clin N Am 2014; 25: 545–571.
Bryce TN, Biering-Sørensen F, Finnerup NB, Cardenas DD, Defrin R, Ivan E et al. International spinal cord injury pain (ISCIP) classification Part 2. Initial validation using vignettes. Spinal Cord 2012; 50: 404–412.
Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS et al. A new definition of neuropathic pain. Pain 2011; 152: 2204–2205.
Margot-Duclot A, Tournebise H, Ventura M, Fattal C . What are the risk factors of occurrence and chronicity of neuropathic pain in spinal cord injury patients? Ann Phys Rehabil Med 2009; 52: 111–123.
Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J et al. Comparison of pain syndromes associated with nervous or somatic lesion and development of a new neuropathic pain diagnostic questionnaire [DN4]. Pain 2005; 114: 29–36.
Dworkin RH, Turk DC, Revicki DA, Harding G, Coyne KS, Peirce-Sandner S et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain 2009; 144: 35–42.
Hallstrom H, Norrbrink C . Screening tools for neuropathic pain: can they be of use in individuals with spinal cord injury? Pain 2011; 152: 772–779.
Erzurumulu A, Dursun H, Gunduz S . The management of chronic pain in spinal cord injured patients. The comparison of effectiveness of amitriptyline and carbamazepine combination and electroacupuncture application. J Rheumatol Med Rehabil 1996; 7: 176–180.
Fenollosa P, Pallares J, Cervera J, Pelegrin F, Inigo V, Giner M et al. Chronic pain in the spinal cord injured: statistical approach and pharmacological treatment. Paraplegia 1993; 31: 7229.
Heilporn A . Two therapeutic experiments on stubborn pain in spinal cord lesions: coupling melitracen-flupenthixol and the transcutaneous nerve stimulation. Paraplegia 1977; 15: 368–372.
Cardenas DD, Warms CA, Turner JA, Marshall H, Brooke MM, Loeser JD . Efficacy of amitriptyline for relief of pain in spinal cord injury: results of a randomized controlled trial. Pain 2002; 96: 365–373.
Rintala DH, Holmes SA, Courtade D, Fiess RN, Tastard LV, Loubser PG . Comparison of the effectiveness of amitriptyline and gabapentin on chronic neuropathic pain in persons with spinal cord injury. Arch Phys Med Rehabil 2007; 88: 1547–1560.
Finnerup NB, Sindrup SH, Bach FW, Johannesen IL, Jensen TS . Lamotrigine in spinal cord injury pain: a randomized controlled trial. Pain 2002; 96: 375–383.
Wiffen PJ, Derry S, Moore RA . Lamotrigine for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev 2013; 12: 1–47.
Jose VM, Bhansali A, Hota D, Pandhi P . Randomized double blind study comparing the efficacy and safety of Lamotrigine and Amitryptilline in painful diabetic neuropathy. Diabet Med 2007; 24: 377–383.
Acknowledgements
I gratefully acknowledge the contributions by Dr Deepak Gupta in statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Agarwal, N., Joshi, M. Effectiveness of amitriptyline and lamotrigine in traumatic spinal cord injury-induced neuropathic pain: a randomized longitudinal comparative study. Spinal Cord 55, 126–130 (2017). https://doi.org/10.1038/sc.2016.123
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.123
This article is cited by
-
Neuropathic Pain and Spinal Cord Injury: Management, Phenotypes, and Biomarkers
Drugs (2023)
-
Pharmacologic therapies of pain in patients with spinal cord injury: a systematic review
Spinal Cord Series and Cases (2022)
-
The CanPain SCI clinical practice guidelines for rehabilitation management of neuropathic pain after spinal cord injury: 2021 update
Spinal Cord (2022)
-
Pregabalin and Gabapentin in Patients with Spinal Cord Injury-Related Neuropathic Pain: A Network Meta-Analysis
Pain and Therapy (2021)
-
Membrane Stabilizer Medications in the Treatment of Chronic Neuropathic Pain: a Comprehensive Review
Current Pain and Headache Reports (2019)
