
Abstract
Study design:
Prospective, regional population-based study.
Objectives:
To provide the incidence, aetiology and injury characteristics of traumatic spinal cord injury (TSCI) in the City of Cape Town, South Africa.
Setting:
All government-funded hospitals within the City of Cape Town, South Africa.
Methods:
All survivors of acute TSCI, given that they met the inclusion criteria, were prospectively included for a 1-year period. The International Spinal Cord injury Core Data Set was used and systematically completed by specialist doctors. Further, international standards for neurological classification were adhered to.
Results:
In total, 147 cases of acute TSCI were identified and 145 were included in the study. The male to female ratio was 5.9:1 and the mean age was 33.5 years, ranging from 18 to 93. The crude incidence rate was 75.6 per million (95% CI: 64.3–88.8) with assault as the main cause of injury, accounting for 59.3% of the cases, followed by motor vehicle accidents (26.3%) and falls (11.7%). Most injuries occurred in the cervical spine (53.1%), and American Spinal Injury Association Impairment Scale A severity was most common (39.3%) in the cohort.
Conclusion:
The incidence rate of TSCI in a region of South Africa was high when compared to previously postulated figures for the country. There is a need for primary preventative strategies to target younger men that are exposed to violent activities. A national study is required to learn whether these findings are only locally applicable or generalisable.
Similar content being viewed by others


Introduction
Injury to the spinal cord, due to trauma, could affect persons irrespective of age, gender, socioeconomic background, ethnicity and demographic location.1, 2 As such, many countries have invested in establishing knowledge concerning the epidemiological profile of traumatic spinal cord injuries (TSCI).3, 4, 5 Knowledge pertaining to the epidemiology of health conditions is essential for developing policies and preventative programs. Different causative factors could result in TSCI; therefore, knowledge and understanding of causes are imperative for geographically delineated prevention programs.
The global profile of TSCI had been studied recently. Studies found that incidence rates and injury characteristics across continents differ greatly.1, 2, 6 However, methodological inconsistency is one of the reasons for this perceived disparity. A recent worldwide review7 and another including developing countries only,8 estimated incidence rates of TSCI between 3.6 and 195.4 and 2.1–130.7 per million, respectively. Further, younger males remain at greater risk and the main causes of injury are context dependant.8 Uniform across reports were the limited empirical data available for the Carribean and Latin America, and specifically Africa and Asia.1, 2, 6, 7 The lack of knowledge and prevention could result in a relatively stable incidence and an increased prevalence of TSCI.
In South Africa, two retrospective hospital-based studies have been conducted, two decades ago, investigating injury characteristics of persons with spinal cord injury (SCI),9, 10 with no estimate of the incidence rate. Interestingly, they reported the main cause of injury to be due to gunshot and stab wounds. To date, no SCI register or database is available that prospectively record individuals with an SCI; hence, little is known whether the injury profile has changed or not. The aim of this study was to contribute to the global map of TSCI epidemiology using a prospective, population-based approach to estimate the incidence rate and to determine the main causes and injury characteristics of survivors in the City of Cape Town region, South Africa. Further, this study will assist in creating an evidence-based foundation for primary and secondary prevention of TSCI and its associated consequences.
Materials and methods
Design
All acutely injured survivors of TSCI, fulfilling the inclusion criteria, were prospectively included in a 1-year, open-ended, population-based cohort study. The prospective design was implemented for all citizens with government-funded healthcare insurance, comprising 75% of the total population. The observation period was 1 year, from 15 September 2013 to 14 September 2014.
Setting and implementation of active registration system
The study was conducted in the City of Cape Town region, which is situated in the Western Province of South Africa. The catchment is most diverse with regard to socioeconomic status and ethnicity, and consists of urban and peri-urban areas.
The population, at the end of 2013, was estimated at 3.86 million and is spread across an area of 2445 km2 (see Table 1). The region is most inhabited by Coloured people (mixed race origin), comprising 42.4% of the population, followed by Africans representing 38.6%, Whites contributing 15.7% to the population, and the remaining 1.3% belonging to the Indian/Asian ethnic group.
A specialized acute SCI unit is situated in the City of Cape Town region, serving people in the Western Cape Province of South Africa. In the government-funded healthcare system, the SCI care is provided in a systematic manner with survivors receiving care at Groote Schuur Hospital acute SCI unit and specialized rehabilitation at another facility situated in Cape Town. However, due to limited resources (number of beds/placements) at the acute SCI unit, patients are accepted on a referral basis.
In order to maximise the coverage to all survivors of TSCI, other non-specialized, referring hospitals in the catchment area that were responsible for their management, either for an interim period (until a placement became available at the specialized unit) or for the entire acute management period, were included. Thus, the registration system for TSCI included the screening of cases at the specialized acute SCI unit at Groote Schuur Hospital, the other tertiary hospital (Tygerberg), and referrals that were received from three secondary hospitals. Figure 1 illustrates the active registration system for the screening and inclusion of participants.

Active registration system for TSCI registration in the City of Cape Town, South Africa.
Inclusion criteria
Inclusion criteria for the study were: (1) confirmed acute traumatic spinal cord or cauda equina lesion, (2) age 18 or older at the time of injury, (3) admittance to one of the government hospitals within the catchment area, (4) survival for at least 7 days post trauma and maintaining TSCI as the primary diagnosis, (5) a resident of the country and of the catchment area, and (6) those that provided informed consent.
Data collection and procedure
The instrument for data collection consisted of the International SCI Core Data Set, as recommended by the members of the Executive Committee for the International SCI Data Sets Committees.11 Variables included, date of birth, gender, date of injury, date of acute admission and discharge (duration of hospital stay), aetiology, presence of vertebral fractures and associated injuries, whether spinal surgery was performed, ventilator-dependence at discharge, and place of discharge. Assessment of neurological severity was done according to the International Standards for Neurological Classification of Spinal Cord Injury.12 Two attending specialist doctors completed the International SCI Core Data Set for all admitted patients.
Statistical analyses and ethics
Participants’ characteristics (for example, age, gender, duration of hospital stay, causes of injury and vertebral injuries) and injury characteristics (location of injury and completeness of injury) were analysed descriptively. Continuous variables were expressed as both, mean with standard deviation and median with range. Categorical variables were expressed as number of cases and percentages. For age, two sets of categories were created. For participants’ characteristics and aetiology of injury, 15 year increments were used as recommended.11 Concerning the age-specific incidence rates, 10 year increments were used in order to facilitate comparison between studies that reported the information. Differences between subgroups were analysed using Chi-square and Fischer’s exact test. The incidence rate was calculated for the government-funded sector. The population at risk, for the crude incidence, was calculated using the end of 2013 population figures minus those under 18 years old and those with private medical care. The incidence rates (crude, age specific and gender specific), with 95% confidence intervals, were calculated using the Poisson distribution. Age and gender-adjusted incidence rates were calculated by the method of direct standardisation, using the World Health Organization standard population. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Results
Study population characteristics
Overall, 147 individuals sustained a TSCI during the study period. Of the 145 consented cases, 124 (85.5%) were males, and the male to female ratio was 5.9:1. The mean age at injury was 33.5 (s.d.=±13.8), ranging between 18 and 93 with 54% and 6% of the cohort in the 18–30 and ⩾61 age categories, respectively. Most of the injuries occurred during the summer and winter months with the highest proportion (23.4%) of the injuries occurring on a Saturday and the lowest (5.5%) on a Thursday. In total, 106 (73.1%) sustained a vertebral fracture while 51.7% (of entire cohort) underwent spinal surgery. Associated injuries were present in 84 participants (57.9%). Table 2 summarizes participant characteristics.
Incidence
The annual crude incidence rate of TSCI for this population was 75.6 per million persons (95% CI: 64.3–88.8). After standardisation, the annual incidence was 71.3 per million (95% CI: 53.9–94.3). The gender-specific incidence rates were 130.3 (95% CI: 109.2–155.3) and 21.2 (95%CI: 13.8–32.4) for males and females, respectively. For age and gender-specific rates (Table 3), a significant difference was found for age categories 18–29, 30–39 and 40–49 (P<0.001).
Aetiology
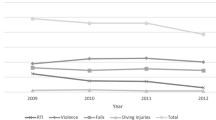
The main cause of injury in this study was assault (59.3%), followed by transportation (26.3%) and falls (11.7%) (Figure 2). Only one sport-related injury was registered and three classified into the so-called ‘other traumatic cause’ (two work-related and one due to self-harm). With reference to the ‘assault’ category, 52% of injuries were caused by gunshots, 33% due to stab wounds, and 15% as a result of interpersonal violence involving blunt trauma. For falls (n=17; n=1 missing), 41% of the injuries were from heights greater than 3 m, 29% occurred on the same level, and 24% from heights between 1 and 3 m. Only two of the 13 falls in the three combined age categories (18–30, 31–45 and 46–60) occurred on the same level, compared to all in the ⩾61 years of age category. Concerning aetiological differences between males and females, the proportion of TSCI caused by assault was significantly higher (P=0.03) in males (63%) than in females (38%). Falls together with assault were the leading causes of TSCI in females. Assault was the leading cause of TSCI in the age categories 18–30 and 31–45, whereas both transportation and falls were leading causes in the 46–60 and ⩾61 age groups.

Aetiology of traumatic spinal cord injury for different age categories.
Location and severity of injury
Spinal injury to the cervical area (C1–8) was most common (53.1%), followed by injuries in the thoracic area (38.6%). Injury to the lumbar and sacral areas was least common (8.3%) (Figure 3). Fifty-seven (39.3%) participants were motor-sensory complete (AIS A) with the highest proportion of those having thoracic spinal injuries (55.4%). Participants with AIS D classifications constituted the second highest proportion, manifesting in 36.5%, and most common in those with cervical spinal injuries (35.1%). Comparing two categories for classification (tetraplegia vs paraplegia) and severity (complete vs incomplete), significantly more persons (50%) with paraplegia had complete injuries compared to those (28.6%) with tetraplegia (P=0.01).

Location and severity of injury.
Discussion
The first prospective, population-based study in the City of Cape Town, South Africa, revealed a high incidence of TSCI that occurred predominantly in males between the ages of 18 and 29 years and chiefly due to interpersonal violence (assault).
The annual crude incidence of TSCI was 75.6 per million for the population under study, which was found to be among the highest in the world and comparable to estimates of 60.6 per million in China13 and 52.5 per million in Canada.14 The global incidence rate was estimated to be 23 cases per million, with the highest in North America (40 per million) and an interval for Africa ranging between 21 and 29 per million.6 The results of this study suggested a much higher incidence of TSCI in South Africa than previously estimated. A recent epidemiological study on TSCI, conducted in Botswana (situated in SubSaharan Africa), reported an incidence of 13 per million population,15 also much lower than reported in this study. Overall, it is difficult to compare the incidence to other countries in Africa due to the lack of information concerning the epidemiology of TSCI.
When comparing age- and gender-specific rates in this study, a significant difference was found between males and females for age categories 18–29, 30–39 and 40–49. The incidence for men in the age groups 18–29 and 30–39 were ~200 and 125 per million, respectively. Very few studies report age and gender-specific incidence rates, information that is essential for the planning of relevant preventive strategies and for resource allocation. One recent study conducted in Estonia found similar peaks in males for the 20–29 (133.9 per million) and 30–39 (95.0 per million) age categories,16 and an older Canadian study reported an incidence rate of 138.0 per million for men between 20 and 29 years of age.14 The need exists to identify the factors that place this particular group at greater risk for TSCI compared with other age categories. In our study, the mean age at injury was 33.5 (median 29.0 years), lower than the global estimate, but comparable to studies conducted in the developing world.8 Interpreting our results requires the consideration that this study included individuals from 18 years of age only. Therefore, we postulate that the mean and median age of onset would have been lower if all ages were studied.
Almost 60% of the TSCIs were caused by assault. In this study, the assault category comprised gunshots, stabs and blunt trauma. It was the leading cause for both genders, suggesting similar preventative needs. More than half of the assault cases were firearm related. Comparing the proportion of gunshots (31%) and stabs (20%) in this study to a study conducted two decades ago in the northern part of South Africa, it is evident that gunshot injuries (36%) and stab wounds (20%) remained relatively stable as the main causes of injury.9, 10 It is inconclusive whether preventative strategies were ineffective or limited since earlier data from each specific region are lacking. However, it is reasonable to highlight the need for preventative initiatives when recognising the devastating consequences of firearm use.
The proportion of gunshot and stab wounds appears to be a unique problem in South Africa compared to other African countries.15, 17, 18 Interpersonal violence cause an unprecedented burden of morbidity and mortality,19 not only for SCI, but also for other health events. A national study in South Africa reported that violence-induced injuries are the second leading cause of death in the country. Although we could not provide evidence on the associated fatalities caused by assault, due to the scope of the study, our findings clearly showed that the main cause of TSCI morbidity was interpersonal violence.19 A study focusing on mortality is warranted to determine the burden of TSCI due to preventable causes such as interpersonal violence.
The majority of the study population was tetraplegic with incomplete lesions, whereas those with paraplegia most commonly presented with complete injuries (AIS A). Interestingly, at discharge from acute hospitalisation none of the participants was ventilator-dependant. This is inconsistent with a recent report that included this key outcome.20 We have initiated a currently ongoing study that investigates factors influencing mortality (during acute hospitalisation and 1-year follow-up), with a secondary aim to study the prognosis of those who were mechanically ventilated for a prolonged duration since admission.
The strength of this study was the prospective, population-based design, which was the first to be conducted in a region of South Africa. Furthermore, the International SCI Core Data Set was used, as recommended for the standardized reporting of core data. Previously mentioned as ideal practise for TSCI registration, the core data set was completed by specialist doctors that could limit false-negative results.20
The study presented with limitations that need consideration for future research. First, only those 18 years and above were included and those in the government-funded healthcare system; thus leaving a knowledge gap concerning paediatric TSCI and those with private healthcare insurance. Therefore, the incident cases in this study are likely an underestimation of the burden of TSCI morbidity in this region of South Africa. However, the incidence rate could be an over- or underestimation. Second, the study setting was limited to one large region in the Western Province of South Africa; therefore, the results cannot automatically be generalised to other provinces in the country. Given these limitations, follow-up studies should include all ages, survivors in both healthcare systems, settings in other provinces, and the International SCI Core Data Set along with the International Classification of External Causes of Injury should be implemented in all hospitals nationwide involved in SCI care in order to fully represent the nation of South Africa.
In conclusion, the first prospective, population-based study found that the incidence rate of newly injured survivors was high (75 per million), peaking in males between 18 and 29 years of age. TSCI due to interpersonal violence was alarmingly high, among the highest in the world. The results provided some evidence to suggest a need for preventative programs.
Data archiving
There were no data to deposit.
References
Vasiliadis AV . Epidemiology map of traumatic spinal cord injuries: a global overview. Int J Caring Sci 2012; 5: 335–347.
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Divanoglou A, Levi R . Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord 2009; 47: 796–801.
van Asbeck FW, Post MW, Pangalila RF . An epidemiological description of spinal cord injuries in The Netherlands in 1994. Spinal Cord 2000; 38: 420–424.
Albert T, Ravaud JF, Tetrafigap group. Rehabilitation of spinal cord injury in France: a nationwide multicentre of incidence and regional disparities. Spinal Cord 2005; 43: 357–365.
Lee BB, Cripps RA, Fitzharris M, Wing PC . The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord 2014; 52: 110–116.
Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V . Incidence of traumatic spinal cord injury worldwide: a systematic review. Eur Spine J, (e-pub ahead of print 21 june 2014; doi:10.1007/s00586-014-3424-6).
Rahimi-Movaghar V, Sayyah MK, Akbari H, Khorramirouz R, Rasouli MR, Moradi-Lakeh M et al. Epidemiology of traumatic spinal cord injury in developing countries: a systematic review. Neuroepidemiology 2013; 41: 65–85.
Hart C, Williams E . Epidemiology of spinal cord injuries: a reflection of changes in South Africa society. Paraplegia 1994; 32: 709–714.
Velmahos G, Degiannis E, Hart C, Souter I, Saadia R . Changing profiles in spinal cord injuries and risk factors influencing recovery after penetrating injuries. J Trauma Injury Infect Crit Care 1995; 38: 334–337.
DeVivo MJ, Biering-Sorensen F, Charlifue S, Noonan V, Post M, Stripling T et al. International spinal cord injury core data set. Spinal Cord 2006; 44: 535–540.
Waring WP III, Biering-Sorensen F, Burns S, Donovan W, Graves D, Jha A et al. 2009. Review and revisions of the international standards for the neurological classification of spinal cord injury. J Spinal Cord Med 2010; 33: 346–352.
Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B et al. The epidemiological survey of acute traumatic spinal cord injuries (ATSCI) of 2002 in Beijing municipality. Spinal Cord 2011; 49: 777–782.
Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW et al. The epidemiology of traumatic spinal cord injury in Alberta, Canada. Can J Neurol Sci 2003; 30: 113–121.
Löfvenmark I, Norrbrink C, Nilsson-Wikmar L, Hultling C, Chakandinakira S, Hasselberg M . Traumatic spinal cord injury in Botswana; characteristics, aetiology and mortality. Spinal Cord 2015; 53: 150–154.
Sabre L, Pedai G, Rekand T, Asser T, Linnamagi U, Korv J . High incidence of traumatic spinal cord injury in Estonia. Spinal Cord 2012; 50: 755–759.
Draulans N, Kiekens C, Roels E, Peers K . Etiology of spinal cord injuries in Sub-Saharan Africa. Spinal Cord 2011; 49: 1148–1154.
Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO . Profile of spinal injuries in Lagos, Nigeria. Spinal Cord 2009; 47: 134–137.
Seedat M, Van Niekerk A, Jewkes R, Suffla S, Ratele K . Violence and injuries in South Africa: prioritising an agenda for prevention. Lancet 2009; 374: 1011–1022.
Koskinen EA, Alen M, Väärälä EM, Rellman J, Kallinen M, Vainionpää A . Centralised spinal cord injury care in Finland: unveiling the hidden incidence of traumatic injuries. Spinal Cord 2014; 52: 779–784.
Acknowledgements
This work was supported by the Thuthuka Grant from the National Research Foundation in South Africa. The authors would like to thank Dr Stander and Dr Sothman for evaluating the participants in the study and Professor Karin Harms-Ringdahl for valuable advice. We would also like to thank Professor Åke Seiger for reviewing the manuscript and his support throughout the project.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Joseph, C., Delcarme, A., Vlok, I. et al. Incidence and aetiology of traumatic spinal cord injury in Cape Town, South Africa: a prospective, population-based study. Spinal Cord 53, 692–696 (2015). https://doi.org/10.1038/sc.2015.51
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.51
This article is cited by
-
The interrelationship between pain, life satisfaction and mental health in adults with traumatic spinal cord injury, in the context of a developing country
Spinal Cord Series and Cases (2024)
-
The prevalence and profile of spinal cord injury in public healthcare rehabilitation units in Gauteng, South Africa
Spinal Cord Series and Cases (2023)
-
Mortality and secondary complications four years after traumatic spinal cord injury in Cape Town, South Africa
Spinal Cord Series and Cases (2020)
-
Wirbelsäulenverletzungen im Kindesalter – Ergebnisse einer nationalen Multizenterstudie mit 367 Patienten
Der Unfallchirurg (2020)
-
Prevention care for secondary health conditions among people living with spinal cord injuries: research protocol
BMC Research Notes (2019)
