
Abstract
Study design:
Multi-center, cross-sectional study.
Objectives:
Our aim was to evaluate the treatment methods and follow-up of neurogenic bladder in patients with traumatic spinal cord injury retrospectively using a questionnaire.
Setting:
Turkey.
Methods:
Three hundred and thirty-seven patients who had spinal cord injury for at least 2 years were enrolled from six centers in the neurogenic bladder study group. They were asked to fill-out a questionnaire about treatments they received and techniques they used for bladder management.
Results:
The study included 246 male and 91 female patients with a mean age of 42±14 years. Intermittent catheterization (IC) was performed in 77.9% of the patients, 3.8% had indwelling catheters, 13.8% had normal spontaneous micturition, 2.6% performed voiding maneuvers, 1.3% used diapers and 0.6% used condom catheters. No gender difference was found regarding the techniques used in bladder rehabilitation (P>0.05). Overall, 63.2% of patients used anticholinergic drugs; anticholinergic drug use was similar between genders (P>0.05). The most common anticholinergic drug used was oxybutynin (40.3%), followed by trospium (32.6%), tolterodine (19.3%) darifenacin (3.3%), propiverine (3.3%) and solifenacin (1.1%). The specialties of the physicians who first prescribed the anticholinergic drug were physiatrists (76.2%), urologists (22.1%) and neurologists (1.7%). Only four patients had previously received injections of botulinum-toxin-A into the detrusor muscle and three of them stated that their symptoms showed improvement. Most of the patients (77%) had regular follow-up examinations, including urine cultures, urinary system ultrasound and urodynamic tests, when necessary; the reasons for not having regular control visits were living distant from hospital (15.3%) and monetary problems (7.7%). Of the patients, 42.7% did not experience urinary tract infections (UTI), 36.4% had bacteriuria but no UTI episodes with fever, 15.9% had 1-2 clinical UTI episodes per year and 5% had ⩾3 clinical UTIs. The clinical characteristics of patients with and without UTI (at least one symptomatic UTI during 1 year) were similar (P>0.05). The frequency of symptomatic UTI was similar in patients using different bladder management techniques (P>0.05).
Conclusion:
The most frequently used technique for bladder rehabilitation in patients with SCI was IC (77.9%). In all, 63.2% of patients used anticholinergic drugs, oxybutynin being the most commonly used drug. Also, 77% of patients had regular control visits for neurogenic bladder; 42.7% did not experience any UTIs.
Similar content being viewed by others


Introduction
More than 10 000 people are diagnosed with spinal cord injury (SCI) in the United States each year. SCI is associated with a high socioeconomic burden on patients and their families, and has a high complication rate.1 One of the most important consequences of SCI is changes in lower urinary tract function. The primary aims for treatment of neurogenic lower urinary tract dysfunction and their priorities are: (1) protection of the upper urinary tract, (2) improvement of urinary continence, (3) restoration of (parts of) the lower urinary tract function, and (4) improvement of the patient’s quality of life.2 Although mortality related to urological complications has been reduced during the past decades, urinary tract problems continue to be a prominent cause of morbidity after SCI.2, 3, 4 Urinary tract infection (UTI) is the most common complication in patients with SCI.5, 6 Problems related to UTIs are the most frequent reason for hospital readmissions, and symptoms such as autonomic dysreflexia and incontinence can cause serious physical disturbances or social inconvenience in the lives of those with SCI.7 In order to reduce morbidity and to prevent urological complications, regular follow-up visits to a spinal cord rehabilitation clinic are required.
The primary aim of the current study was to evaluate the methods of bladder management and the follow-up of traumatic SCI patients with neurogenic bladder retrospectively using a questionnaire. The secondary aim was to assess the frequency of self-reported UTI, anticholinergic drug use and injections of botulinum-toxin-A into the detrusor muscle for bladder problems.
Materials and methods
A total of 337 patients who had SCI for at least 2 years were enrolled in this study of Turkish neurogenic bladder research group. The study was carried out in six rehabilitation clinics in four different cities of Turkey between January and October 2012. The patients were asked to fill out a questionnaire about treatments they received and techniques they used for bladder rehabilitation. The patients had help of their physicians during filling the questionnaire.
Approval was obtained from the ethics committee for the study. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Demographic and clinical parameters, including age, gender, marital status, occupation, employment status, accompanying family members, and the etiology, level, severity and duration of SCI were recorded. The severity of SCI was classified into five categories according to the American Spinal Injury Association Impairment Scale (AIS): A=complete lesion, no sensory or motor function is preserved in the lowest sacral segments; B=sensory incomplete (including segments S4–S5), but no motor function below the neurological level; C=sensory and motor incomplete but more than half of the 10 pairs of key muscles have a muscle grade <3 on a scale of 0–5; D=sensory and motor incomplete, at least half of the key muscles have a muscle grade ⩾3; and E=sensory and motor function normal.8
The urological questions dealt with methods of bladder management, regular follow-up visits, UTI and pharmacological treatment (Table 1). Patients were evaluated in six groups according to the bladder management method used: (1) normal spontaneous micturition (NSM), (2) micturition with assisted maneuvers (such as Crede, Valsalva and tapping) (MAM), (3) aseptic intermittent catheterization (IC), (4) indwelling catheterization (IDC), (5) condom catheterization (CC), and (6) diaper use. Regular follow-up was described as control visits according to the physician’s recommendations (it may be at every 6 months, yearly or biyearly according to the patients’ conditions). The questions about pharmacological treatment in the questionnaire identified the anticholinergic drug used at the time of the questionnaire was applied.
Clinical and demographic data of the patients were compared according to the gender of the patients and according to the presence of UTI (at least one symptomatic UTI during 1 year).
Statistical analysis
The PASW (Predictive Analysis Software) Statistics 19.0 (Statistical Package for Social Sciences Inc., Chicago, IL, USA) was used for statistical analysis. Descriptive statistics were used to describe demographic characteristics. For continuous variables, the significance of the differences was analyzed using the Student’s t-test, while categorical variables were analyzed using a chi-square test. The level of significance was set at P<0.05.
Results
The number of eligible patients was 337, and 246 (73%) of them were male and 91 were (27%) female. The majority of the patients were those who were admitted to outpatient clinics for neuro-urological control visit. The remaining group consisted of the patients who were hospitalized for a short period of time for neuro-urological re-assessment and further rehabilitation requirements. The median age was 41 (min: 18, max: 68) years, and the median time since the injury was 48 (min: 24, max: 324) months. Of these patients, two refused to have AIS examination due to personal reasons and one of them could not be evaluated for AIS. Owing to this reason, data concerning severity and level of the lesion were available for 334 subjects. In total, 161 (48%) had a complete lesion and 173 (52%) an incomplete lesion. A total of 57 (17%) subjects had tetraplegia and 277 (83%) paraplegia. The main demographic and clinical data of the patients with SCI are shown in Tables 2 and 3, respectively.
IC was performed in 77.9% of the patients, 13.8% had NSM, 3.8% had IDC, 2.6% performed MAM, 1.3% used diapers and 0.6% used CC (Table 3). All the patients in the IDC group were using urethral catheters. There was no patients with suprapubic catheter. The numbers of female and male subjects in the bladder management groups are shown in Table 4.
Information about medication was available only in 288 subjects. Of these, 63.2% (182/288) of the patients used anticholinergic drugs. The most commonly used anticholinergic drug was oxybutynin (40.3%), followed by trospium (32.6%), tolterodine (19.3%), darifenacin (3.3%), propiverine (3.3%) and solifenacin (1.1%). There was no patients who used a combination of anticholinergics. The specialties of the physicians who first prescribed the drugs were physiatrists (76.2%), urologists (22.1%) and neurologists (1.7%). Only four patients had previously received injections of botulinum-toxin-A into the detrusor muscle and three of them benefited from this treatment (Table 3).
Overall, 77% of the patients stated that they had regular follow-up controls with urine cultures, urinary system ultrasound and urodynamic tests, when necessary; the reasons for not having regular controls were living distant from the hospital (15.3%) and monetary problems (7.7%) (Table 3). In all, 42.7% of the patients had not experienced UTI, 36.4% had asymptomatic bacteriuria but no UTI episodes with symptoms, 15.9% had 1–2 clinical UTI episodes per year and 5% had ⩾3 clinical UTIs (Table 3).
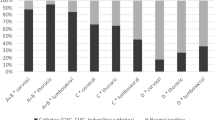
Table 4 shows the comparison of the level and severity of the spinal cord lesion, ambulation status, bladder rehabilitation techniques, anticholinergic drug use, UTI and regular control visits in patients with SCI according to gender. The demographic and clinical data of the female and male patients were similar (P>0.05).
Table 5 shows the comparison of the level and severity of the spinal cord lesion, gender, ambulation status, methods of bladder management, anticholinergic drug use and regular control visits in patients with SCI according to the presence of symptomatic UTI (at least one symptomatic UTI during 1 year). Although it was observed that symptomatic UTI rate was higher among patients with complete injuries and among patients using IDC and MAM, there was no significant difference between the patients with and without UTI (P>0.05). The frequency of symptomatic UTI was similar in the bladder management groups (P>0.05).
Discussion
Today, the average lifespan of SCI patients is longer due to recent improvements in medical care. For this reason, treatment and healing of problems causing morbidity gains much more importance. Among these problems are the urological complications. Therefore, the management of neurogenic bladder dysfunction is a crucial component of a rehabilitation program for SCI, because it affects the morbidity of patients.3, 4 The objective of this study was to evaluate the treatment and follow-up of neurogenic bladder in patients with traumatic SCI retrospectively using a questionnaire.
Normal voluntary voiding is usually impossible after SCI. In the Stockholm SCI Study, 34% of the subjects were classified in the normal micturition group, but at least some of them had functional impairment or used external compression over lower abdomen.9 In another study performed by Dahlberg et al.,10 the subjects who reported to have control over their voiding were divided into two groups: those who had no signs of neurogenic bladder (normal voiding group, 11% of the study group), and those who reported incontinence or those with assisted voiding (controlled voiding group, 12% of the study group). Of the patients in our study, 13.8% of them had normal micturition.
Clean intermittent catheterization (CIC) has helped to improve our knowledge of the bladder and reduce the incidence of urinary complications in patients with SCI.2 Many studies have reported bladder management methods with the use of CIC ranging from 16% to 96%.11, 12 CIC is considered the ideal management or gold standard for neurogenic bladder if the patient is willing, physically and mentally able to perform the task or has caregivers who are able to assist.13, 14 It is usually the primary recommendation for long-term bladder management.15 In accordance with these studies, our results revealed that the most frequently used technique for bladder rehabilitation in patients with SCI is CIC (77.9%).
For practical reasons, reflex voiding and crede or valsalva maneuvers are still commonly in use, often combined with condom drainage in men. In addition, IDC (urethral or suprapubic) remain in common use. Published guidelines are based on reviews of current literature showing that there are significantly more serious complications associated with IDC compared with CIC.2 CIC avoids the need for a permanent foreign body within the bladder and is preferred over an IDC when addressing hygiene, sexuality, body image and preservation/improvement in renal function. However, little is known about what the actual bladder management for the majority of spinal cord injured patients is in everyday practice. It was noted that CIC does not find acceptance initially with the patients and their caregivers. In a recent large study, 24.762 patients with SCI were followed between 1972 and 2005; the use of CIC increased from 12.6% to 49.6%. On the other hand, IDC use decreased from 33.1% in 1972 to 23.1% in 2005. The biggest change was in the use of condom catheterization, which decreased from 34.6% in 1972 to 1.5% in 2005.3 In our study, CC and IDC usage among SCI patients were quite low (0.6% and 3.8% respectively) at a mean of 66 months and a minimum of 24 months follow-up. Our follow-up period was short, 66 months as compared with theirs of 30 years. In the large-scale study mentioned above, it was also reported that female patients had a higher risk for using IDC at discharge from rehabilitation and follow-up.3 Similarly, another study indicated that IDC usage rate was higher in female patients with impaired hand functions.16 Unlike these studies, we demonstrated that bladder management was not different in male and female patients. Lower rate of IDC usage and relatively small number of participants according to the other related studies and short follow-up could be the reasons for this finding.
Absence of other bladder management methods such as sacral neuromodulation, sacral anterior root stimulation, bladder augmentation and conduit in our study group could be due to relatively small number of patients and short-term follow-up.
Satisfactory outcomes, however, have been also reported with conservative methods, which can be combined with oral (anticholinergic) and intravesical medication (that is, botulinum-toxin-A) to improve bladder function.13 Anticholinergic drugs are the first-line choice for treating neurogenic lower urinary tract dysfunction. They provide an established approach to managing neurogenic detrusor overactivity. Anticholinergic drugs are used to stabilise the detrusor muscle, which reduces its overactivity and makes it moderately refractory to parasympathetic stimulation. This results in improved bladder compliance and reduced symptoms of overactive bladder, which in turn helps to prevent renal and bladder damage and potentially improve long-term outcomes.2 In a meta-analysis, including 69 trials with 26 229 patients, similar overall adverse event profiles were found for darifenacin, fesoterodine, transdermal oxybutynin, propiverine, solifenacin, tolterodine and trospium chloride, whereas oral oxybutynin dosages of ⩾10 mg day−1 have less favorable adverse event profiles.17 In our study, 63.2% of the patients used anticholinergic drugs. Of these, the most commonly used drug was oxybutynin, followed by trospium and tolterodine. In the study by Khanna et al.,18 oxybutynin alone was used in 52% of the patients and was combined with tolterodine in 28% of the patients and in combination with solifenacin in six patients. In the study by Dahlberg et al.,10 it was reported that only six patients had been on anticholinergic medication (oxybutynin) and three patients had used alpha-blockers (tamsulosin) out of the 119 SCI patients who were followed up at least a year. In the studies of Sekar et al.14 and Nosseir et al.,19 the rate of patients using anticholinergic medication was 31% and 58%, respectively. Combined treatment with anticholinergics and CIC as part of the conservative treatment still remains the mainstay of urological management of most SCI patients with detrusor overactivity and detrusor-sphincter dyssinergia. Hansen et al.,12 conducted a study on 236 SCI patients (193 men, 43 women) between 10 and 45 years (mean 24.1 years), including 126 paraplegic and 110 tetraplegic patients. That study used a follow-up questionnaire and a retrospective review of the notes; they determined that 56% of the patients utilized CIC in bladder emptying, and only 19% used medications. Interestingly, about 40% of those taking medication were on anticholinergics. Intradetrusor injection with botulinum-toxin-A has a role in treating drug-resistant neurogenic detrusor overactivity. Its efficacy has been demonstrated by randomized placebo-controlled trials in patients with SCI.20, 21 Because of its short duration of action, it requires repeated invasive procedures. The optimal number and long-term effects of botulinum-toxin-A injections providing efficacy is not clearly known. Intermittent injections of botulinum-toxin-A will tentatively bridge the gap between oral treatment and invasive surgical treatment. Most patients maintained benefit for 10–12 months, and 20% benefitted for >12 months.22 In our study, botulinum-toxin-A was used in four patients and three of them expressed improvement. We feel that the low frequency of botulinum-toxin-A injections to detrusor observed in our study is due to the policies of health insurance agencies. Botulinum-toxin-A injections to detrusor are not paid by health insurance agencies in Turkey.
It is noteworthy that UTI is the most commonly reported complication of SCI in all series.5, 6 No uniform definition of UTI was used in articles.6, 14, 15, 16, 18, 23 In a long-term follow-up (ranged between 8 and 21 years, with a mean of 17.7 years) study evaluating the outcomes of bladder management in 119 SCI patients, 61% of the patients were reported to have complications. UTI stands out as the most common (80.1%) complication either alone (50%) or in combination with other complications.16 In the study of Maynard and Glass,23 the records of SCI patients were retrospectively evaluated at a mean of 5 years, and symptomatic UTI rate was reported as 30% in those using CIC as the bladder management method, whereas Khanna et al.18 determined the rate as 58% at 3 years follow-up. Biering-Sorensen et al.13 reported that 81% of the patients had been treated for at least one UTI, 22% had 2–3 UTI per year and 12% of the patients had ⩾4 UTI per year in 75 patients at 5 years. However, in our study, 15.9% had 1–2 symptomatic UTI episodes per year and 5% had at least 3 UTIs per year. Weld et al.11 reported that 93% of their patients developed lower UTI symptoms, whereas the incidence of UTI in our series was 20.1%. Our results concerning UTI have to be interpreted with caution as the information was collected retrospectively. However, they did not define the presentation of UTI, and hence it is difficult to accurately compare the incidence of UTI between these four series.
In our study, in accordance with previous studies, the incidence of UTI does not seem to be related to gender.14, 16 In addition, demographic and clinical characteristics of the patients, including age, level and severity of the spinal cord lesion, ambulation status, bladder management methods, anticholinergic drug use and the regularity of visits to the rehabilitation clinic, were similar in SCI patients with and without UTI (at least one symptomatic UTI during 1 year). The method of urinary drainage is thought to be a very important risk factor for UTI in SCI population, and IDC with urethral or suprapubic catheters and urinary diversion are the methods most likely to lead to persistent bacteriuria. The IDC is a persistent foreign body and facilitates bacterial growth and migration of uropathogens upwards through the mucosal sheath surrounding the catheter. Although the difference was not statistically significant, the proportion of patients with NSM was higher among patients without UTI compared with those with UTI. This occasion was also mentioned in the work by El-Masri et al.16 On the contrary, in the group with UTI, the proportion of patients with IDC and MAM was higher than that of patients without UTI, although not at a statistically significant level. This may suggest that NSM carries less risk than IDC and MAM. Also in the study by Dahlberg et al.,10 the subjects in the suprapubic-tapping group had less UTI than those who used CIC. In our study, the insignificant difference in UTI rates among patients using different bladder management methods may be attributed to the small numbers of patients in the bladder management subgroups, except in the IC group.
There are some limitations of our study that must be considered. The study population was enrolled from six centers in four different cities. Although these six centers are the major clinics those serve SCI population in Turkey, the findings may not reflect the care that is given in the other clinics throughout Turkey. There may be some accuracy problem in asymptomatic bacteriuria and UTI frequencies because of the subjectivity of the reports of the patients. The relatively small number of the patients in subgroups, lack of data about long-term follow-up, lack of some detailed data relating to bladder management and UTIs, retrospective analysis of UTI, using a questionnaire which was not self-administrated and not validated and also not including information about the treatment results are other limitations of our study. The questionnaire should better include more comprehensive data, but because of the time limitation, this relatively short and practical questionnaire was used.
Conclusions
According to the results of this study that were derived from the data collected retrospectively by the supervised questionnaire, the most frequently used technique for neurogenic bladder management in patients with SCI is IC, and 63% of the patients with SCI use anticholinergic drugs, oxybutynin being the most common medication used. In all, 77% of the patients had regular controls for neurogenic bladder, and 43% did not experience any UTIs.
Data Archiving
There were no data to deposit.
References
Horstmann M, Schaefer T, Aguilar Y, Stenzl A, Sievert KD . Neurogenic bladder treatment by doubling the recommended antimuscarinic dosage. Neurourol Urodyn 2006; 25: 441–445.
Pannek J, Stöhrer M, Blok B, Castro-Diaz D, Del Popolo G, Kramer G et al. Guidelines on Neurogenic Lower Urinary Tract Dysfunction. European Association of Urology (EAU): Arnhem, The Netherlands. 2011.
Cameron AP, Wallner LP, Tate DG, Sarma AV, Rodriguez GM, Clemens JQ . Bladder management after spinal cord injury in the United States 1972 to 2005. J Urol 2010; 184: 213–217.
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and cause of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Ruutu M, Lehtonen T . Urinary tract complications in spinal cord injured patients. Ann Chir Gynaecol 1984; 73: 325.
Penders J, Huylenbroeck AA, Everaert K, Van Laere M, Verschraegen GL . Urinary infections in patients with spinal cord injury. Spinal Cord 2003; 41: 549–552.
Savic G, Short DJ, Weizenkamp D, Charlifue S, Gardner BP . Hospital readmissions in people with chronic spinal cord injury. Spinal Cord 2000; 38: 371–377.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A et al. International standards for neurological classification of spinal cord injury (Revised 2011). J Spinal Cord Med 2011; 34: 535–546.
Levi R, Hultling C, Nash MS, Seiger A . The Stockholm spinal cord injury study: 1. Medical problems in a regional SCI population. Paraplegia 1995; 33: 308–315.
Dahlberg A, Perttila I, Wuokko E, Ala-Opas M . Bladder management in persons with spinal cord lesion. Spinal Cord 2004; 42: 694–698.
Weld KJ, Graney MJ, Dmochowski RR . Differences in bladder compliance with time and associations of bladder management with compliance in spinal cord injured patients. J Urol 2000; 163: 1228.
Hansen RB, Biering-Sorensen F, Kristensen JK . Urinary incontinence in spinal cord injured individuals 10–45 years after injury. Spinal Cord 2010; 48: 27–33.
Biering-Sorensen F, Nielans HM, Dorflinger T, Sorensen B . Urological situation five years after spinal cord injury. Scand J Urol Nephrol 1999; 33: 157–161.
Sekar P, Wallace DD, Waites KB, DeVivo MJ, Lloyd LK, Stover SL et al. Comparison of long-term renal function after spinal cord injury using different urinary management methods. Arch Phys Med Rehabil 1997; 78: 992–997.
Bakke A, Digranes A, Hoisaeter PA . Physical predictors of infection in patients with clean intermittent catheterization: a prospective 7-year study. Br J Urol 1997; 79: 85–90.
El-Masri WS, Chong T, Kyriakider AE, Wang D . Long-term follow-up study of outcomes of bladder management in spinal cord injury patients under the care of The Midlands Centre for Spinal Injuries in Oswestry. Spinal Cord 2012; 50: 14–21.
Kessler TM, Bachmann LM, Minder C, Löhrer D, Umbehr M, Sc hünemann HJ et al. Adverse event assessment of antimuscarinics for treating overactive bladder: a network meta-analytic approach. PLoS One 2011; 6: e16718.
Khanna CR, Sandhu AS, Doddamani CD . Urodynamic management of neurogenic bladder in spinalcord injury. Med J Armed Forces India 2009; 65: 300–304.
Nosseir M, Hinkel A, Pannek J . Clinical usefulness of urodynamic assessment for maintenance of bladder function in patients with spinal cord injury. Neurourol Urodyn 2007; 26: 228–233.
Ehren I, Volz D, Farrelly E, Berglund L, Brundin L, Hultling C et al. Efficacy and impact of botulinum toxin A on quality of life in patients with neurogenic detrusor overactivity: a randomised, placebo-controlled, double-blind study. Scand J Urol Nephrol 2007; 41: 335–340.
Schurch B, de Seze M, Denys P, Chartier-Kastler E, Haab F, Everaert K et al. Botulinum toxin type a is a safe and effective treatment for neurogenic urinary incontinence: results of a single treatment, randomized, placebo controlled 6-month study. J Urol 2005; 174: 196–200 This article provides evidence for the efficacy of botulinum toxin A in treating NDO from a phase 2 placebo-controlled randomized trial.
Del Popolo G, Filocamo MT, Li Marzi V, Macchiarella A, Cecconi F, Lombardi G et al. Neurogenic detrusor overactivity treated with english botulinum toxin a: 8-year experience of one single centre. Eur Urol 2008; 53: 1013–1019.
Maynard FM, Glass J . Management of the neuropathic bladder by clean intermittent catheterisation: 5 year outcomes. Paraplegia 1987; 25: 106–110.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Neurogenic Bladder Turkish Research Group., Yıldız, N., Akkoç, Y. et al. Neurogenic bladder in patients with traumatic spinal cord injury: treatment and follow-up. Spinal Cord 52, 462–467 (2014). https://doi.org/10.1038/sc.2014.41
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.41
This article is cited by
-
Sex differences in urological management during spinal cord injury rehabilitation: results from a prospective multicenter longitudinal cohort study
Spinal Cord (2023)
-
Kurzfassung der S2k-Leitlinie medikamentöse Therapie der neurogenen Dysfunktion des unteren Harntraktes (NLUTD)
Die Urologie (2023)
-
Impact of Neurogenic Lower Urinary Tract Dysfunction on Bowel Symptoms
Current Bladder Dysfunction Reports (2023)
-
Bladder management in individuals with spinal cord injury or disease during and after primary rehabilitation: a retrospective cohort study
World Journal of Urology (2022)
-
Bladder management in individuals with chronic neurogenic lower urinary tract dysfunction
Spinal Cord (2016)
