
Abstract
Study design:
Descriptive comparison analysis.
Objective:
To evaluate whether five training cases of International Spinal Cord Injury Core Data Set (ISCICDS) are appropriate for testing the facts within the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) and could thus be used for testing its training effectiveness.
Methods:
The authors reviewed the five training cases from the ISCICDS and determined the sensory level (SL), motor level (ML) and American Spinal Injury Association Impairment Scale (AIS) for the training cases. The key points from the training cases were compared with our interpretation of the key aspects of the ISNCSCI.
Results:
For determining SL, three principles of ML, sacral sparing, complete injury, classification of AIS A, B, C and D, determining motor incomplete status through sparing of motor function more than three levels below the ML, there are corresponding case scenarios in ISCICDS. However, no case scenario shows classification of AIS E and the use of voluntary anal sphincter contraction for determination of motor incomplete status. Neurological level of injury could be deduced from the SL and ML. Finally, none of the cases include information about zone of partial preservation, sensory score or motor score.
Conclusion:
Majority of the facts related to SL, ML and AIS are included in the five training cases of ISCICDS. Thus, using these training cases, it is feasible to test the above facts within the ISNCSCI. It is suggested that the missing fact should be included in an update of the training cases.
Similar content being viewed by others


Introduction
The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) is widely used in clinical and research settings when assessing and treating individuals who suffer from spinal cord injury (SCI). With the efforts of continued revisions in the past few decades, the ISNCSCI is progressively refined and optimized, with the latest seventh edition being published in 2011.1 The easy-to-use booklet of the seventh edition2 is available from the American Spinal Injury Association. Accurate scoring and scaling of the ISNCSCI is of utmost importance, hence it was suggested that proper training should be given before the use of the ISNCSCI in clinical practice. Some studies3, 4, 5 have demonstrated that case presentation was an effective method for training of the ISNCSCI. However, different cases are used for training and the effect among the studies can hardly be compared. Thus, a series of standardized training cases including as many items as possible from ISNCSCI is optimal for the training. To our knowledge, no internationally published training cases are available; especially, there is a lack of officially endorsed translation of training cases into other languages, including Chinese.
The International Spinal Cord Injury Core Data Set (ISCICDS) was developed in 20066 to standardize the collection and reporting of minimal information worthwhile to know about any SCI population. The minimal information necessary to document neurological status in ISCICDS is the sensory (SL) and motor level (ML) on each side of the body and the American Spinal Injury Association Impairment Scale (AIS). These three items are components of the ISNCSCI. The official document of ISCICDS is presented at the International Spinal Cord Society (ISCoS) website.7 In addition to the data collection form and syllabus, the document also includes five training cases.7 Each of the case description includes the neurological status both at admission and at discharge. Thus there are 10 scenarios representing the determination of SL, ML and AIS. These training cases can be downloaded free of charge from the website; hence, they could be considered as standardized cases for training the neurological classification if they contain the majority of facts within ISNCSCI. Furthermore, the ISCICDS including the training cases is officially translated to Chinese, according to the recommendations by the Executive Committee for the International SCI Standards and Data Sets,8 and the translation is likewise available from ISCoS website.9
In this study, the clinical reasoning process used in determining SL, ML and AIS in the five training cases of ISCICDS is analyzed and then compared with the facts within the ISNCSCI in order to evaluate whether these cases are appropriate for testing the fact of ISNCSCI as well as provide suggestions for the refinement of these training cases.
Materials and methods
Initially, the first and second authors reviewed the five training cases from the official translated Chinese version of ISCICDS9 and answered the SL, ML and AIS both at admission and at discharge of these cases. Then the authors compared the answers with the correct results that are also posted with the document.9 In addition, the authors perused the Chinese translation of the ISNCSCI booklet and listed all the facts within the booklet.10 Next, the clinical reasoning process for determining SL, ML and AIS were discussed and analyzed according to the items in the ISNCSCI. Last, the clinical reasoning process used in the five training cases were matched with the items from the ISNCSCI.
Training cases of ISCICDS
The five training cases involve all 10 neurological statuses, that is, at admission and discharge after SCI.7, 9 Training case 1 illustrates an injury of C4 AIS A at admission and C5 AIS A at discharge, whereas training case 2 is an injury of C3 AIS A at admission and C5 AIS A at discharge. Training case 3 represents an injury of C7 AIS B at admission and C8 AIS B at discharge, whereas case 4 is an injury of C6 AIS C at admission and C7 AIS D at discharge. Training case 5 shows a neurological level of injury (NLI) and AIS of T11 AIS A at admission and L2 AIS A at discharge.
Booklet of ISNCSCI
The booklet describes the seventh edition of the ISNCSCI that was published in 2011.2, 10 The concepts related to the sensory and motor scores/levels, and AIS were reviewed in order to provide all potential facts for comparison with those retrieved from the training cases.
Comparison analyses
All potential items from the ISNCSCI are listed. If the fact was reflected in the training case, the corresponding case number and the setting, admission or discharge was noted. If the fact was not shown in the training case, not available was mentioned accordingly.
Results
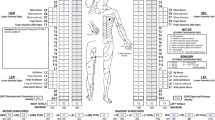
From our interpretation of the key aspects of the ISNCSCI, there could be totally nine items retrieved for description of the neurological status after SCI. The detailed items are documented on the left side of Table 1, which include the following issues: SL, ML, sacral sparing, complete/incomplete injury, AIS, NLI, zone of partial preservation and sensory and motor scores. The ML is further divided into three principles that are: (1) general principle, which is defined by the lowest key muscle function that has a grade of at least 3 (on supine manual muscle testing), providing the key muscle functions represented by segments above that level are judged to be intact (graded as 5);2 (2) consistent with SL (C1–C4, T2–L1 and S2–S5), that is, for those myotomes that are not clinically testable by a manual muscle exam, the ML is presumed to be the same as the SL if testable motor function above (rostral) that level is normal as well;2 and (3) C5 or L2 motor level: for these transitional levels, the motor level can be tested rather than being inferred from the SL, that is, if the C4 or L1 light touch (LT) and pin prick (PP) are both normal on the right or left side, then this is equivalent to the C4 or L1 motor being grade 5.2 In addition, the classification of AIS is categorized into items for definition from AIS A to AIS E, as well as an overall principle about determining motor incomplete status. In the booklet, the definitions of AIS C and D are marked with ‘**’, with the additional explanation: ‘For an individual to receive a grade of C or D, that is, motor incomplete status, they must have either (1) voluntary anal sphincter contraction or (2) sacral sensory sparing (at S4/5 or deep anal pressure [DAP]) with sparing of motor function more than three levels below the motor level for that side of the body’.2
After analyzing the clinical reasoning process of the five training cases of ISCICDS, the case number and the settings (admission and discharge) were matched with the corresponding items and listed on the right side of Table 1. For determining SL, three principles of ML, sacral sparing and complete/incomplete injury, there are at least two case scenarios involving each fact. For AIS, at least two case scenarios reflect the classification of AIS A and AIS B, and using sacral sensory sparing with sparing of motor function more than three levels below the ML for determining motor incomplete status, whereas only one case scenario for classification of AIS C and AIS D. However, there are no case scenarios for classification of AIS E and using voluntary anal sphincter contraction (VAC) for determining motor incomplete status. Although NLI is not documented directly in the data collection form of ISCICDS, it could be deduced from the SL and ML. Finally, none of the cases include information about zone of partial preservation, sensory or motor scores.
Discussion
The ISNCSCI provides a scheme that determines the severity and level of normal sensory and motor functioning.11 Among the items within the ISNCSCI, SL, ML and AIS are fundamental concepts through which the examiner can illustrate the basic neurological status for individuals with SCI. From the results of this analysis and comparison, we can conclude that the facts related to SL, ML and AIS are well reflected in the five training cases of ISCICDS.
From the result of a study using training cases for the ISNCSCI training by Schuld et al.,4 it is demonstrated that SL and completeness are easiest to rate, whereas ML and AIS are more difficult to determine. It is rather because the principles used in defining the SL and complete SCI are easy to understand. Despite this, it has to be emphasized that SL is determined on the basis of both PP and LT sensations. Although five case scenarios involved clinical reasoning about SL determination, only one scenario showed difference in level between PP and LT. From a retrospective review by Vasquez et al.,12 it is noticed that only in 30.3% instances LT and PP both indicated the same level of injury. Most frequently, PP alone determined the level. However, there is solely one case scenario reflecting this situation, hence it is suggested that in an update of the training cases, the clinical situation should be reflected in a more truthful manner.
As three principles should be used in defining the ML, it made ML more difficult to be accurately determined. Among the training cases of ISCICDS, six case scenarios test the fact of the general principle, the second and third case scenarios examine the ML consistency with SL, and the C5 or L2 ML issue, respectively. We do know that defining the ML in a patient with no correlating key motor function to test is a difficult concept to teach.13 Schuld et al.4 also reported most of the errors in ML determination that arise from SLs in the high cervical region (C2–C4), where by convention the ML is presumed to be the same as the SL. For determining ML in C5 or L2, a specific section was added in 200914 and then revealed in the 2011 revision of ISNCSCI1 to clarify this situation. Fortunately, all these three principles are expressed in the five training cases of ISCICDS.
Using the AIS based on the sensory and motor function of the sacral segments S4–S5 and the anorectal exam15 is now considered as the gold standard in grading the severity of SCI. In addition to the PP discrimination and LT sensation in the S4–S5 dermatome, sacral sparing also includes DAP and VAC during anorectal examination. When analyzing the five training cases of ISCICDS, there are four and two case scenarios describing AIS A and AIS B, whereas only one case scenario each reflecting AIS C and AIS D. Furthermore, these two scenarios of motor incomplete status are both determined through sparing of motor function more than three levels below the ML. Unfortunately, another principle, using VAC in determining motor incomplete status is not involved in the current cases. From the results of the previous studies,3, 4, 5 the most challenging fact and difficult step in AIS classification is the determination of motor incomplete injuries. It is proposed that more case scenarios related to motor incomplete status are warranted in an update of the training cases of ISCICDS. Moreover, a case scenario reflecting AIS E at discharge should be supplemented with the neurological status at discharge as it would not be relevant at admission.
According to the definition of NLI, it refers to the most caudal segment of the spinal cord with intact sensation and antigravity key muscle function strength, provided that there is normal (intact) sensory and motor function rostrally.2 Thus it is the highest level among the four levels (that is, right and left SL and ML). Although there is no training case in the ISCICDS that tests this concept, the clinical reasoning process of this fact could be thought to be involved in these cases as NLI could be deduced directly if needed. As zone of partial preservation, sensory score and motor score are not the components of ISCICDS, hence none of the training cases involve information about these concepts. Thus, the current training cases from ISCICDS should not be used in testing such specific facts. In addition, in previous studies16, 17, 18, 19 related to the test of the ISNCSCI, sensory score and motor score were more frequently investigated in clinical setting through examining the individual with SCI, rather than in virtual setting through using the training cases. It is because that determination of sensory and motor scores relies more on the assessments made at the physical examination, and not merely on observing and calculating assigned scores in training cases. Accordingly, to test the knowledge level of these items, it is preferable to examine individuals with SCI in clinical setting. At the same time, it is to be admitted that the purpose of the ISCICDS was not to include such knowledge as it was more the aim to document the minimal necessary information in relation to the SCI.
We do know that the International Standards Training e-Learning Program (InSTeP) was developed by American Spinal Injury Association in collaboration with ISCoS in 2010 aimed at training clinicians to perform accurate and consistent neurological examinations of individuals with SCI. The InSTeP is a six-module course including basic anatomy; sensory examination; motor examination; anorectal examination; scoring, scaling, the AIS classification; and a module on optional testing (http://lms3.learnshare.com/home.aspx). The fifth module of the InSTeP also includes five training cases for testing the effectiveness of training. These cases are presented with the scores reported in ISNCSCI worksheets. The InSTeP should be the preferred method in standardizing the use of the ISNCSCI. The intention is also to have InSTeP translated into multiple languages; unfortunately, it is in English only so far, hence its utilization in non-English-speaking setting may be difficult. In contrast, the ISCICDS is already translated into an official Chinese version, which as well is available from ISCoS website.9 Other official translations are in progress. In addition, we have to acknowledge that the technical and resource requirements to translate a document versus an interactive web course with video are substantially different, and therefore the utilization of the ISCICDS is an attractive alternative for those who have access to this kind of translations for testing the training effectiveness of the ISNCSCI until the InSTeP is translated into Chinese and other languages.
Conclusion
The majority of the facts related to SL, ML, and AIS are included in the five training cases of ISCICDS. Thus, using these training cases it is feasible to test the above facts within the ISNCSCI. However, the training cases of ISCICDS cannot be used for testing knowledge about zone of partial preservation, sensory score and motor score of ISNCSCI. Because these training cases are free to download and easy to access through the website of ISCoS, it is recommended to use them during the process of training the ISNCSCI. However, it is suggested that the clinical reasoning process about AIS E and using VAC for determining motor incomplete status should be included in an update of the training cases of ISCICDS, so that they could be more effective in testing the training effectiveness of the ISNCSCI.
Data Archiving
There were no data to deposit.
References
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A et al. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 2011; 34: 535–546.
American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury, revised 2011. Atlanta, GA. 2011.
Chafetz RS, Vogel LC, Betz RR, Gaughan JP, Mulcahey MJ . International standards for neurological classification of spinal cord injury: training effect on accurate classification. J Spinal Cord Med 2008; 31: 538–542.
Schuld C, Wiese J, Franz S, Putz C, Stierle I, Smoor I et al. Effect of formal training in scaling, scoring and classification of the international standards for neurological classification of spinal cord injury. Spinal Cord 2013; 51: 282–288.
Liu N, Zhou MW, Krassioukov AV, Biering-Sørensen F . Training effectiveness when teaching the international standards for neurological classification of spinal cord injury (ISNCSCI) to medical students. Spinal Cord 2013; 51: 768–771.
DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M, Stripling T et al. International spinal cord injury core data set. Spinal Cord 2006; 44: 535–540.
DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M, Stripling T et al. International spinal cord injury data set core data set. 2006 Available at http://www.iscos.org.uk/resources/sitefiles/PageFile_20_coredataset.pdf.
Biering-Sørensen F, Alexander MS, Burns S, Charlifue S, Devivo M, Dietz V et al. Recommendations for translation and reliability testing of international spinal cord injury data sets. Spinal Cord 2011; 49: 357–360.
Liu N, Zhou MW, Chen ZQ, Cao Y, Wang D . Chinese version of international spinal cord injury core data set. Available at http://www.iscos.org.uk/sitefiles/Chinese%20translation%20International%20SCI%20Core%20Data%20Set%20%20Version%201.0%20%20-%20%20incl.%20TRAINING%20Cases.pdf.
American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury, (Chinese translation: Zhou MW, Chen ZQ, Liu N) 7th edn People’s Medical Publishing House: Beijing, China. 2013.
Linassi G, Li Pi, Shan R, Marino RJ . A web-based computer program to determine the ASIA impairment classification. Spinal Cord 2010; 48: 100–104.
Vasquez N, Gall A, Ellaway PH, Craggs MD . Light touch and pin prick disparity in the international standard for neurological classification of spinal cord injury (ISNCSCI). Spinal Cord 2013; 51: 375–378.
Kirshblum SC, Waring W, Biering-Sorensen F, Burns SP, Johansen M, Schmidt-Read M et al. Reference for the 2011 revision of the international standards for neurological classification of spinal cord injury. J Spinal Cord Med 2011; 34: 547–554.
Waring WP 3rd, Biering-Sorensen F, Burns S, Donovan W, Graves D, Jha A et al. 2009 review and revisions of the international standards for the neurological classification of spinal cord injury. J Spinal Cord Med 2010; 33: 346–352.
Vogel L, Samdani A, Chafetz R, Gaughan J, Betz R, Mulcahey MJ . Intra-rater agreement of the anorectal exam and classification of injury severity in children with spinal cord injury. Spinal Cord 2009; 47: 687–691.
Savic G, Bergström EM, Frankel HL, Jamous MA, Jones PW . Inter-rater reliability of motor and sensory examinations performed according to American Spinal Injury Association standards. Spinal Cord 2007; 45: 444–451.
Mulcahey MJ, Gaughan J, Betz RR, Johansen KJ . The international standards for neurological classification of spinal cord injury: reliability of data when applied to children and youths. Spinal Cord 2007; 45: 452–459.
Marino RJ, Jones L, Kirshblum S, Tal J, Dasgupta A . Reliability and repeatability of the motor and sensory examination of the international standards for neurological classification of spinal cord injury. J Spinal Cord Med 2008; 31: 166–170.
Mulcahey MJ, Gaughan J, Betz RR . Agreement of repeated motor and sensory scores at individual myotomes and dermatomes in young persons with complete spinal cord injury. Spinal Cord 2009; 47: 56–61.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Liu, N., Hu, ZW., Zhou, MW. et al. Feasibility of using training cases from International Spinal Cord Injury Core Data Set for testing of International Standards for Neurological Classification of Spinal Cord Injury items. Spinal Cord 52, 919–922 (2014). https://doi.org/10.1038/sc.2014.141
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.141
