
Abstract
Background:
The high mechanical efficiency of the geared handcycle makes it suitable for elite athletes to train and even compete in races with able-bodied (recreational) cyclists. However, the actual exercise profile for endurance events has not been quantified.
Objective:
To guide future training regimes in a safe and effective process, the aim of this research was to quantify the workload, speed, cadence and heart rate parameters during 6000 km of training and within a 540 km ultra-long races.
Methods:
One spinal cord injured participant (lesion level Th4, ASIA B) handcycle (modified Shark S Sopur—Sunrisemedical, Malsch, Germany) was equipped with Schoberer Bike Measurement System (SRM) crank. For the laboratory test, a Cyclus II Ergometer was used. The energy intake and quality was determined during the time of race (540 km).
Results:
Workload at a defined metabolic situation was augmented through training by 63.8% from 90.0 to 147.6 W. The athlete finished the 540 km race with an average speed of 21.6 km h–1 and a total race time of 38:52 h.
Conclusions:
Ultra-long-term races in a handcycle can be suited by well-trained persons with a spinal cord injury. The quality of the training preparation time (for example, intensity and volume) is of immense importance to reach an adequate physiological capacity and to avoid serious injuries or medical problems.
Similar content being viewed by others


Introduction
A handcycle is a relatively new sports equipment that is a combination of the traditional wheelchair and a hand-operated bicycle crank.1 The high mechanical efficiency of this geared fixed-frame racing cycle in comparison with an manual wheelchair can potentially increase the distance a person with a loss of lower limb function can travel.2 To guide the optimal setup for the handcyclist the influence of crank length3, 4 and crank configuration5, 6 have been analyzed. The physiological profile of the handcyclist has also been studied,7, 8 and although this is often limited to investigations within the laboratory environment some studies have explored this relationship in competition.8, 9 In spite of the established relationship that a handcycle can improve the mechanical efficiency in long-term endurance, the actual exercise profile for long distance handcycling has not been quantified.
The bicycle race from Trondheim to Oslo has a long and important tradition in Scandinavia and for more than 40 years the route has provided an imposing challenge to riders of all abilities. Every year a wide range of cyclists rise to this challenge, from professionals aiming to finish the race in a target time of <14 h, to recreational riders trying to complete the race within the maximum possible time of 46 h. To reach the finish line in Oslo, cyclists must ride 540 km with an altitude increase of more than 4.2 km. Recently, an elite athlete with a traumatic spinal cord injury participated in this race using a handcycle, scientifically supervised by a sport science expert team. While other handcycling research has been limited to either able-bodied studies10 or sub-elite people with a disability populations,11 the athlete in this study is a multiple gold medallist, World Champion in wheelchair racing and European Champion in handcycling.
The aim of this study, therefore, was to generate unique and elite sport-specific training and race data. To guide future training regimes for elite handcyclists in a safe and effective process, this study quantified and analyzed the workload, speed, cadence and heart rate parameters during 6000 km of training, and within a 540 km ultra-long races. The energy intake and blood profile were also analyzed for the ultra-long race. This new knowledge can assist the safe preparation for other athletes with a lower limb disability competing in ultra-long handcycling distance events.
Materials and methods
Participants
After reviewing the procedures and possible risks associated with the investigation an elite male athlete with a long-lasting fourth thoracic vertebra spinal cord injury (ASIA B) provided written informed consent to participate. The athlete was not active in any sport before his spinal cord injury occurred. After his rehabilitation he was very successful in different wheelchair sport forms at an international level. The investigation was approved by the University's ethical advisory committee. All training sessions were planned and supervised by a sport science team. Data were collected during three different laboratory sessions, from 6000 km of outdoor training, and during the race in Norway. Training was organized as a 3:1 macro cycle with weeks of moderate long-lasting aerobic-orientated training (>300 km) followed by a more recreational training week (<200 km). In-between a training week there was a similar balance (3:1) between days with high training volumes (>3 h followed by a recreational training day (<1 h bike-specific training).12 The training intensities were defined using the lactate threshold defined by Heck and Mader.13 Workloads as a percentage of the intensity at a defined metabolic threshold (4 mmol l–1 lactate) were used to set training zones as recovery, extensive endurance, intensive endurance and intensive interval training. All training intensities excluding the intensive interval training are based on an in total aerobic use of carbohydrates and fatty acids.
Instrumentation
During the training period and the races, the following parameters were registered with Powercontrol by means of the Schoberer Bike Measurement System (SRM; eight resistance strain gauge; Schoberer, Jülich, Germany) and then transferred to a personal computer for further interpretation: (a) workload (W), (b) heart frequency (beats min–1), (c) speed (km h–1), (d) crank frequency (revolutions per minute) and (e) distance (km). The SRM system has been accepted to accurately measure these values.14 Before each training session and in each break during the race, the measurement system was calibrated following the instructions of the manufacturer.
Experimental procedure
To provide baseline data, five performance diagnostic tests were conducted in the laboratory on three different occasions during the training phase. These examinations included fasting blood test. To determine peak oxygen uptake incremental (starting at 20 W, increased by 20 W per 5 min) ergometer load tests were performed. To determine maximum power output and maximum oxygen uptake, an incremental (starting at 2 mmol l–1 lactate and increasing by 15 W per 15 s) ramp test was also conducted. Both tests were performed with the athlete's individual recumbent handcycle (modified Shark S Sopur—Sunrisemedical, Malsch, Germany), which was attached to a Cyclus II Ergometer (Avantronic Richter, Leipzig, Germany). The Cyclus II ergometer has been accepted to accurately measure workload.15 At least 2 h recovery was provided between each test. Before and after the race venous blood was taken, centrifuged for separation for serum and stored at −20 °C on site. Intermittently, blood sampling was conducted from the manually stimulated ear lobe to measure lactate concentration. The blood samples for determination of lactate concentration were cooled directly after collection, stored at −20 °C and were analyzed after the race (Biosen C-line; EKF, Magdeburg, Germany). Furthermore, food intake during the race was documented and interpreted using Prodi (Nutri-Science GmbH, Hausach, Germany). Regulation of exercise intensity as well as nutritional substitution during the competition was carried out by the athlete at his own discretion.
Data analysis
Descriptive statistics were presented as mean (s.d.) for workload, heart rate, speed, cadence and distance. A Pearson correlation for speed heart rate and workload over time was calculated using STATISTICA for Windows Version 5.1 F (StatSoft Inc., Tulsa, OK, USA). A P-value <0.05 was considered significant.
Results
The average training intensities orientated on the laboratory staged test were: 56.5% with intensity <2.6 mmol l–1 lactate (<60 W; 44% peak oxygen uptake), 10.2% in between 2.6 and 3.4 mmol l–1 lactate (60–80 W; 55% peak oxygen uptake), 23.6% in between 3.4 and 6 mmol l–1 lactate (80–105 W; 70% peak oxygen uptake), 9.7%>6 mmol l–1 lactate (>125 W; >73% peak oxygen uptake). The effectiveness of the training interventions is shown in Figure 1. Performance capacity at a lactate concentration of 4 mmol l–1 increased by 63.8% from 90.1 to 147.6 W (peak workload 180 W). Maximum oxygen uptake per kilogram body weight increased by 14.6% from 36.9 to 42.3 ml kg–1 at 240 W.

Workload at a defined metabolic situation in the course of the training periods.
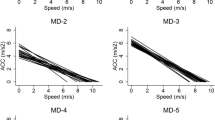
During the 540 km race, the athlete completed the race in 38:52 h with a net cycling time of 28:40 h. Average workload was 82.4±12.2 W corresponding to an average speed of 21.6±3.1 km h–1. In the course of the race, the competitor took 11 breaks lasting from 30 to 60 min. In the second night, after 470 km, a longer break of 3 h was required. Workload and heart rate showed a significant negative correlation over time (r=−0.75; r=−0.87). A poor and not significant negative correlation was found for speed over time (r=−0.37). Relevant workload, crank frequency and speed of the race are shown in Figure 2 and Table 1.

Cycling time, workload, crank frequency, speed and distance during the race.
The percentages of energy sources being used were: carbohydrates 76%, fat 17% and protein 7%. During the race, the athlete's food intake totalled 15 220 kJ, with 9.32 l of fluids consumed. The preferred mixture was 1 l water, 500 ml Red Bull and 82 g Power Gel with caffeine. There were some phases of nausea were the athlete could drink water only. In the course of the race, lactate concentrations were around 1.99–2.3 mmol l–1. These intensities are completely covered by an aerobic metabolism and reflect the intensities during >50% of all training kilometres. In Table 2, values of the blood count gained during the training period are listed. Owing to low ferritin and haemoglobin levels, the general practitioner who was responsible for the athlete's care administered intravenous iron (Ferrlecit, Sanofi-Aventis, Frankfurt, Germany). Creatine kinase (CK-MB) increased from 228 U l–1 directly before the race to 2026 U l–1 directly after the race.
Discussion
The higher mechanical efficiency of a handcycle has been previously established in the laboratory and from this study the training and ultra-long endurance profile for an athlete with a disability has now been assessed. The monitoring of workload, heart rate, speed, cadence and distance parameters during training and the 540 km race provide an interesting and applied sport profile. This new knowledge from actual competition of 38 h begins to address the existing void of information of what actually happens during an elite event. Furthermore, the increasing numbers of people with a spinal cord injury that are active in elite handcycling necessitate scientific knowledge to guide the safe preparation for training and competition. Valid results cannot be produced by using able-bodied participants or persons using the handcycle for leisure time activities.
Within the preparation phase for the race, the athlete could improve his performance capacity (W) at a defined metabolic level (4 mmol l–1 lactate) by approximately 63%. Although there always was a seasonal fluctuation in the athlete's capacity during the last 10 years, he never reached a comparable status as before the race in Norway. This extraordinary improvement in the athlete's physical performance capacity can be attributed to exercising predominantly at the recommended moderate intensity levels. The performance capacity values reached by the athlete were considerably high when compared with previously published values for athletes in a wheelchair.16, 17 Table 3 shows the relationship between the athlete's race performance and relevant published values in handcycling. It is clearly recommended to focus on elite athletes as participants as a scientific outcome for elite sport is required.
Fundamentally, the training regime generated an adequate performance capacity to successfully finish the race, and the recreational training volumes appear appropriate.12
The athlete's physical capacity has been measured for almost 10 years. In spite of the high lesion level of Th4 (ASIA B) no reduction in maximum heart rate was found (approximately 200 beats min–1). During all laboratory tests no event of autonomic dysreflexia occurred and the race data do not show signs of potential autonomic dysrefelxia situations. During the race no skin problems appeared although the long-lasting race with the athlete fixed in his handcycle for two nights and almost 2 days. Obviously in this case the lying position of the recumbent cycle allowed a well-balanced skin pressure distribution and avoided ulcers. Nevertheless during any ultra-long-term competition for persons with a spinal cord injury it is of great importance to take care of any skin problem.
From the nutrition perspective, the percentage of carbohydrates used as energy substrate was remarkably high.12, 18 No diarrhoea occurred in spite of the intake of carbohydrates added up to 75.6%, which is in contrast to other studies that reported problems with an carbohydrate intake of 65%.18 During the Norway race, the athlete experienced a hypocaloric and dehydration situation attributed to nausea during the second night. This situation forced the athlete into a longer resting period of approximately 3 h. Ultra-long distance sport is often associated with nausea.19 During the Norway race some additional factors were considered to cause this scenario, the composition of the fluids consumed, the low temperatures (−2 °C on the first night), and the long-term pressure from the abdominal belt used by the athlete to maintain stability within the handcycle.
The slightly reduced performance toward the end of the race was attributed to the energy demands from the first 170 km of the course, which were mainly uphill and the onset of fatigue showed by a negative correlation with workload, as well as heart rate over time. During this phase the athlete intentionally chose a high exercise intensity. Furthermore, 3 weeks before the Norwegian race the athlete set a new record for the 174 km distance in the handcycle race (average speed 33.5 km h–1) around Lac Leman, which could have negatively affected on his performance capacity. The noticeable low values of haemoglobin could be explained by abdominal problems that were treated by medical care after diagnosis in February 2006 (operation). Nevertheless, in comparison with athletes with spinal cord injury the athlete tends to show low values of haemoglobin.20
In spite of some temporary disorders with the wrists and the shoulders, which were treated by administering 75 mg Voltaren on two occasions, no further medical problems occurred during the race. The impressive increase in creatine kinase (CK-MB) (228 U l–1 vs 2026 U l–1) reflects the high effect of the race on the muscular system. Comparable results are shown for highly trained athletes directly after finishing an Ironman triathlon.21

References
Abel T, Kröner M, Vega S, Peters C, Klose C, Platen P . Energy expenditure in wheelchair racing and handbiking-a basis for prevention of cardiovascular diseases in those with disabilities. Eur J Cardiovasc Prev Rehabil 2003; 10: 371–376.
van der Woude LHV, Dallmeijer AJ, Janssen TW, Veeger D . Alternative modes of manual wheelchair ambulation: an overview. Am J Sports Med 2001; 80: 765–777.
Kramer C, Hilker L, Bohm H . Influence of crank length and crank width on maximal hand cycling power and cadence. Eur J Appl Physiol 2009; 106: 749–757.
Goosey-Tolfrey V, Alfano H, Fowler N . The influence of crank length and cadence on mechanical efficiency in hand cycling. Eur J Appl Physiol 2008; 102: 189–194.
Faupin A, Gorce P, Meyer C, Thevenon A . Effects of backrest positioning and gear ratio on nondisabled subjects’ handcycling sprinting performance and kinematics. J Rehabil Res Dev 2008; 45: 109–116.
Mossberg K, Willman C, Topor MA, Crook H, Patak S . Comparison of asynchronous versus synchronous arm crank ergometry. Spinal Cord 1999; 37: 569–574.
Haisma JA, van der Woude LH, Stam HJ, Bergen MP, Sluis TA, Bussmann JB . Physical capacity in wheelchair-dependent persons with a spinal cord injury: a critical review of the literature. Spinal Cord 2006; 44: 642–652.
Abel T, Schneider S, Platen P, Strüder H . Performance diagnostics in handbiking during competition. Spinal Cord 2005; 44: 211–216.
Abel T, Peters C, Platen P . Performance profile and health assessment of elite quad rugby players. Eur J Sport Sci 2003; 3: 1–7.
Faupin A, Gorce P, Campillo P, Thevenon A, Rémy-Néris O . Kinematic analysis of handbike propulsion in various gear ratios: Implications for joint pain. Clin Biomechanics 2006; 21: 560–566.
Valent LJ, Dallmeijer AJ, Houdijk H, Slootman HJ, Janssen TW, Post MW et al. Effects of hand cycle training on physical capacity in individuals with tetraplegia: a clinical trial. Phys Ther 2009; 89: 1051–1060.
Zaryski C, Smith DJ . Training principles and issues for ultra-endurance athletes. Curr Sports Med Rep 2005; 4: 165–170.
Heck H, Mader A, Hess G, Mucke S, Muller R, Hollmann W . Justification of the 4-mmol/l lactate threshold. Int J Sports Med 1985; 6: 117–130.
Paton CD, Hopkins WG . Ergometer error and biological variation in power output in a performance test with three cycle ergometers. Int J Sports Med 2006; 27: 444–447.
Reiser M, Meyer T, Kindermann W, Daugs R . Transferability of workload measurements between three different types of ergometer. Eur J Appl Physiol 2000; 82: 245–249.
Abel T, Schneider S, Platen P, Struder HK . Performance diagnostics in handbiking during competition. Spinal Cord 2006; 44: 211–216.
Janssen TW, Dallmeijer AJ, van der Woude LH . Physical capacity and race performance of handcycle users. J Rehabil Res Dev 2001; 38: 33–40.
Knechtle B, Bisig A, Schlapfer F, Zwyssig D . Energy metabolism in long-term endurance sports: a case study]. Schweiz Rundsch Med Prax 2003; 92: 859–864.
Peters EM . Nutritional aspects in ultra-endurance exercise. Curr Opin Clin Nutr Metab Care 2003; 6: 427–434.
Schumacher YO, Ruthardt S, Schmidt M, Ahlgrim C, Roecker K, Pottgiesser T . Total haemoglobin mass but not cardiac volume adapts to long-term endurance exercise in highly trained spinal cord injured athletes. Eur J Appl Physiol 2009; 105: 779–785.
Neubauer O, Konig D, Wagner KH . Recovery after an Ironman triathlon: sustained inflammatory responses and muscular stress. Eur J Appl Physiol 2008; 104: 417–426.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Abel, T., Burkett, B., Schneider, S. et al. The exercise profile of an ultra-long handcycling race: the Styrkeprøven experience. Spinal Cord 48, 894–898 (2010). https://doi.org/10.1038/sc.2010.40
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.40
Keywords
This article is cited by
-
Biomechanics of handcycling propulsion in a 30-min continuous load test at lactate threshold: Kinetics, kinematics, and muscular activity in able-bodied participants
European Journal of Applied Physiology (2020)
-
Physiological responses during simulated 16 km recumbent handcycling time trial and determinants of performance in trained handcyclists
European Journal of Applied Physiology (2020)
-
Kinematics and kinetics of handcycling propulsion at increasing workloads in able-bodied subjects
Sports Engineering (2018)
-
Lactate kinetics in handcycling under various exercise modalities and their relationship to performance measures in able-bodied participants
European Journal of Applied Physiology (2018)
-
Mountain time trial in handcycling: exercise intensity and predictors of race time in people with spinal cord injury
Spinal Cord (2014)
